Article Text

Statistics from Altmetric.com
Ventilation inhomogeneity, measured using multiple breath washout (MBW), reflects small airway function and has emerged as a valuable tool in cystic fibrosis (CF). Improved sensitivity to detect early lung damage has been suggested from preschool children through to adults and confirmed in high-resolution CT (HRCT) studies.1 Longitudinal utility is now emerging.2 A large number of parameters reflecting overall ventilation inhomogeneity have been proposed, but consensus is lacking about the optimal parameter to report.
The two most commonly reported are lung clearance index (LCI) and moment ratios (MR). LCI, the easier to calculate and understand conceptually, represents the number of lung turnovers (or functional residual capacities, FRC) required to reduce the end tidal inert gas concentration to 1/40th of its starting value. The calculation of MR adds more weight to the latter portion of the washout curve and, while more complicated in their derivation, offer improved robustness to variations in tidal volume (Vt)3 and potentially improved sensitivity.4 5 Truncation of MR to facilitate comparison between subjects is recommended.6 In practice, however, the large Vt fluctuations used by Saidel et al3 are beyond that seen during routine MBW tests, which encourage regular tidal breathing. The derivation of these parameters is described in more detail in the online supplement.
MBW tests from two cohorts, a CF (n=56) and a healthy control (n=32), containing preschool children through to adults were retrospectively studied. Testing, performed in triplicate with results averaged, took place at the West-Swedish CF Centre, Göteborg, Sweden using equipment previously described.7 In children a regular spontaneous breathing pattern was targeted, while an adult protocol was used in older subjects.8 Spirometry was performed according to ATS criteria and z-scores were generated from appropriate Swedish reference values. LCI and MR results from the healthy cohort generated upper limits of normality. Prism Version 4.0 (GraphPad Software, San Diego, USA) was used for statistical analyses: t tests were used for parametric continuous variables, the Mann-Whitney test for non-parametric continuous variables and multivariate logistic regression analyses to investigate factors influencing the within-subject coefficient of variation (CV) of MBW indices from the triplicate tests. Data were pooled from previous studies with ethics approval, and some of the LCI CF data have been previously reported.9
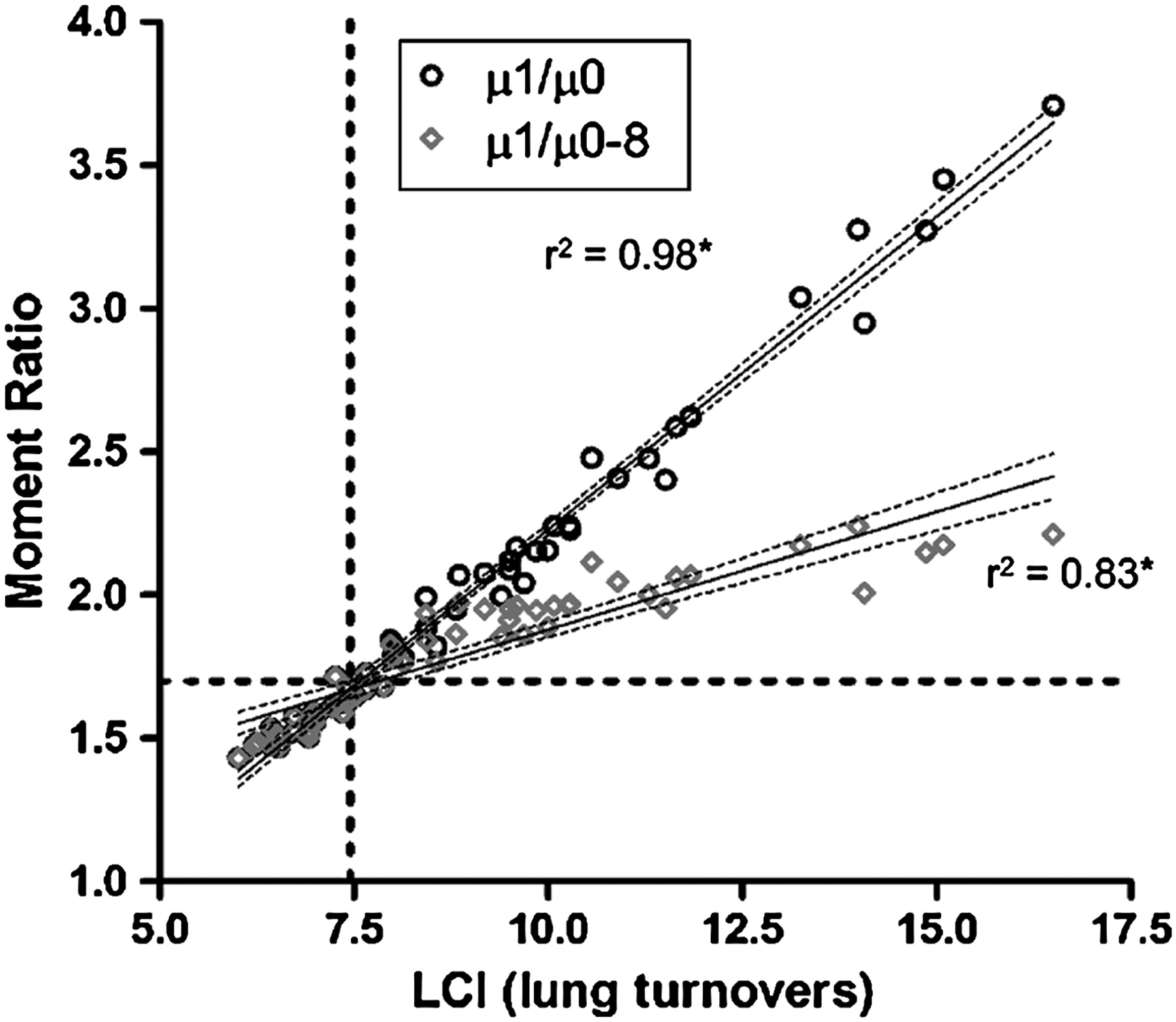
The demographic characteristics of the two groups are summarised in table 1 of the online supplement. MBW indices were significantly raised in the CF cohort compared with controls: LCI 9.03 (2.51) vs 6.28 (0.58); µ1/µ0 2.01 (0.55) vs 1.45 (0.12); and µ2/µ0 6.59 (3.76–30.4) vs 3.85 (2.96–5.43), all p<0.001 (see table 2 in the online supplement). Comparable sensitivity was seen between parameters and was not affected by truncation of MR. No significant difference in CV was seen between LCI and µ1/µ0 in either cohort, but was significantly greater for µ2/µ0 in both (p<0.001). Truncation of MR improved the CV in the CF cohort (table 3 in online supplement). Variation in breathing parameters (respiratory rate (mean, CV), Vt (CV), or Vt/FRC) did not explain the variation in CV seen between the indices. Correlation was strong between LCI and both MR parameters in the CF cohort but negatively affected by truncation at higher LCI values (figure 1) (see also figure 1 in online supplement).

{kind=link}
Correlation between lung clearance index (LCI) and the first moment ratio in its untruncated (µ1/µ0) and truncated forms (µ1/µ0–8). *p<0.001.
While MR truncation improved stability and did not affect sensitivity, a negative effect on the relationship with LCI was seen at higher LCI values, potentially affecting sensitivity and utility in more severe disease. Given the frequency of higher LCI values reported in established CF lung disease2 and its comparable sensitivity and stability to µ1/µ0, this easily derived and simple to understand index should be the preferred longitudinal assessment outcome parameter of ventilation inhomogeneity reported in future CF studies.
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; not externally peer reviewed.