Article Text

Abstract
Current data relating to ventilation in ARDS are reviewed. Recent studies suggest that reduced mortality may be achieved by using a strategy which aims at preventing overdistension of lungs.
- acute respiratory distress syndrome
- acute lung injury
- ventilation
- critical care
Statistics from Altmetric.com
The ventilatory management of patients with acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) has evolved in conjunction with advances in understanding of the underlying pathophysiology. In particular, evidence that mechanical ventilation has an influence on lung injury and patient outcome has emerged over the past three decades.1 The present understanding of optimal ventilatory management is outlined and other methods of respiratory support are reviewed.
PATHOPHYSIOLOGY
The pathophysiology of ARDS has been reviewed by Bellingan in an earlier article in this series.2 However, it is useful to highlight important features relevant to ventilatory management, in particular the anatomical distribution of pulmonary pathology and the potential for ventilator induced lung injury.
The original description of ARDS included the presence of bilateral infiltrates on the chest radiograph.3 Since the 1980s considerable research has been undertaken using computerised tomographic (CT) scanning which has shown that parenchymal consolidation, far from being evenly distributed, is concentrated in dependent lung regions leaving non-dependent lung relatively spared. This pathological distribution of aerated lung lying over areas of dense consolidation has led to comparisons with ventilation of a much smaller or “baby lung”4 and has important implications for ventilatory management. Thus, the application of normal physiological tidal volumes can lead to overdistension of the small volume of normally aerated lung, while failing to recruit consolidated dependent regions.
Ventilator induced lung injury5 can occur by several mechanisms: oxygen toxicity from the use of high Fio2,6 overdistension of the lung causing barotrauma and further inflammation,7 injurious cyclical opening and closing of alveoli from ventilation at low lung volumes,8 and by increasing systemic levels of inflammatory cytokines.9
Ventilatory strategies must therefore be tailored to minimise the risk of inducing or exacerbating further lung injury.
RESPIRATORY MECHANICS
Decreased lung compliance is a prominent feature of ARDS. The static compliance of the respiratory system (lung + chest wall) in a ventilated patient is calculated by dividing the tidal volume (Vt) by end inspiratory plateau pressure (Pplat) minus end expiratory pressure + intrinsic PEEP (PEEPi). As the pathology of ARDS is heterogeneous, calculating static compliance does not provide information about regional variations in lung recruitment and varies according to lung volume. Much attention has therefore focused on analysis of the pressure-volume (PV) curve.
The static PV curve of the respiratory system can be obtained by inserting pauses during an inflation-deflation cycle. A number of different methods have been described including the use of a large syringe (super-syringe), or holding a mechanical ventilator at end inspiration of varying tidal volumes. The principles and methods of PV curve measurement have recently been reviewed.10
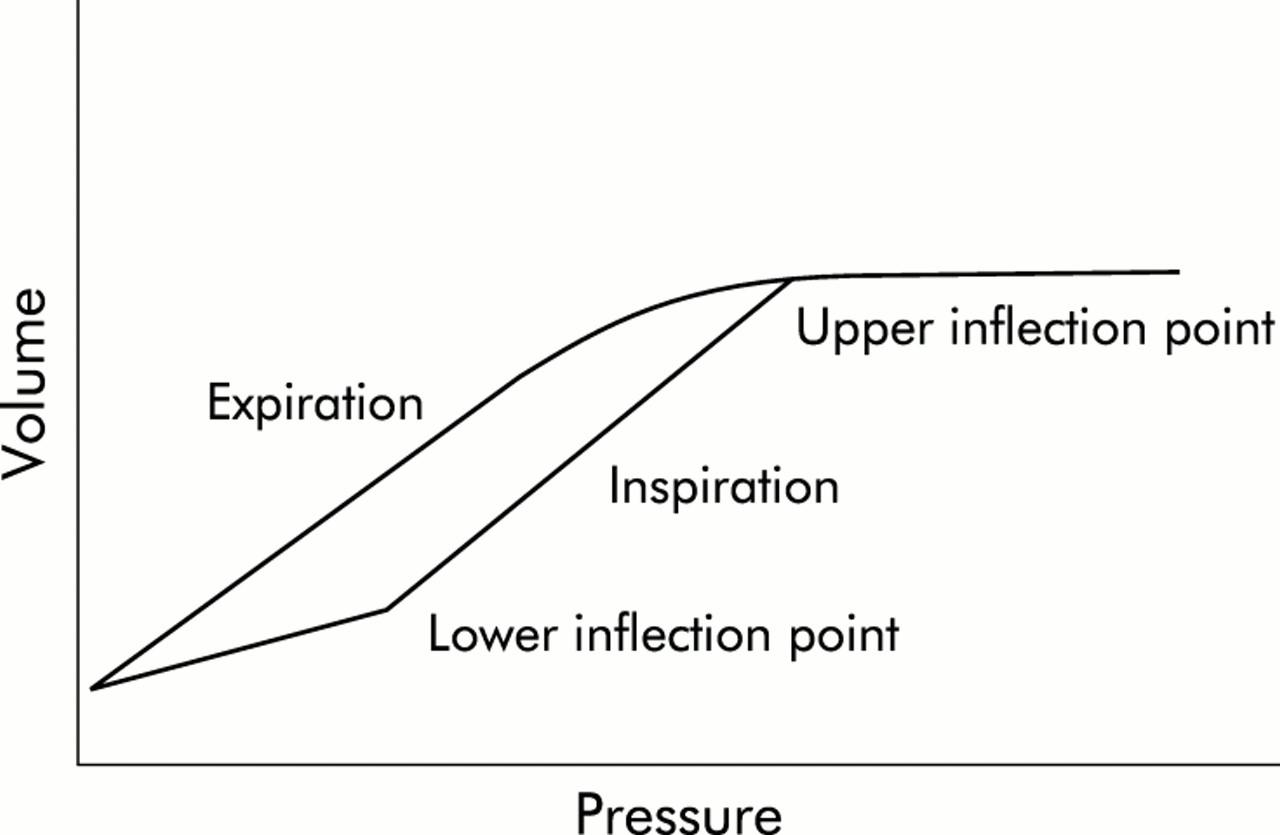
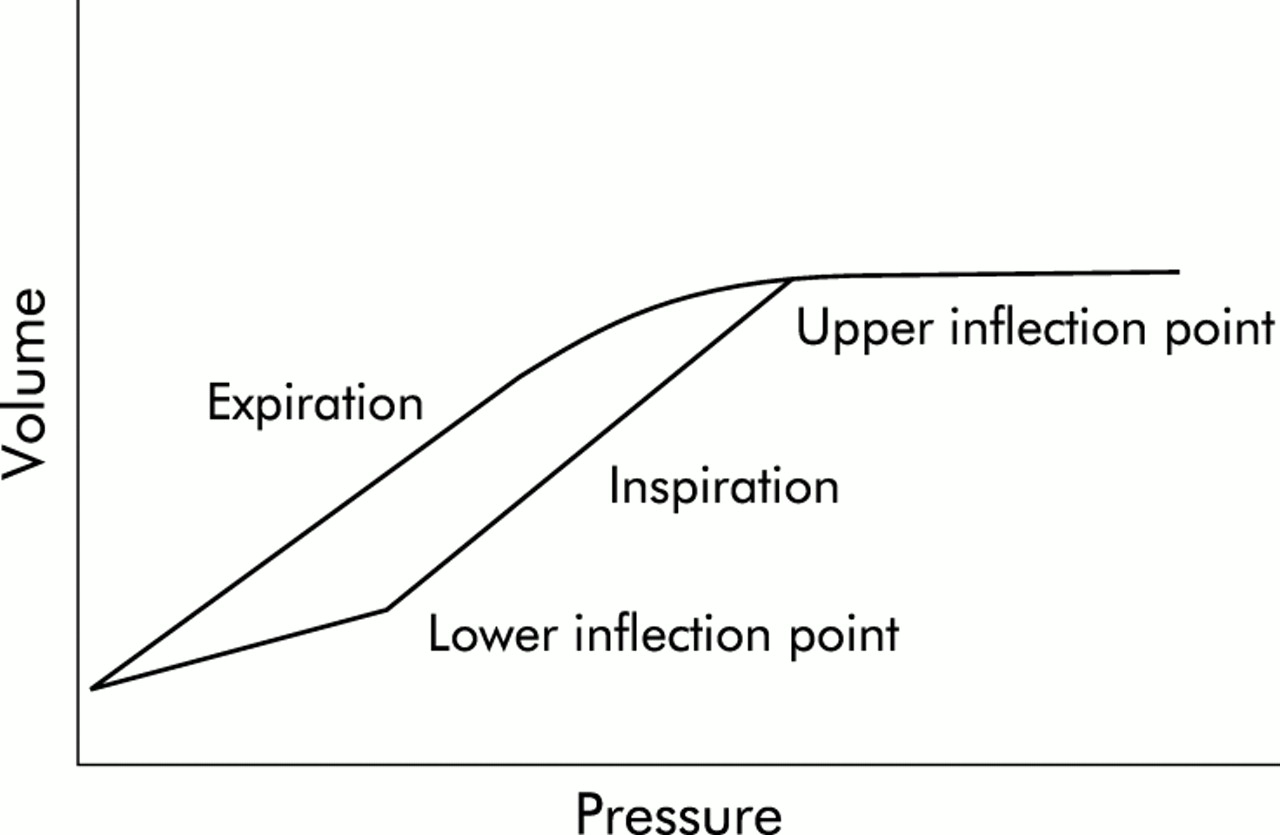
The PV curves thus obtained are sigmoidal and have an inspiratory limb that usually includes a point above which the curve becomes steeper (fig 1).4 Identification of the lower inflection point by clinicians using PV curves is subject to large variability, but is improved by curve fitting.11 In some patients the lower inflection point may be absent. At higher lung volumes the curve becomes flatter again (upper inflection point), above which further increases in pressure cause little increase in volume. Currently, ventilators used routinely in intensive care units do not have automated functions to obtain a static PV curve. Moreover, the static PV curve only provides information about accessible lung4 and also includes chest wall compliance. Separating the lung and chest wall components requires the use of oesophageal pressure measurement.12
{kind=link}
Schematic representation of a static pressure-volume curve of the respiratory system from a patient with ARDS. Note the lower and upper inflection points of the inspiratory limb.
Despite these limitations, many advances in clinical management in patients with ALI/ARDS have been based on consideration of static PV curves. More recently it has been proposed that analysis of the inspiratory pressure-time curve under conditions of constant flow can provide useful information about lung recruitment.13
VENTILATORY STRATEGIES IN ARDS
The goals of ventilating patients with ALI/ARDS should be to maintain adequate gas exchange and avoid ventilator induced lung injury.
Maintenance of adequate gas exchange
Oxygen
High concentrations of inspired oxygen should be avoided to limit the risk of direct cellular toxicity and to avoid reabsorption atelectasis. Arterial oxygen saturation (Sao2) is used as a target in preference to arterial oxygen tension (Pao2) in recognition of the fact that oxygen delivery is the important determinant of tissue oxygenation. Sao2 values of around 90% are commonly accepted but oxygen delivery decreases quickly below 88% because of the shape of the oxyhaemoglobin dissociation curve. However, if a higher Sao2 can only be obtained by increasing airway pressure to levels that result in haemodynamic compromise, lower Sao2 may have to be accepted.
There is no clinical evidence to support the use of specific Fio2 thresholds, but it is common clinical practice to decrease Fio2 below 0.6 as quickly as possible.
Oxygenation can be improved by increased alveolar recruitment through the application of higher airway pressure provided that ventilation-perfusion (V/Q) matching is not adversely affected by the haemodynamic consequences of increased intrathoracic pressure. Lung recruitment is usually obtained by applying extrinsic PEEP, increasing the inspiratory:expiratory (I:E) ratio, or by specific recruitment manoeuvres (discussed below).
Carbon dioxide
Limiting tidal volume and peak pressure to reduce ventilator induced lung injury may cause hypercapnia. Strategies used to manage hypercapnia have included increasing tidal volume and airway pressure, or increasing CO2 removal with techniques such as tracheal gas insufflation or extracorporeal CO2 removal. In 1990 it was reported that the alternative of simply allowing CO2 to rise to a higher level (permissive hypercapnia) and maintaining limits on tidal volume and airway pressure was associated with a significantly lower than predicted mortality from ARDS.14
The physiological consequences of hypercapnia are respiratory acidosis, increased cardiac output, and pulmonary hypertension. Neurological changes include increased cerebral blood flow, and cerebral oedema and intracranial haemorrhage have been reported.15 With severe acidosis there may be myocardial depression, arrhythmias, and decreased response to exogenous inotropes. Renal compensation of the respiratory acidosis occurs slowly.
Unfortunately there are no data to confirm the degree of respiratory acidosis that is safe. Recent studies (discussed below) have allowed hypercapnia as part of lung protective ventilatory protocols. 1,16–19 Arterial pH was lower in the lung protective groups and the ARDSNet study included the use of sodium bicarbonate to correct arterial pH to normal.1 At present no recommendations can be made concerning the management of respiratory acidosis induced by permissive hypercapnia. However, if bicarbonate is infused, it should be administered slowly to allow CO2 excretion and avoid worsening of intracellular acidosis.
One method used to increase CO2 clearance is insufflation of gas into the trachea to flush out dead space CO2 and reduce rebreathing.20 Tracheal gas insufflation has been used both continuously and during expiration only. As no commercially available ventilator includes this technique, modifications are required to the ventilator circuit and settings to prevent inadvertent and potentially dangerous increases in intrinsic PEEP, Vt, and peak airway pressure.
In adult patients with ARDS, managed using pressure control ventilation, the introduction of continuous tracheal gas insufflation allowed a decrease in inspiratory pressure of 5 cm H2O without increasing arterial carbon dioxide tension (Paco2).21 Tracheal gas insufflation may therefore be useful when permissive hypercapnia is contraindicated. However, managing the appropriate ventilator settings and adjustment is complicated, with real potential for iatrogenic injury.
In practice, Paco2 is allowed to rise during lung protective volume and pressure limited ventilation. Paco2 levels of 2–3 times normal seem to be well tolerated for prolonged periods. Renal compensation for respiratory acidosis occurs over several days. Many clinicians infuse sodium bicarbonate slowly if arterial pH falls below 7.20.
Avoidance of ventilator induced lung injury
Traditional mechanical ventilation (as applied during routine general anaesthesia) involves tidal volumes that are relatively large (10–15 ml/kg) in order to reduce atelectasis. PEEP levels are adjusted to maintain oxygenation but high levels are generally avoided to prevent cardiovascular instability related to increased intrathoracic pressure. Present understanding of ventilator induced lung injury suggests that traditional mechanical ventilation, using high tidal volumes and low PEEP, is likely to enhance lung injury in patients with ARDS. Five randomised studies of “lung protective” ventilation in ARDS have recently been published, four of which investigated limitation of tidal volume to prevent injury from overdistension (table 1).
Randomised prospective studies of ventilatory strategies to limit lung overdistension in patients with ARDS
In these studies the protective ventilatory strategy was directed at preventing lung overdistension and was not designed to look at differences in ventilation at low lung volumes. Only the largest study (ARDSNet)1 showed an advantage of such a protective strategy. The ARDSNet study had the largest difference in Vt and Pplat between the groups, the highest power, and was the only study to correct respiratory acidosis (table 2).
Protective lung ventilation protocol from the ARDSNet study1
Others studies have addressed the issue of adjustment of ventilatory support based on PV curve characteristics. Amato et al randomised 53 patients with early ARDS to either traditional ventilation (volume cycled, Vt 12 ml/kg, minimum PEEP guided by Fio2, normal Paco2) or a lung protective strategy (PEEP adjusted to above the lower inflection point of a static PV curve, Vt <6 ml/kg, permissive hypercapnia, and pressure limited ventilatory mode with PIP limited to <40 cm H2O).19 Patients in the lung protective group had improved indices of oxygenation, compliance, and weaning rates. Mortality in the traditional ventilation group was worse at 28 days (71% v 45%, p<0.001) and hospital discharge (71% v 45%, p=0.37). By using the static PV curve to adjust PEEP in the protective ventilation group, this study also addressed the issue of ventilator induced damage by cyclical opening and closure of alveoli. The hospital mortality was lower, but not significantly, in a small group of patients. However, mortality was very high in the traditional ventilation group, making this study difficult to interpret. Further clinical investigation into the role of higher levels of PEEP in combination with recruitment manoeuvres is currently being undertaken by the ARDS Net group.
Pressure and volume limited ventilation
Invasive ventilation of adult patients in the intensive care setting has traditionally been provided by delivering a set tidal volume at a set rate and inspiratory flow. This technique has the advantage of maintaining a constant minute volume and Paco2 under conditions of changing respiratory system compliance providing that preset limits of airway pressure are not reached. Another strategy that has been used increasingly over the last 10 years is to use pressure controlled ventilation in which a decelerating inspiratory flow profile is applied to a set pressure limit. Changes in compliance during pressure control ventilation will result in variable minute volume and Paco2, but this mode has the advantage of limiting pressure to a set level. More sophisticated mechanical ventilators have allowed adjustment of more parameters in each mode and have made the distinction between these two types of ventilation blurred. Studies of volume versus pressure controlled ventilation in ARDS have been reported but have been too small to detect any important outcome differences.22–24 The largest study of ventilation in ARDS reported an outcome difference between the two protocols using volume controlled ventilation, suggesting that settings rather than the mode is the important issue.1
Whatever mode of ventilation is used, it is now clear that tidal volume should be set in the region of 6 ml/kg rather than the traditional 10–12 ml/kg and the peak pressure should be limited to 30–35 cm H2O to prevent lung overdistension—that is, inspiration should be terminated before the upper inflection point on the PV curve.
PEEP
The application of PEEP improves oxygenation by providing movement of fluid from the alveolar to the interstitial space, recruitment of small airways and collapsed alveoli, and an increase in functional residual capacity (FRC). In addition, cyclical collapse and low volume lung injury is prevented. Increased Pao2 induced by PEEP was found to be correlated with the volume of lung recruited.25
In theory, setting PEEP above the lower inflection point may prevent derecruitment and low lung volume ventilator associated injury. As discussed above, adjusting the level of PEEP to 2 cm H2O above the lower inflection point was part of a lung ventilatory strategy that was advantageous.19 The ARDS Network is currently conducting a randomised trial to identify optimal PEEP.
It has been suggested that the effect of PEEP on recruitment in ARDS varies according to the regional distribution of consolidation. In a study employing CT scanning, patients were divided into groups according to the distribution of consolidation (lobar, diffuse, or patchy CT attenuations).26 PEEP had little effect on lobar consolidation but induced the greatest reduction in non-aerated lung in patients with diffuse CT abnormalities. Current clinical practice in the absence of routine static PV curve measurement is to set PEEP at a relatively high level such as 15 cm H2O in patients with ARDS.
Inspiratory time
Prolongation of the inspiratory time with an increased I:E ratio is commonly used as a method of recruitment. Mean airway pressure is increased. Shortening of expiratory time can cause hyperinflation and the generation of intrinsic PEEP (PEEPi). Providing that ventilation is pressure limited, PEEPi can be manipulated to increase recruitment further. In volume control modes of ventilation without pressure limitation, PEEPi levels can increase to dangerous levels causing lung overdistension and haemodynamic compromise. No clinical outcome studies have specifically addressed inspiratory time or levels of PEEPi. It is common practice during pressure control ventilation to increase the I:E ratio to 1:1 or 2:1 (inverse ratio ventilation) with close monitoring of PEEPi and haemodynamics.
Recruitment manoeuvres
There has been renewed interest recently in manoeuvres aimed at increasing alveolar recruitment following the recognition that higher levels of PEEP are necessary to sustain any benefit obtained by such manoeuvres, and that any sudden reduction such as ventilator disconnection for suctioning leads to derecruitment.
The sigh function involves the delivery of intermittent breaths of larger tidal volume, administered either via the mechanical ventilators or by hand. Sighs delivered to patients with ARDS increase alveolar recruitment but the benefit is short lived, lasting less than 30 minutes.27 The same authors also suggest that secondary ARDS (ARDS as a result of non-pulmonary disease) is more responsive to sighs than primary ARDS.
Sustained inflation or continuous positive airway pressure (CPAP) is another form of recruitment manoeuvre. Several investigators have reported the effects of different manoeuvres in patients with ARDS (table 3).
Reported lung recruitment manoeuvres
Recruitment manoeuvres may be more effective in patients ventilated with relatively low levels of PEEP. Conversely, they may be less effective and cause lung overdistension in patients with already optimally recruited lungs—that is, with higher levels of PEEP. Recruitment manoeuvres all involve increasing intrathoracic pressure and therefore the risk of barotrauma and cardiovascular instability. At present there are no published data from randomised studies to indicate whether recruitment manoeuvres, of whatever form, influence outcome.
Spontaneous breathing during positive pressure ventilation (BiPAP, APRV)
Two modes of ventilation commonly available on mechanical ventilators—biphasic airway pressure (BiPAP) and airway pressure release ventilation (APRV)—allow spontaneous breathing to occur at any stage of the respiratory cycle. In these modes the ventilator cycles between an upper and lower pressure at preset time intervals. Spontaneous breathing during mechanical ventilation decreases intrathoracic pressure and improves V/Q matching and cardiac output.28 These theoretical benefits have resulted in more widespread use of the BiPAP mode, which provides a range of I:E ratios (APRV applies a very short expiratory time), but again no data exist concerning any influence on outcome.
PRONE VENTILATION
Prone position was reported to improve oxygenation in patients with ARDS as long ago as 1976.29 The mechanism of the improvement in oxygenation on turning prone, seen in about two thirds of patients with ARDS, is complex. The intuitive explanation that regional lung perfusion is primarily dependent on gravity leading to improved perfusion of non-consolidated lung on turning is not substantiated by research. In fact, perfusion to dorsal lung regions predominates whatever the patient’s position,30 and gravity accounts for less than half the perfusion heterogeneity seen in either the supine or prone position.31 Changes in regional pleural pressure are more important. The gradient of pleural pressure from negative ventrally to positive dorsally in the supine position is not completely reversed on turning prone, so that the distribution of positive pressure ventilation is more homogenous in the prone position.32 Thus, recruitment of dorsal lung appears to be the predominant mechanism of improved oxygenation.
Potential problems of prone positioning are increased venous pressure in the head (facial oedema), eye damage (corneal abrasions, retinal and optic nerve ischaemia), dislodgment of endotracheal tubes and intravascular catheters, and increased intra-abdominal pressure.
A multicentre prospective randomised study of the prone position for adult patients with ARDS has recently been completed in Italy.33 Patients randomised to prone positioning were assessed daily for the first 10 days and turned prone for at least 6 hours if severity criteria were met. There were no differences in clinical outcome.
Prone positioning is a useful adjunct to ventilation and may help to improve oxygenation and pulmonary mechanics but, as yet, has not been shown to alter outcome in ARDS.
HIGH FREQUENCY VENTILATION
There has been a resurgence of interest in high frequency ventilation (HFV, rate >60/min) over the last few years. Initial enthusiasm had been tempered by practical difficulties and the lack of clinical outcome data showing any advantage over conventional mechanical ventilation. The recent clinical studies of conventional ventilation demonstrating the advantages of limited Vt and maintenance of lung volume have helped to promote interest in HFV. The very low Vt (1–5 ml/kg) provided by HFV offers the possibility of maintaining lung volume at a higher point on the PV curve with less risk of causing overdistension.34 High frequency jet ventilation (HFJV) and high frequency oscillatory ventilation (HFOV) have been the two most commonly used methods used to ventilate patients in the intensive care unit.
High frequency jet ventilation (HFJV)
High frequency jet ventilation uses a high pressure gas jet delivered into an endotracheal tube at high frequency (100–200 Hz). Other gas in the ventilator circuit is entrained producing a Vt of 2–5 ml/kg that can be adjusted by altering the inspiratory time and/or driving pressure. During HFJV, expiration occurs passively. Practical problems encountered are inadequate humidification, potential for gas trapping, difficulty in adjusting ventilator settings, and the need for a specialised endotracheal tube.
HFJV has been investigated in two large prospective randomised studies. In a study of 309 patients being ventilated for different causes of respiratory failure, the use of HFJV resulted in no significant outcome differences.35 Similarly, a study of 113 patients at risk of ARDS had similar clinical outcomes in both patients ventilated conventionally and in those in whom HFJV was used.36 These studies did not include recruitment manoeuvres that are now recognised to be important37 and were underpowered with respect to clinical outcomes such as mortality.38
High frequency oscillatory ventilation (HFOV)
High frequency oscillatory ventilation differs from HFV in a number of important aspects. Tidal volume (1–3 ml/kg) is generated by the excursion of an oscillator within a ventilator circuit similar to that used for CPAP and is varied by altering the frequency, I:E ratio, and oscillator amplitude. The use of an oscillator to generate Vt results in active expiration. Mean airway pressure is adjusted by altering the fresh gas flow (bias flow) into the circuit or the expiratory pressure valve. Oxygenation is controlled by altering mean airway pressure or Fio2.
On initiation of HFOV, lung recruitment is achieved by increasing mean airway pressure and monitoring arterial oxygenation. Once optimal recruitment has occurred, mean airway pressures are reduced, taking advantage of the hysteresis of the lung pressure-volume relationship in order to prevent alveolar overdistension. This process needs to be repeated after each episode of derecruitment.38
HFOV has been used extensively in neonates, and studies suggest that it is associated with a lower incidence of chronic lung disease than conventional ventilation.39 HFOV (with a recruitment protocol) was compared with conventional mechanical ventilation in 70 paediatric patients with respiratory failure secondary to diffuse alveolar disease or large air leaks using a crossover (for treatment failure) study design.40 Overall outcomes were similar with the exception that patients randomised to HFOV had a lower requirement for supplemental oxygen at 30 days. After subgroup analysis, mortality was lower in patients treated with HFOV than in those treated with conventional mechanical ventilation only (6% v 40%).
There are few data on the use of HFOV in adult patients. In an observational study of 17 patients with ARDS, HFOV was reported to be effective and safe.41 A multicentre prospective randomised study of HFOV compared with conventional mechanical ventilation is currently underway (Multicenter Oscillator ARDS Trial (MOAT 2)).
LIQUID VENTILATION
ARDS is associated with loss of surfactant, a consequent rise in surface tension, and alveolar collapse. Filling the lung with liquid removes the air-liquid interface and supports alveoli, thus preventing collapse. Perfluorocarbons have been used in this approach because they have low surface tension and dissolve oxygen and carbon dioxide readily.
Total liquid ventilation involves filling the entire lung with liquid and using a special ventilator to oxygenate the perfluorocarbon, a technique that is both difficult and expensive. Partial liquid ventilation is a much more practical alternative. The lung is filled to FRC with liquid and ventilated with a conventional mechanical ventilator. Although partial liquid ventilation has been shown to be practical and safe, no randomised prospective studies against conventional management have yet been published.42 Further information on liquid ventilation can be obtained from a recent review by Leonard.43
OTHER RESPIRATORY SUPPORT
Inhaled vasodilators
The use of inhaled vasodilators in patients with ALI/ARDS will be described in a later article in this series by Cranshaw et al44 and will not be discussed further here.
Extracorporeal gas exchange
During extracorporeal membrane oxygenation (ECMO) venous blood is removed via a cannula in the inferior vena cava or right atrium, passed through a heart/lung machine, and is returned to either the right atrium (veno-venous bypass) or aorta (veno-arterial bypass). In veno-venous bypass, pulmonary and systemic haemodynamics are maintained by the patient’s own cardiovascular function. Veno-arterial bypass allows systemic haemodynamic support as well as gas exchange. Institution of ECMO allows ventilator pressures and volumes to be decreased to prevent further ventilator induced lung injury. In addition, the reduction in intrathoracic pressure allows fluid removal to be carried out with less risk of haemodynamic instability. A pumpless form of extracorporeal gas exchange using arteriovenous cannulation has recently been described.45
ECMO has proven mortality benefit in neonatal ARDS. In adults a single prospective randomised study failed to show a survival advantage over conventional support.46 However, overall survival in both groups was extremely low and the results are not applicable to current practice. Extracorporeal CO2 removal (ECCOR) involves use of an extracorporeal veno-venous circuit with lower blood flows and oxygenation still occurring via the patient’s lungs. A randomised prospective study of ECCOR compared with conventional support in patients with severe ARDS reported no significant difference in survival.47 Several centres have recently reported observational studies showing high survival rates in adult patients managed with extracorporeal support (table 4). These encouraging survival rates should be interpreted, however, in the context of improved survival without ECMO.48,49 A randomised prospective controlled study of ECMO in adult patients is currently underway in Leicester, UK.
Recent observational studies reporting survival of patients with ARDS managed with extracorporeal membrane oxygenation (ECMO)
CONCLUSION
The current data relating to conventional ventilation in ARDS suggest that high tidal volumes (12 ml/kg) with high plateau pressure (more than 30–35 cm H2O) are deleterious and that a strategy aimed at preventing overdistension by decreasing tidal volume to 6 ml/kg and limiting plateau pressure to <30 cm H2O is associated with lower mortality.50 In addition, ventilation directed at preventing cyclical opening and closing of alveoli by adjusting PEEP according to the PV curve to maintain recruitment may have a role in preventing lung injury and further studies are underway to clarify this issue. There may also be a role for recruitment manoeuvres, particularly after episodes of derecruitment. High frequency ventilation, including a recruitment protocol, may offer the ultimate lung protective ventilation, but further clinical studies are required.