Article Text

Statistics from Altmetric.com
HOME NIV AND REHABILITATION IN COPD
In contrast to the proven benefit of non-invasive ventilation (NIV) for the management of acute hypercapnic respiratory failure, there has been considerable controversy over the last 15 years or so about the use of home NIV in COPD patients with hypercapnic respiratory failure. This has been caused by conflicting results due to studies being of relatively small size, differing patient selection with varying outcomes measured and most performed over a limited time. There has also been some previous evidence that home NIV may be beneficial if added to exercise training. In this months’ Thorax. Duiverman and colleagues report a randomised study of home NIV added to a 3 month course of pulmonary rehabilitation or rehabilitation alone. The results show that the combined treatment produced improvements in several measures of quality of life, functional status and gas exchange though only over a 3 month study period. A considerable number of COPD patients are now being treated long term with home NIV and we are in need of large studies of home NIV in COPD, that are adequately powered for the desired outcomes and contain longer term follow up.
See pages 1052
RAGE IN ACUTE LUNG INJURY
Acute lung injury (ALI) is a major cause of acute respiratory failure and death in critically ill patients. The receptor for advanced glycation end products (RAGE) has been shown to be a new marker for alveolar type 1 cell injury and in this issue, Calfee and colleagues study whether plasma levels of RAGE are associated with severity and outcome in ALI. The study shows that higher baseline levels of RAGE were independently associated with worse outcomes, including higher mortality in patients given higher tidal volume ventilation. In the accompanying editorial, Griffiths and McAuley discuss the importance of a biomarker that can reflect the course of ALI and acute respiratory distress syndrome. They suggest that RAGE may be suitable, but its usefullness needs testing in a prospective longitudinal study.
See pages 1083
STATINS IN ASTHMA
There has been considerable recent interest in the anti-inflammatory properties of statins and in this month’s Thorax, Hothersall and colleagues report a randomised controlled crossover trial of atorvastatin added to inhaled corticosteroids in atopic asthma. Although there were falls in sputum macrophage count and sputum leucotriene B4 with the addition of the statin, there was no difference in clinical outcomes between the 2 study groups. The authors point out that the reduction observed in sputum macrophages suggests that atorvastatin may have a role in other chronic lung disease where there is evidence of activated alveolar macrophages such as COPD.
See pages 1070
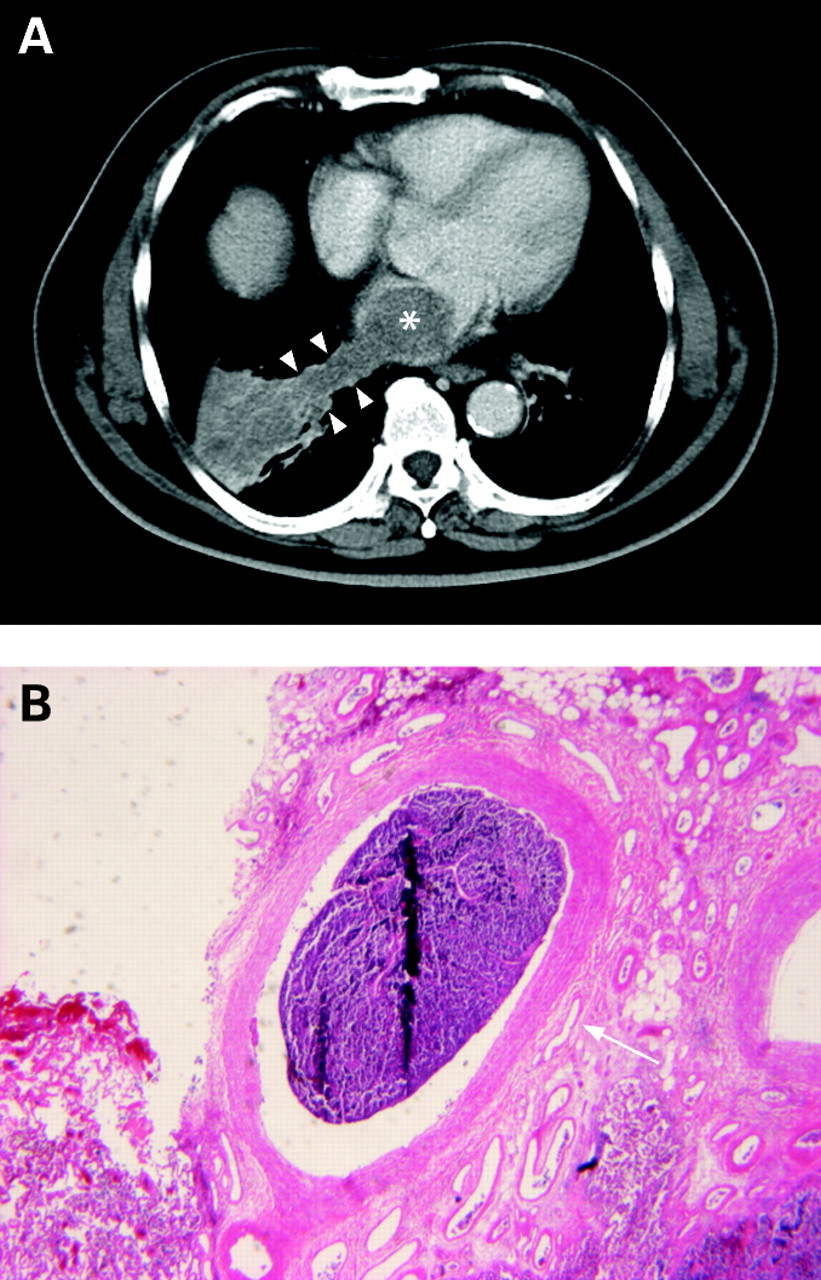
NON-SMOKERS WITH PIZZ
Severe alpha-1-antitrypsin (AAT) deficiency (PiZZ) is associated with early onset emphysema in individuals who are smokers. However there has been little information on the clinical course of non-smokers with PiZZ. In this issue, Tanash and colleagues report on the outcome of a large number of never-smokers with PiZZ selected from the Swedish National AAT Deficiency registry and followed for over 15 years. PiZZ non-smoking patients with respiratory symptoms, liver disease or other conditions had a higher mortality rate but patients identified from screening families did not have a high mortality risk compared to the Swedish general population. The authors also report a high risk of liver cirrhosis and liver carcinoma in elderly never smoking PiZZ subjects.
See pages 1091

{kind=link}
{kind=link}
Linked Articles
- Chronic obstructive pulmonary disease
- Acute lung injury
- Asthma
- Alpha-1-antitrypsin deficiency
- Images in Thorax
- Miscellaneous