Article Text

Abstract
BACKGROUND The effect of the orally active local anaesthetic mexiletine on the cough response to two different tussive agents, a C-fibre ending stimulator capsaicin and a chemostimulant tartaric acid, was examined in normal subjects.
METHODS The cough threshold, defined as the lowest concentration of capsaicin (C5-CP) or tartaric acid (C5-TA) causing five or more coughs, and histamine induced bronchoconstriction were measured three hours after a single oral dose of 300 mg mexiletine or placebo in 14 normal subjects.
RESULTS Mexiletene in a mean (SE) serum concentration of 0.99 (0.04) μg/ml significantly increased C5-TA from a geometric mean (SE) of 32.0 (1.27) mg/ml with placebo to 49.9 (1.34) mg/ml, but C5-CP did not differ significantly between treatment with mexiletine (12.2 (1.33) μM) and placebo (14.9 (1.23) μM).
CONCLUSIONS These results suggest that the cough response to capsaicin and tartaric acid may be mediated in part via different neural pathways.
- cough response
- mexiletine
- capsaicin
- tartaric acid
Statistics from Altmetric.com
Cough elicited by inhaled tussive agents is mediated via neural pathways. Irritant receptors, and possibly C-fibre endings, are generally recognised as cough receptors in the airways.1Capsaicin is the active ingredient of red pepper and has been presumed to produce cough mainly by stimulating C-fibre endings,2though its action may be indirect.1 In contrast, although tartaric acid and citric acid are chemostimulants that have been postulated to induce cough by stimulating irritant receptors, it has been shown that the capsaicin receptor antagonist capsazepine inhibits cough induced by citric acid as well as capsaicin.3 Thus, it remains unclear whether capsaicin and chemostimulants elicit cough through different neural pathways.
Mexiletine is an orally active local anaesthetic agent. It has been shown that a single oral dose of mexiletine reduces histamine induced reflex bronchoconstriction by the same degree as intravenous lidocaine in subjects with mild asthma.4 Thus, oral mexiletine is useful in investigating the effects of local anaesthetics on various airway functions because aerosol administration of these drugs can in itself cause an initial bronchoconstriction5 and may influence the cough response to tussive agents.
We therefore investigated whether oral administration of mexiletine could reduce the cough response to inhaled capsaicin and tartaric acid in normal subjects. We also examined the inhibitory effect of mexiletine on histamine induced bronchoconstriction to confirm that the tested dose is adequate.
Methods
SUBJECTS
Fourteen normal young women with a mean (SE) age of 20.4 (0.2) years (range 20–22) were selected from 20 non-smoking university students who underwent histamine, capsaicin, and tartaric acid challenge tests during a three week run in period before entering the study. The 14 subjects selected had a histamine PC20 value (concentration of histamine producing a 20% fall in FEV1) of <40 mg/ml. Informed consent was obtained from all subjects and the study was approved by the ethics committee of the Kanazawa University Hospital.
MEASUREMENT OF COUGH SENSITIVITY
Cough sensitivity to capsaicin and tartaric acid were measured by the method described previously.6 Tartaric acid (Wako Pure Chemical Industries Ltd, Tokyo, Japan) was dissolved in physiological (normal) saline to give concentrations of 1.56, 3.12, 6.25, 12.5, 25, 50, 100, 200, 400, and 800 mg/ml. Capsaicin (30.5 mg) was dissolved in Tween 80 (1 ml) and ethanol (1 ml) and then in normal saline (8 ml) to make a stock solution of 3.05 mg/ml (1 × 10–2 M) which was stored at –20°C. This solution was diluted with physiological saline to give solutions of 0.49, 0.98, 1.95, 3.9, 7.8, 15.6, 31.2, 62.5, 125, 250, 500, and 1000 μM. Subjects inhaled progressively increasing concentrations of the tartaric acid or the capsaicin solution for 15 seconds by mouth tidal breathing every 60 seconds from a Bennett twin nebuliser (3012-60 ml, Puritan-Bennett Company, Carlsbad, California, USA), inhaling increasing concentrations until they coughed at least five times. The nebuliser output was 0.21 ml/min. It has been reported that the aerodynamic mass median diameter (MMD) of the particles is 3.60 μm with a geometric standard deviation of 3.47.7 The number of coughs induced by capsaicin or tartaric acid was counted by two medical technicians. The cough threshold was defined as the lowest concentration of capsaicin (C5-CP) or tartaric acid (C5-TA) that elicited five or more coughs.6
MEASUREMENT OF HISTAMINE INDUCED BRONCHOCONSTRICTION
Histamine dihydrochloride (Sigma Chemical Company, St Louis, Missouri, USA) was dissolved in physiological saline to make solutions of 0.04, 0.08, 0.16, 0.31, 0.63, 1.25, 2.5, 5, 10, 20, 40, 80 and 160 mg/ml. Histamine was inhaled for two minutes by tidal mouth breathing from a DeVilbiss No. 646 nebuliser (DeVilbiss Co, Somerset, Pennsylvania, USA) operated by compressed air at 5 l/min, immediately followed by measurement of forced expiratory volume in one second (FEV1) (Transfer Test, P K Morgan Ltd, Chatham, UK). Increasing concentrations of histamine were successively inhaled until a fall of 20% or more in the FEV1 occurred. PC20 values were determined by linear interpolation from the log dose response curve.
STUDY PROTOCOL
On six subsequent visits seven days apart, in random order and in a double blind fashion, the subjects took three capsules at 11.00 hours (either 300 mg mexiletine or placebo). The order of measurement of the cough threshold to capsaicin and tartaric acid and bronchial responsiveness to histamine was also randomised. Each subject attended at 13.30 hours on the six separate days. After resting for 30 minutes challenge with capsaicin, tartaric acid, or histamine was started.
Immediately after the histamine challenge serum was collected from each subject in order to examine the serum concentration of mexiletine which was measured by ELISA.
DATA ANALYSIS
Values for C5-CP, C5-TA and PC20 were presented as geometric means with geometric standard errors (GSE). Changes in C5-CP, C5-TA, and PC20 by treatment with mexiletine in each subject were shown in doubling concentrations, which were calculated as log2 (the value with mexiletine/the value with placebo) and presented as arithmetic means (SE). Geometric mean values for C5-CP, C5-TA, and PC20 were compared during the run in period and during treatment with mexiletine and with placebo by the Student's paired ttest. Simple regression analysis was employed in assessing the relationship between the parameters. Significance was based on a 95% confidence level (p<0.05).
Results
The values for C5-CP, C5-TA, and PC20 were not significantly different between the run in period and on the first and second visits. The geometric mean (SE) values for C5-CP were 13.5 (1.23) μM during the run in period and 14.9 (1.23) μM and 12.2 (1.33) μM with placebo and mexiletine, respectively (fig 1). The C5-TA value with mexiletine was 49.9 (1.34) mg/ml, which was significantly greater than that with placebo (32.0 (1.27) mg/ml) (doubling concentration 0.64 (0.25), p = 0.02) and that during the run in period (32.0 (1.20) mg/ml (doubling concentration 0.64 (0.29), p = 0.04; fig 1). There was a significant correlation between C5-CP and C5-TA values during the run in period (r = 0.737, p = 0.003) and during treatment with placebo (r = 0.707, p = 0.005). On the other hand, the correlation coefficient between C5-CP during the run in period and during placebo treatment was 0.880 (p<0.0001), and between C5-TA during the run in period and during placebo treatment was 0.849 (p = 0.0001).

Cough threshold to inhaled capsaicin (C5-CP) and tartaric acid (C5-TA) in each subject in the run in period (baseline) and three hours after an oral dose of mexiletine and placebo. Each horizontal bar represents a geometric mean value.
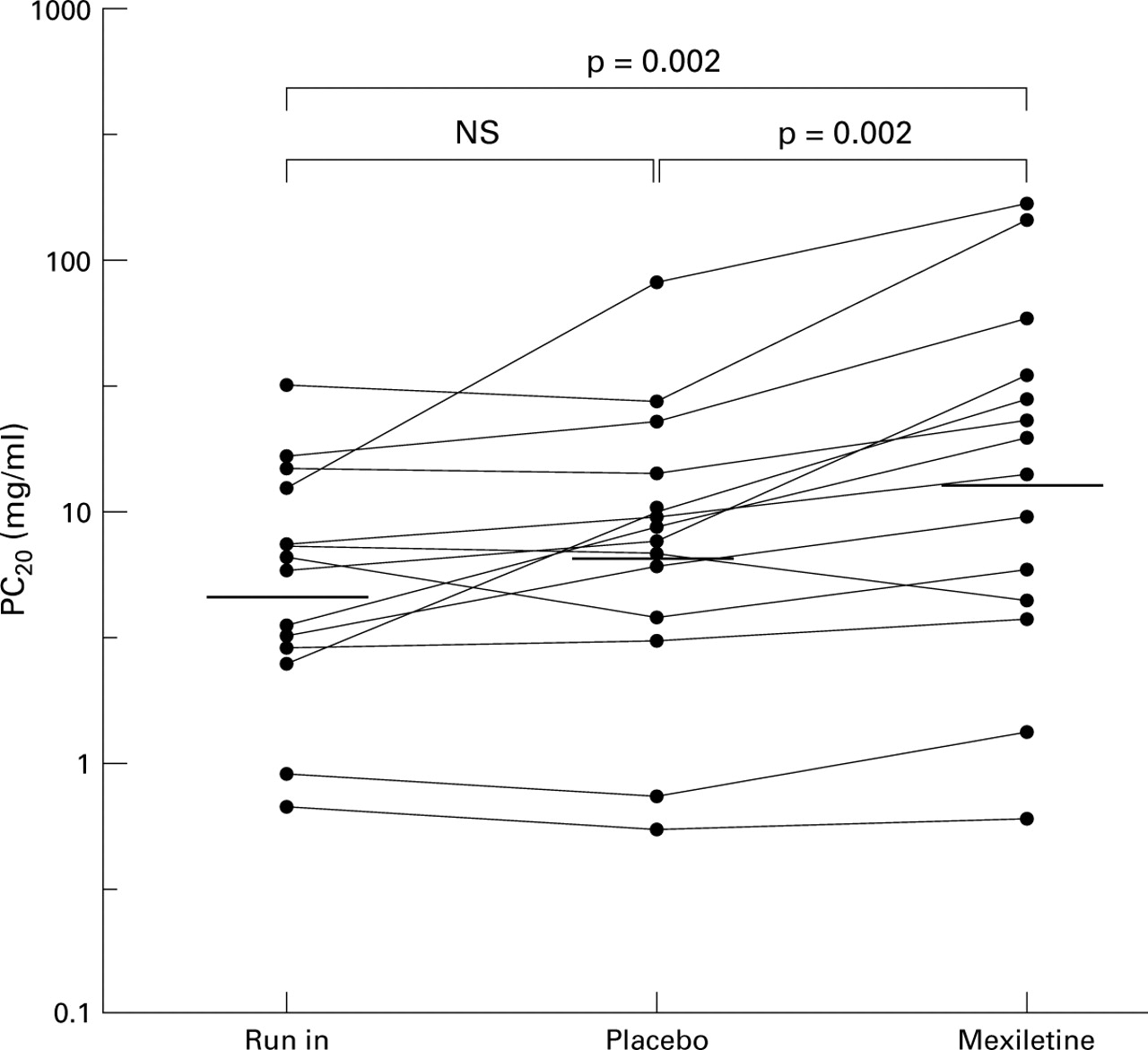
The geometric mean (SE) PC20 values were 5.08 (1.33) mg/ml during the run in period and 7.08 (1.42) mg/ml and 13.4 (1.55) mg/ml during treatment with placebo and mexiletine, respectively (fig 2). The value with mexiletine was significantly greater than that with placebo (doubling concentration 0.90 (0.23), p = 0.002) and that in the run in period (doubling concentration 1.38 (0.35), p = 0.002). The serum concentration of mexiletine immediately after completing the histamine challenge was 0.99 (0.04) μg/ml (therapeutic range 0.7–2.0 μg/ml).
{kind=link}
{kind=link}
Histamine PC20 value in each subject in the run in period (baseline) and three hours after an oral dose of mexiletine and placebo. Each horizontal bar represents a geometric mean value.
After administration of mexiletine five subjects complained of mild to severe dizziness which had disappeared completely by the next morning. Each patient also felt nauseous and sleepy.
Discussion
This study has shown that oral mexiletine reduces cough sensitivity to inhaled tartaric acid, but not to capsaicin, and decreases histamine induced bronchoconstriction in non-asthmatic subjects. The latter result is in agreement with Groeben and coworkers.4 The serum concentrations of mexiletine were in the therapeutic range for cardiac protection against dysrhythmias. It is suggested that tartaric acid induced cough may be mediated in part via the same neural pathway as histamine induced reflex bronchoconstriction in normal subjects, whereas the neural pathway may not be involved in capsaicin induced cough.
Local anaesthetics may influence airway responses such as bronchial responsiveness and cough sensitivity by several mechanisms, including direct airway smooth muscle relaxation, inhibition of mediator release from inflammatory and resident cells in the airways, central nervous system depression, and neural blockade of vagal reflex pathways. Although the direct effects of local anaesthetics on airway smooth muscle tone and mediator release from inflammatory cells have been shown in vitro, the drug concentration necessary to achieve these effects was more than 100 times greater than the concentration used clinically.8 ,9 It is possible that severe depression of the central nervous system suppresses the airway responses, but it has been reported that lidocaine prevents reflex induced cough in anaesthetised subjects.10 Accordingly, it is thought that the major mechanism by which mexiletine reduces tartaric acid induced cough and histamine responsiveness is by neural blockade of vagal reflex pathways.
Histamine causes both direct airway smooth muscle contraction and vagally mediated reflex constriction.11 Brownet al 12 have shown in a dog model that local anaesthetics are effective in blocking neurally mediated reflex induced airway constriction, whereas they are ineffective in preventing direct airway smooth muscle contraction induced by methacholine. In asthmatic subjects it has been clearly shown that oral mexiletine blocks reflex mediated histamine induced bronchoconstriction, as does intravenous lidocaine.4 We therefore examined the effect of oral mexiletine on histamine induced bronchoconstriction to confirm that the drug in the tested dose blocks reflex mediated bronchoconstriction in non-asthmatic subjects.
Local anaesthetics prevent sensory nerve traffic in both myelinated and non-myelinated nerves and are the most consistently effective antitussive agents,13 but the effects of anaesthetics on the cough response to tussive agents have been controversial. Cross and colleagues14 reported that bupivacaine administered by inhalation, but not by intravenous infusion, reduced the cough induced by citric acid aerosol in man, suggesting a different effect between local and systemic administration of anaesthetics. Choudryet al 15 have shown that inhalation of lidocaine, but not dyclonine, reduces the cough response to inhaled capsaicin at doses that do not affect reflex bronchoconstriction in humans, while both lidocaine and dyclonine cause significant reports of oral anaesthesia which suggests that the inhibitory effect of lidocaine may be mediated by the sensory pathways that are unaffected by dyclonine. In the present study oral administration of mexiletine inhibited both the cough response to inhaled tartaric acid and histamine induced bronchoconstriction, but did not alter capsaicin induced cough. In addition, the relationship between the cough threshold to capsaicin and tartaric acid was relatively weaker than that to each cough stimulant between the run in period and placebo treatment. These findings suggest that inhaled capsaicin and tartaric acid cause cough via somewhat different neural pathways and that the histamine induced reflex bronchoconstriction may be mediated in part by the same neural pathway as tartaric acid induced cough.