Article Text

Abstract
Objective To examine the impact of ACE inhibitor (ACE-I)/angiotensin receptor blocker (ARB) use on rate of SARS-CoV-2 infection and adverse outcomes.
Methods This nationwide case-control and cohort study included all individuals in Denmark tested for SARS-CoV-2 RNA with PCR from 27 February 2020 to 26 July 2020. We estimated confounder-adjusted ORs for a positive test among all SARS-CoV-2 tested, and inverse probability of treatment weighted 30-day risk and risk ratios (RRs) of hospitalisation, intensive care unit (ICU) admission and mortality comparing current ACE-I/ARB use with calcium channel blocker (CCB) use and with non-use.
Results The study included 13 501 SARS-CoV-2 PCR-positive and 1 088 695 PCR-negative individuals. Users of ACE-I/ARB had a marginally increased rate of a positive PCR when compared with CCB users (aOR 1.17, 95% CI 1.00 to 1.37), but not when compared with non-users (aOR 1.00 95% CI 0.92 to 1.09).
Among PCR-positive individuals, 1466 (11%) were ACE-I/ARB users. The weighted risk of hospitalisation was 36.5% in ACE-I/ARB users and 43.3% in CCB users (RR 0.84, 95% CI 0.70 to 1.02). The risk of ICU admission was 6.3% in ACE-I/ARB users and 5.4% in CCB users (RR 1.17, 95% CI 0.64 to 2.16), while the 30-day mortality was 12.3% in ACE-I/ARB users and 13.9% in CCB users (RR 0.89, 95% CI 0.61 to 1.30). The associations were similar when ACE-I/ARB users were compared with non-users.
Conclusions ACE-I/ARB use was associated neither with a consistently increased rate nor with adverse outcomes of SARS-CoV-2 infection. Our findings support the current recommendation of continuing use of ACE-Is/ARBs during the SARS-CoV-2 pandemic.
Trial registration number EUPAS34887
- clinical epidemiology
- critical care
- viral infection
- respiratory infection
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is the key question?
Does use of ACE inhibitors (ACE-I) and angiotensin receptor blockers (ARBs) increase the rate or worsen the outcome of SARS-CoV-2 infection?
What is the bottom line?
Use of ACE-I/ARB was associated neither with a consistently increased rate nor with adverse outcomes of SARS-CoV-2 infection, compared with ACE-I/ARB non-use or calcium channel blocker use.
Why read on?
This population-based study, including all individuals PCR tested for SARS-CoV-2 in Denmark, used extensive confounder adjustment and an active comparator design to examine the association between ACE-I/ARB use and the rate of microbiologically verified SARS-CoV-2 infection as well as the associated outcomes including hospitalisation, intensive care unit admission, mechanical ventilation and death.
Introduction
The use of renin–angiotensin system inhibitors, including ACE inhibitors (ACE-Is) and angiotensin receptor blockers (ARBs), has been suggested to increase the risk of being infected by SARS-CoV-2 and of adverse outcomes of coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2. ACE-Is/ARBs upregulates the human ACE2 receptor, which facilitates entry of SARS-CoV-2 into cells.1–5 The initially published studies of ACE-I/ARB users and SARS-CoV-2 infection reported no increased risk or worsened outcome after a positive SARS-CoV-2 test or a diagnosis of COVID-19.6–16 However, available studies are limited by incomplete data on recent ACE-I/ARB use and preexisting comorbidities,6 7 9 by restriction to hospitalised or hospital-diagnosed COVID-19 patients,9 10 12–15 or by incomplete follow-up.6 Other limitations have included immortal time bias from inclusion of in-hospital ACE-I/ARB use after COVID-19 diagnosis,10 11 15 16 which may lead to apparently beneficial effects, because ACE-I/ARBs would only be prescribed if patients are haemodynamically stable and have survived until drug initiation. Only few studies on risk of SARS-CoV-2 infection included an active comparator.12 13
Major professional societies have called for further high-quality research and issued warnings against ACE-I/ARB discontinuation in patients with SARS-CoV-2 infection,1 17 to avoid worsening of underlying cardiometabolic conditions.18
As ACE-Is/ARBs are widely used drugs, any association with rate of infection or adverse outcomes of SARS-CoV-2 infection may have an important public health impact. Thus, there is an urgent need to examine the hypotheses of increased rate of SARS-CoV-2 infection and worsened outcome, among users of ACE-Is/ARBs.
Methods
Design and setting
We conducted this nationwide combined case-control and cohort study in Denmark (population ~5.8 million persons) to study the rate (case-control design) and the prognosis (cohort design) of SARS-CoV-2. Denmark has a uniform tax-supported healthcare system responsible for all acute care in Denmark. The unique personal identification number assigned at birth or on immigration allows individual-level linkage of data and complete follow-up.19
As previously described,20 data on all individuals tested for SARS-CoV-2 RNA by reverse transcriptase PCR (RT-PCR) were obtained from the Danish Microbiology Database21 and linked to regularly updated data from the Danish National Patient Registry,22 the Civil Registration System,23 the National Prescription Database24 and the Danish Register of Causes of Deaths.25
Participants
The study included prospectively collected data on all individuals tested for SARS-CoV-2 RNA from 27 February 2020 (the date when the first patient tested positive for SARS-CoV-2 in Denmark) to 26 July 2020, allowing complete 30-day follow-up through 26 August 2020.
The study population for the analysis of the rate of acquiring a positive SARS-CoV-2 test (the case-control analysis) included all patients tested for SARS-CoV-2, while the analysis of the outcome (the cohort analysis) only included patients who tested positive for SARS-CoV-2. The first date of a positive test was defined as the index date.
Medication exposures
Current use of ACE-Is and ARBs was ascertained from prescriptions filled within 90 days before testing (online supplemental eFigure 1). Former use was defined as a prescription filled within 91–365 days before testing, while non-use was defined as no prescriptions filled during 1 year before testing. Prescription data included complete and valid information on all prescriptions filled at community pharmacies in Denmark since 1995.24 Registry data include date of dispensing, Anatomical Therapeutic Chemical code and drug quantity. In addition to prescriptions for ACE-I/ARBs, we obtained data on prescriptions for other antihypertensive medications, including calcium channel blockers (CCBs), beta blockers and thiazides.
Supplemental material
The main exposure comparisons were current use of ACE-Is/ARBs versus current use of CCBs, and current use of ACE-Is/ARBs versus no ACE-Is/ARB use. The first comparison allowed us to reduce confounding by indication, as CCB is an active drug with medical indications similar to those for ACE-Is/ARBs and with no known effects on the renin–angiotensin system.
SARS-CoV-2 infection and adverse outcomes
Cases in the case-control analysis were individuals acquiring a positive SARS-CoV-2 PCR test, and controls were individuals with a negative PCR test. The primary outcome in the cohort analysis of outcome was death within 30 days following a positive SARS-CoV-2 test. Secondary outcomes included hospital admission (hospital stay lasting >12 hours) within 30 days after index date, among patients who were not already hospitalised. Additional secondary outcomes included intensive care unit (ICU) admission, ICU admission with mechanical ventilation (MV) and dialysis within 30 days after index date. Secondary outcomes were obtained from the Danish National Patient Registry, which is also the platform for mandatory reporting to the national database for quality of ICU, and earlier assessments of the accuracy of its data on ICU admissions, ICU admission with MV and dialysis yielded positive predictive values of 96%–100%.26 27
Potential confounders
We included a wide range of potential confounders that may be associated with both ACE-I/ARB use and the risk and outcome of SARS-CoV-2 infection (table 1). Data on age, sex, marital status, ethnicity and urban residence were obtained from the Civil Registration System.23 We also obtained information on comorbidities associated with an inpatient stay or an outpatient hospital clinic diagnosis or with treatment by prescribed medications within 10 years before the index date (codes provided in online supplemental eTable 1).22 24 Prescriptions for concurrent medications filled within 90 days before the index date were also included.24
Characteristics of patients with positive and negative tests for SARS-CoV-2
Statistical methods
In the test-negative case-control analysis, the association between ACE-I/ARB use and a positive SARS-CoV-2 test was examined using a logistic regression model to compute ORs with 95% CIs adjusted for all covariates in table 1 and test date in 3-day intervals. In post hoc analyses, we tabulated patient characteristics in all tested patients by exposure group (current ACE-I/ARB use, no ACE-I/ARB use and current CCB use) and described positive:negative ratio, both overall and stratified by age group.
In the cohort analyses of outcome, we computed a propensity score (PS) for each individual, that is, the probability of being exposed in each comparison (eg, current ACE-I/ARB use vs current CCB use), using a logistic regression model including all covariates in table 1. We used the PS for inverse probability of treatment weighting (IPTW) with stabilised weights to estimate the average treatment effect in the population.28 Covariate balance before and after IPTW was described using standardised mean differences.
We restricted the comparison of current vs no ACE-I/ARB use to patients aged 50 years or older as there were only few ACE-I/ARB users, but many non-users, under age 50 leading to imbalance before restriction.
The cohort analysis of adverse outcomes followed patients from the day of their first positive test result to the date of the outcome of interest, that is, hospital admission, ICU admission (with or without need for MV), dialysis, date of death, emigration, or for up to 30 days. Patients were excluded in the analysis of each non-fatal outcome if they experienced that outcome from seven to 1 day before the test date.
Patient characteristics were tabulated according to each exposure group before and after weighting. For each exposure group, we estimated the 30-day weighted risks and risk differences with robust 95% CIs using generalised linear models with a binomial distribution and an identity link. Risk ratios (RRs) were estimated similarly but using a log link.
A subgroup analysis was conducted to address potential effect modification by age group (≤65 years, >65 years). A second subgroup analysis was conducted in patients with assumed uncomplicated hypertension as the primary indication for treatment (defined as patients without a history of diabetes, renal disease, angina pectoris, myocardial infarction or heart failure). A third subgroup analysis was restricted to patients tested after the test strategy changed in Denmark and the country was locked down on 13 March 2020.
In a sensitivity analysis, we explored the robustness of our findings by repeating the analyses for patients who filled a prescription within 120 days before a positive test. We also conducted a sensitivity analysis stratified by calendar time to address changes in testing and hospitalisation strategy. We followed the protocol registered in the European Union electronic Register of Post-Authorisation Studies (EU PAS Register) (record number: EUPAS34887), with two exemptions. First, standardised mortality rate weighting was replaced with IPTW with stabilised weights to better handle the low number of current CCB users in the comparison group. Second, the comparison with non-users of ace-i/ARB was restricted to patients aged 50 years and older due to the imbalance mentioned above.
All data management and statistical analyses were performed using STATA V.16 MP.
Results
The study included 13 501 test-positive and 1 088 695 test-negative individuals (table 1). Among test-positive cases, there were 1466 current ACE-I/ARB users (11%) (587 ACE-I users, 887 ARB users and 8 using both) of whom 1336 were 50 years or above and included in the comparison between current ACE-I/ARB use with no ACE-I/ARB use. Among the 1466 current ACE-I/ARB users, 1065 did not receive concurrent CCBs and could therefore be included in the comparison between current ACE-I/ARB use and current CCB use.
Rate of acquiring a positive SARS-CoV-2 test
There were no major differences in characteristics of test-positive and test-negative individuals with regard to age, sex, comorbidity and medication use (table 1). There were, however, more healthcare professionals, more living in urban areas, but fewer non-immigrants among the test-positive cases. After adjusting, ACE-I/ARB users had a slightly increased rate of a positive test compared with current CCB users (adjusted OR 1.17, 95% CI 1.00 to 1.37) (figure 1). ACE-I/ARB users had a similar rate of a positive test compared with ACE-I/ARB non-users (adjusted OR 1.00, 95% CI 0.92 to 1.09) (figure 1).

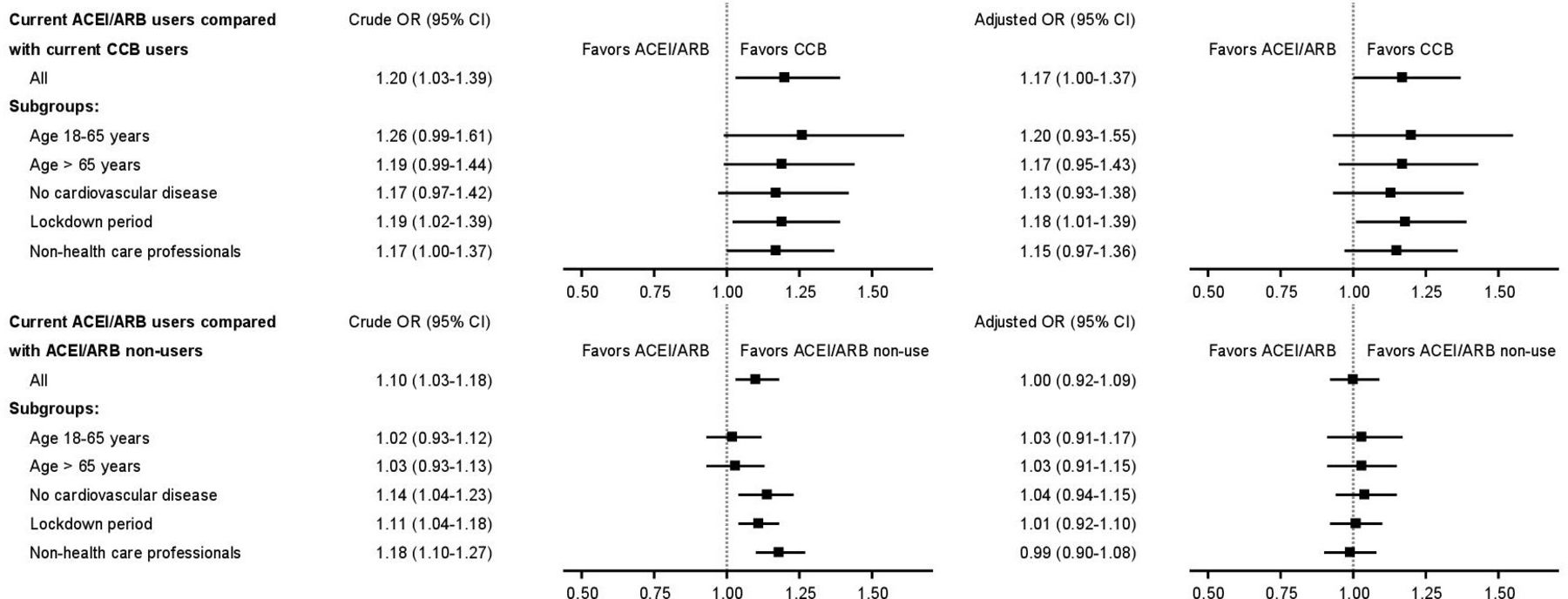{kind=link}
OR for a positive test among ACE-I/ARB users compared with CCB users and non-users tested for SARS-CoV2. ACE-I, ACE inhibitors; ARB, angiotensin receptor blocker; CCB, calcium channel blocker.
Outcomes of SARS-CoV-2 infection
Patient characteristics of current ACE-I/ARB users are compared with CCB users in table 2 and with non-users in table 3.
Characteristics of current ACE-I/ARB users and current CCB users before and after inverse probability of treatment weighting
Characteristics of current ACE-I/ARB users and non-users aged 50 years or above, before and after inverse probability of treatment weighting
After excluding patients both on ACE-I/ARB and CCB from the SARS-CoV-2 positive cohort, 1065 ACE-I/ARB users and 289 current CCB users remained. The characteristics of patients in the two groups were well balanced after weighting (table 2).
The risk of hospital admission was 36.5% in ACE-I/ARB users and 43.3% in CCB users (RR 0.84, 95% CI 0.70 to 1.02) after weighting (table 4). The risk of ICU admission was 6.3% in ACE-I/ARB users and 5.4% in CCB users (RR 1.17, 95% CI 0.64 to 2.16), while the risk of death within 30 days was 12.3% in ACE-I/ARB users and 13.9% in CCB users (RR 0.89, 95% CI 0.61 to 1.30).
Outcomes in current ACE-I/ARB users compared with ACE-I/ARB non-users aged 50+ years and compared with CCB users
Among SARS-CoV-2 positive patients aged 50 years or above, 1336 were current ace-i/ARB users and 4326 were non-users. Characteristics of patients in the two groups were well balanced after weighting (table 3). The weighted risk of hospital admission was 32.3% in ACE-I/ARB users and 33.1% in non-users (RR 0.98, 95% CI 0.84 to 1.14) (table 4). The risk of ICU admission was 6.4% in ACE-I/ARB users and 5.1% in non-users (RR 1.25, 95% CI 0.66 to 2.36), while the risk of death within 30 days was 9.5% in ACE-I/ARB users and 10.8% in non-users (RR 0.88, 95% CI 0.68 to 1.14).
Subgroup analyses
Results were confirmed in subgroup analyses stratified by age, no cardiovascular disease other than hypertension, and period of testing (online supplemental eTable 2).
Results for various exposure definitions are shown in online supplemental eTable 3. Results remained robust when the exposure window was changed to 120 days and when current ACE-I/ARB use was compared with current thiazide and beta-blocker use. There was no conclusive difference in the associations when analysing current ACE-I and ARB use separately, although point estimates differed.
Post hoc analyses
Among all tested individuals, patient characteristics were similar for current ACE-I/ARB users compared with current CCB users, while ACE-I/ARB non-users were younger and had less comorbidity (online supplemental eTable 4). The overall positive:negative ratios were similar for current ACE-I/ARB users, ACE-I/ARB non-users and current CCB users (online supplemental eTable 5). When stratified by age, the positive:negative ratio differed slightly between the exposure groups among young adults only.
Discussion
In this large nationwide study of prospectively collected data, current ACE-I/ARB use was associated with a marginally increased rate of testing positive compared with CCB use but not when compared with ACE-I/ARB non-use. Moreover, we showed that among individuals who tested positive for SARS-CoV-2, current use of ACE-Is/ARBs was not associated with increased risk of hospitalisation, ICU admission or 30-day mortality.
Strengths and limitations of the study
Strengths of the current study include its nationwide population-based design, including all individuals tested for SARS-CoV-2 in Denmark, with linkage to validated medical registries and complete follow-up for censoring of all Danish residents.19 20 23–25 ICU admissions and treatments also are recorded accurately, as the Danish National Patient Registry is used for financial reimbursements to hospitals and for mandatory reporting to national quality of care databases.26 27 The RT-PCR test for presence of SARS-CoV-2 has high sensitivity and predictive value,29 and registration of the tests are complete and accurately recorded in the Danish Microbiology Database.21 Despite these strengths, the study had several limitations. The threshold for SARS-CoV-2 testing was lowered as the pandemic progressed and testing capacity has increased steadily since March 2020.20 Importantly, our results did not change after restriction to patients tested after the policy guidelines changed and the country was locked down on 13 March 2020. Any bias should be minimal as use of ACE-I/ARB was not expected to influence the threshold for testing, which followed national guidelines. This was confirmed by the lack of major difference in positive:negative ratios between exposure groups.
Medication use was assessed using complete and valid data on prescriptions prior to testing in a time window corresponding to the typical interval between medication refills. Still, misclassification could have occurred if some patients had sporadic use of drugs filled more than 90 days before testing. Given the chronic use of the drugs included in the study, such misclassification should be minor and not associated with the outcome of interest. The direction of any information bias is therefore expected to be towards the null. It is likely to be minimal as no change in estimates was observed after the time window was extended from 90–120 days before testing in a sensitivity analysis. A related concern is that we lacked in-hospital medication data to examine the impact of continued and discontinued use of prescribed drugs during follow-up, which may be relevant, since 50% of hospitalised COVID-19 patients may discontinue ACE-I/ARB.30
The use of ICU admission as an outcome in observational prognostic studies is challenging.31 In clinical practice, ICU admission is offered to patients who are expected to have a clear prognostic benefit from invasive monitoring and treatment.32 This is the case particularly in countries with limited ICU capacity, which are not able to accommodate the level of need during the COVID-19 pandemic. In Denmark, ICU capacity was more than sufficient during the study period. In addition, patients’ quality of life, functional level at home and hospital capacity may influence the decision to admit a patient to the ICU. This may explain why ICU and mortality outcomes tended to go in opposite directions for some associations examined in our study.
Potential confounding by medical indication for drug treatment was handled by use of an active comparator in the main analysis, by implementing IPTW that included a large number of potential confounders, and by restricting analyses to subgroups according to indication for treatment. Although cardiovascular and other diagnoses used in the study have documented high positive predictive values,20 33 we cannot entirely rule out that our findings were influenced by unmeasured confounding by indication and contraindication for treatments and by severity of underlying comorbidity. A final concern is that precision of risk estimates was limited in some subgroups.
Comparison with other studies
Our results on risk of acquiring a positive SARS-CoV-2 test are consistent with the few published studies on risk of ACE-I/ARB users compared with non-users,6–8 12 13 16 and to other antihypertensives.12 13 The earlier studies, which used hospital based rather than population based data or were limited by incomplete data on recent ACE-I/ARB exposure, reported ORs ranging from 0.94 to 1.23 associated with ACE-I/ARB use.6–8 12 13 16 A Danish study limited to hospital-diagnosed COVID-19 cases and population controls found similar association between ACE-I/ARB use and non-use (HR 1.05, 95% CI 0.80 to 1.36) and CCB use (HR 1.23, 95% CI 0.89 to 1.70), respectively.13
Thus, our study has confirmed and extended the previous findings in a large nationwide cohort of all individuals with microbiologically confirmed SARS-CoV-2 infection comparing ACE-I/ARB users to a specific active comparator group of users of another antihypertensive, CCB, corroborating no major association.
In our cohort analysis of patients with positive SARS-CoV-2 test, we found that ACE-I/ARB users had no increased risk of an ICU admission, confirming previous hospital-based studies.9–11 13–15 More importantly, our findings qualified that ACE-I/ARB use was not associated with increased risk of hospitalisation when accounting for confounding factors. Our adverse outcome findings remained robust across varying exposure definitions, subgroups and also in comparison with CCB use.
Our observed associations were more precise and closer to the null than reported in a recent systematic review.34 The few larger studies had some limitations. Reynolds et al conducted a study of 12 594 patients tested for SARS-CoV-2 in emergency departments or during hospitalisation at New York University Langone Health.6 They examined use of ACE-Is/ARBs and other antihypertensive medications and a positive SARS-CoV-2 test result, as well as severity of COVID-19, and found no substantial association. The study was limited by its inclusion of only 18 months of chronic disease history, as well as by defining ACE-I/ARB exposure as any treatment yes/no within 18 months before the SARS-CoV-2 tests without evidence of discontinuation in the previous 30 days. In addition, severity of illness (defined by ICU admission, MV or death) was assessed only at one time point at the end of the study period, that is, length of follow-up differed by date of inclusion.6 An Italian case-control study included 6272 patients diagnosed with COVID-19 matched to 30 759 controls. The authors found that neither ACE-I nor ARB use was associated with risk of and severity of COVID-19.7 Exposure was defined as redemption of any prescription in 2019. A Danish study of 4480 patients with hospital-diagnosed COVID-19, found no clear association between ACE-I/ARB use and 30-day mortality (HR 0.83, 95% CI 0.67 to 1.03).13
Potential mechanisms
We have no data to examine whether conflicting mechanisms produced the neutral association with SARS-CoV-2 infection and outcomes that we observed. Cell-surface ACE2 expression, which is likely increased in patients treated with ACE-Is/ARBs, may facilitate SARS-CoV-2 entry into cells.5 However, ACE2 expression also has been shown to protect against development of severe acute lung injury in other infectious diseases.1 4 35 The null findings of our case-control risk analyses argue against any clinically relevant effect of ACE-I/ARB-mediated ACE2 upregulation in increasing SARS-CoV-2 risk in general. These issues will be addressed in several planned trials on the impact of losartan on organ dysfunction and mortality in patients hospitalised with SARS-CoV-2 infection (ClinicalTrials.gov Identifier: NCT04312009 and NCT04328012).
Conclusion
Our study showed that ACE-I/ARB use was not associated with a consistently higher rate of acquiring a positive SARS-CoV-2 test among tested individuals. Further, ACE-I/ARB use was not associated with increased mortality and other adverse outcomes among patients with microbiologically confirmed SARS-CoV-2 infection. These results support the recommendations of continuing treatment with ACE-Is/ARBs during the COVID-19 pandemic.
Acknowledgments
The Danish Departments of Clinical Microbiology are acknowledged for contributing to the national infectious disease surveillance. The Danish Health Data Authority and Statens Serum Institut are acknowledged for valuable support with preparation and linkage of data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ChristianFynbo, @dr_rwt
Correction notice This article has been corrected since it was published Online First. An author first name and last name were interchanged.
Contributors CFC, UH-J, AP, RWT and HTS planned and designed the study. All authors contributed with input to the design and participated in the interpretation of the data. CFC reviewed the literature, organised the writing and wrote the initial manuscript. All authors critically reviewed the manuscript and approved the final version for submission. AP and LCL conducted the statistical analyses. AP and HTS obtained funding. NCB, HTS, RWT supervised the study. AP and HTS are the guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The study was funded by Aarhus University and the University of Southern Denmark.
Competing interests CFC, UH-J, RWT and HTS have not received any personal fees, grants, travel grants or teaching grants from companies, but the Department of Clinical Epidemiology is involved in studies with funding from various companies as research grants to (and administered by) Aarhus University. MR, LCL, AP and JH have participated in industry-funded projects with money paid to their employer, the University of Southern Denmark. MM has received speaker or advisory board fees from AstraZeneca, Bayer, Boston Scientific, Boehringer-Ingelheim, Bristol-Myers Squibb, and Novo Nordisk.
Patient consent for publication Not required.
Ethics approval The study was registered at the University of Southern Denmark (record no. 10.960) and approved by the Danish Health Data Authority (FSEID-00004874). According to Danish law, registry-based studies do not require approval from ethics committees or informed consent from participants.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. No additional data available. Because of the sensitive nature of the data collected for this study, requests to access the databases used in this study from researchers at certified Danish research institutions may be sent to the Danish Health Data Authority by email to forskerservice@sundhedsdata.dk.