Article Text

Abstract
Rationale Genome-wide association studies (GWASs) have identified numerous loci associated with lower pulmonary function. Pulmonary function is strongly related to smoking and has also been associated with asthma and dust endotoxin. At the individual SNP level, genome-wide analyses of pulmonary function have not identified appreciable evidence for gene by environment interactions. Genetic Risk Scores (GRSs) may enhance power to identify gene–environment interactions, but studies are few.
Methods We analysed 2844 individuals of European ancestry with 1000 Genomes imputed GWAS data from a case–control study of adult asthma nested within a US agricultural cohort. Pulmonary function traits were FEV1, FVC and FEV1/FVC. Using data from a recent large meta-analysis of GWAS, we constructed a weighted GRS for each trait by combining the top (p value<5×10−9) genetic variants, after clumping based on distance (±250 kb) and linkage disequilibrium (r2=0.5). We used linear regression, adjusting for relevant covariates, to estimate associations of each trait with its GRS and to assess interactions.
Results Each trait was highly significantly associated with its GRS (all three p values<8.9×10−8). The inverse association of the GRS with FEV1/FVC was stronger for current smokers (pinteraction=0.017) or former smokers (pinteraction=0.064) when compared with never smokers and among asthmatics compared with non-asthmatics (pinteraction=0.053). No significant interactions were observed between any GRS and house dust endotoxin.
Conclusions Evaluation of interactions using GRSs supports a greater impact of increased genetic susceptibility on reduced pulmonary function in the presence of smoking or asthma.
- asthma
- respiratory measurement
- tobacco and the lung
Data availability statement
Data are available upon reasonable request pending all required approvals.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
Whether the reduction in pulmonary function associated with increasing genetic susceptibility is enhanced or reduced by having exposures to smoking or house dust endotoxin or by having asthma.
What is the bottom line?
Smoking or asthma amplifies the reduction in FEV1/FVC that occurs with greater genetic susceptibility.
Why read on?
Using the largest genome-wide association study meta-analysis of pulmonary function to date, we developed a robust Genetic Risk Score (GRS) for each pulmonary function trait in our data. We observed a significant interaction between the GRS for reduced FEV1/FVC and smoking status. Our study is the first to examine interactions between GRSs for reduced pulmonary function and asthma status or house dust endotoxin exposure. We observed a marginally significant interaction between the GRS for reduced FEV1/FVC and asthma. The finding that the association of genetic susceptibility with reduced pulmonary function is strongest among current smokers and asthmatics provides evidence that the population with higher genetic risk for impaired pulmonary function is more susceptible to the deleterious effects of smoking and asthma.
Introduction
Spirometric measures of pulmonary function, such as FEV1, FVC and their ratio, FEV1/FVC, are robust indices of respiratory health used in diagnosing and monitoring various lung conditions, including COPD. These pulmonary function metrics are predictors of mortality, even after adjusting for known risk factors.1–4
Pulmonary function is influenced by both genetic and environmental factors. Genome-wide association studies (GWASs) have identified many loci associated with pulmonary function.5–9 Environmental exposures, most notably, cigarette smoking, also substantially influence pulmonary function.10 11 Endotoxin, a lipopolysaccharide on the cell wall of Gram-negative bacteria ubiquitous in the environment, is a powerful initiator of innate immune response.12 Occupational endotoxin exposure is associated with lower lung function.13 14 Although endotoxin exposure in childhood might protect against asthma development,15 in adulthood, endotoxin in house dust has been associated with lower pulmonary function in asthmatics.16 17 Asthma is associated with reduced lung function in many studies.18
Considerable efforts to identify interactions between individual genetic variants and environmental exposures for many human traits and diseases have identified few to no significant interactions.19–21 Even with large sample sizes, power is limited to detect interactions with individual single-nucleotide polymorphisms (SNPs) in genome-wide analyses.19 Several authors have highlighted the advantage of using Genetic Risk Scores (GRSs) over individual SNPs for identifying significant interactions.22–24 For example, a genome-wide meta-analysis of FEV1 and FEV1/FVC by Hancock et al of nearly 50 000 individuals incorporated interaction with smoking but identified no genome-wide significant interactions despite the well-established association of smoking with these phenotypes.20 Using the summary results from Hancock et al 20 for 26 SNPs previously identified in main effects GWAS of pulmonary function,7 Aschard et al performed single SNP-by-smoking interaction tests and found no significant interactions.24 However, combining the effects of these individual SNPs into a GRS identified a significant interaction between smoking status and the GRS on FEV1/FVC.24 In a study of cotton textile workers, Zhang et al found a significant interaction between occupational endotoxin exposure and a 10-SNP GRS for lower FEV1 for longitudinal decline in FEV1.25 We are not aware of studies examining whether associations of GRSs with pulmonary function differ by asthma status.
Recently, a large-scale meta-analysis involving around 400 000 participants of European ancestry from the UK Biobank and SpiroMeta consortium brought the number of loci for pulmonary function to nearly 300.8 This largest meta-analysis of these outcomes to date, provides the ability to generate authoritative risk scores for pulmonary function in individuals of European ancestry. Shrine et al constructed a single GRS from variants identified for any of four pulmonary function traits (FEV1, FVC, FEV1/FVC and peak expiratory flow) weighted by the effect sizes for FEV1/FVC but found no interaction of GRS with ever-never smoking in relation to FEV1/FVC.8
We constructed GRSs for reduced pulmonary function based on results from the aforementioned meta-analysis8 to investigate whether associated genetic risk for reduced pulmonary function is more pronounced in the presence of smoking or other exposures related to reduced pulmonary function. We constructed a separate GRS for each of the three spirometric traits (FEV1, FVC and FEV1/FVC) based on the meta-analysis8 and applied these three GRSs in a case–control study of asthma in adults nested within a US farming cohort with data on smoking and house dust endotoxin. We examined an interaction hypothesis, namely, whether the reduction in pulmonary function associated with increasing GRS is enhanced or reduced by exposure to smoking or house dust endotoxin or by having asthma.
Methods
Study population and pulmonary function
The Agricultural Lung Health Study (ALHS) is a case–control study of current asthma in farmers and spouses of farmers, nested within the Agricultural Health Study.26 We enrolled 3301 participants in the ALHS from 2009 to 2013. Details regarding the ALHS study design, including measurement of pulmonary function, have been previously reported.16 27 28 Briefly, pulmonary function (FEV1 (in litres), FVC (in litres) and FEV1/FVC (proportion)) was measured during home visits by trained field technicians in accordance with American Thoracic Society guidelines.16 29 Tests were graded by Dr John Hankinson; participants with quality grades of D or F were excluded from analysis.16 30
Classification of asthma
As previously described,16 27 asthma cases were identified from the larger Agricultural Health Study cohort in three categories: self-reported doctor-diagnosed current asthma, potential undiagnosed asthma based on the presence of current asthma symptoms and asthma medication use in non-smokers, and overlapping diagnoses of current asthma and either COPD or emphysema in non-smokers. A random sample of cohort members who did not meet any of these case definitions was selected for enrolment as non-cases.
Endotoxin measurements
House dust samples were collected by vacuuming bedroom floors and sleeping surfaces of participants.16 Endotoxin levels in house dust were measured using the Limulus amebocyte lysate assay (Lonza Walkersville, Walkersville, Maryland, USA), as previously described.31–33 Measurements below the limit of detection were assigned a value equal to that limit divided by the square root of two.
Assessment of smoking
Smoking history was obtained from questionnaires. Participants were classified as current, former or never smokers. Pack-years were calculated as packs smoked per day times years smoked.
Genotyping
Details about the genotyping, imputation and quality control are in the online supplemental material.
Supplemental material
Genetic Risk Scores
Weighted GRSs were constructed using the complete summary results from the previous meta-analysis of more than 400 000 individuals of European ancestry.8 The summary results were pruned for linkage disequilibrium (LD) using the p value informed clumping method in PLINK V.1.9,34 based on the LD structure in the ALHS using a distance of ±250 kb and LD threshold of 0.5. We used a p value threshold of 5×10―9 to maximise stringency and for consistency with currently recommended genome-wide significance thresholds for resequencing analyses of individuals of European ancestry.8 35 After LD clumping, the numbers of SNPs remaining for GRS calculation were 1123 for FEV1, 835 for FVC and 1691 for FEV1/FVC. Weighted GRSs for ALHS participants were calculated as the weighted sum of the number of the risk alleles using effect estimates from the UK Biobank-SpiroMeta meta-analysis as weights.8 Further details about the calculation of GRSs can be found in the online supplemental material.
Statistical analyses
Using linear regression, we tested associations between each trait (FEV1 (litres), FVC (litres) and FEV1/FVC (proportion)) and its corresponding GRS adjusting for age, age2, height, height2, asthma (case and non-case), smoking status (current, former or never), pack-years of smoking, state of residence (Iowa and North Carolina), gender, first 10 genetic principal components and weight (kg, FVC only). Model examining associations of traits with smoking (two dummy variables for former or current smoking vs never) included the aforementioned covariates without pack-years or principal components. Models for association of traits with asthma were additionally adjusted for smoking and pack-years. Endotoxin was log10-transformed and models for association with traits were further adjusted for season of collection of dust sample. Interactions between the GRS and each exposure (smoking, asthma or endotoxin) were tested by adding product terms to the aforementioned models and adjusting for the first 10 genetic principal components. Where we identified significant two-way interactions, we considered further three-way interaction terms with the remaining two exposures. We considered a nominal p value cut-off of 0.05 for statistical significance of our results. All analyses were performed in R.36 Analyses used data release AHSREL201304.00.
Results
Study participants
Among the 3301 ALHS participants, 3069 had spirometry passing quality control and complete data on smoking, asthma and covariates, including 2844 of European ancestry based on principal components analysis. Among these 2844 participants, 1041 were asthma cases. Current smoking was reported by 4.3% and former smoking by 29.5% (table 1). About 52% were farmers; the rest were spouses of farmers. House dust endotoxin measurements were available for 2385 participants. Among these, 177 visits were to homes where a spouse had already been enrolled; spouses were removed, leaving 2208 participants for analyses of endotoxin.
Characteristics of the 2844 participants
Association between exposures and pulmonary function
As expected, smoking status was highly significantly associated with lower FEV1 and FEV1/FVC, with larger effect estimates for current smoking than for former smoking relative to never smoking (table 2). For FVC, inverse associations were observed for both current and former smoking, though the association for former smoking did not reach statistical significance (table 2). Pack-years of smoking was inversely associated with all three pulmonary function traits: FEV1: β=―0.009 L/pack-year, p value<2.0×10−16; FEV1/FVC: β=―0.002 L/pack-year, p value<2.0×10−16; and FVC: β=―0.005 L/pack-year, p value=4.4×10−12.
Association between the exposures and pulmonary function traits
Asthma was highly statistically significantly associated with lower pulmonary function for all three traits (table 2). Log10-transformed house dust endotoxin was inversely related to all three traits but not statistically significantly (table 2).
Genetic Risk Scores
Summary statistics of the GRSs for the three pulmonary function traits are shown in table 3; distributions of the GRSs are shown in online supplemental figure E1. As expected, the GRSs were highly significantly associated with lower values for each pulmonary function trait (table 3, all p values<8.9×10−8).
Association between GRSs and pulmonary function traits
Interaction between GRSs and smoking status
We observed significant interactions between the GRS for FEV1/FVC and smoking status. The interaction effect between GRS and smoking status shows the difference in the effects of GRS on FEV1/FVC between smokers (current or former) and never smokers. The inverse association between GRS and FEV1/FVC was greater for current smokers than never smokers (table 4); the estimated effect of GRS, per unit increase, on FEV1/FVC in never smokers was −0.003 and that for the current smokers was −0.012 with a difference of −0.009 (pinteraction=0.017). Even for former smokers, the inverse association between GRS and FEV1/FVC was higher compared with never smokers, where the estimated effect of GRS on FEV1/FVC in former smokers was −0.006 vs −0.003 in never smokers, with a difference of −0.003 (pnteraction=0.064). Figure 1 plots the association between the GRS and FEV1/FVC according to smoking status and shows that the harmful effects of smoking were larger among participants with higher GRSs. No significant interactions with the GRS were seen with smoking for FEV1 or FVC (lowest pinteraction=0.357, online supplemental table E1). We also tested for interactions between the GRS and pack-years of smoking in relation to each of the three traits but none were close to statistically significant (FEV1: βinteraction=0.0003, pinteraction=0.406; FVC: βinteraction=0.0005, pinteraction=0.480; FEV1/FVC: βinteraction=−0.00002, pinteraction=0.674). However, among current smokers, we observed a significant interaction between the GRS and the number of cigarettes smoked per day for FEV1/FVC (βinteraction=−0.0004, pinteraction=0.027).
Interaction between smoking and GRS in relation to FEV1/FVC

Association between GRS and FEV1/FVC differs by smoking status. FEV1/FVC is regressed on smoking status, GRS and their interaction, adjusting for age, age2, height, height2, state, gender, asthma status and 10 principal components. Shown are the estimated FEV1/FVC values from the model against the range of GRS in our data for the three smoking categories (never, former and current), calculated at the mean values of all continuous variables (GRS, age, age2, height, height2 and 10 principal components) and at the reference category for all categorical covariates (ie, non-asthmatic, female and residing at Iowa). The shaded areas denote 95% pointwise confidence bands. GRS, Genetic Risk Score.
Given that there is some genetic contribution to smoking behaviour and we identified an interaction between the GRS and smoking status in relation to FEV1/FVC, we tested whether its GRS was related to smoking and found no appreciable association (adjusting for age, age2, height, height2, asthma status, state, gender and genetic principal components): former smokers β=0.162, SE=0.096, p value=0.090; current smokers β=−0.139, SE=0.210, p value=0.508.
Interaction between GRSs and asthma
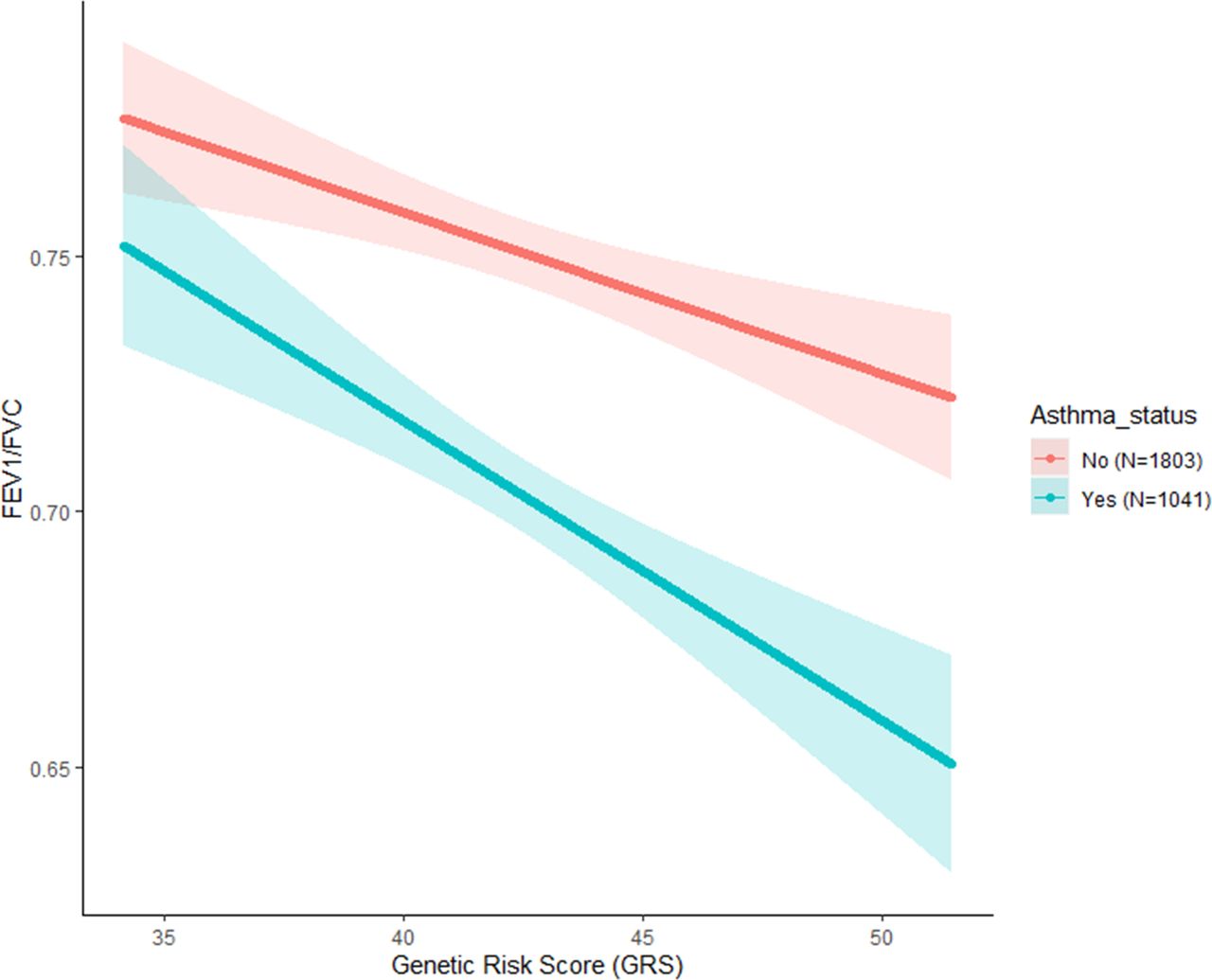
We observed a marginally significant interaction between the GRS and asthma in relation to FEV1/FVC with a stronger inverse association between the GRS and FEV1/FVC in asthmatics (estimated effect of a unit increase in GRS on FEV1/FVC=−0.006) than non-asthmatics (−0.003) with a pinteraction=0.053 (table 5). From figure 2, asthma had a stronger negative effect on FEV1/FVC among participants with higher GRSs. No appreciable interaction with asthma was seen for FEV1 or FVC (online supplemental table E2).
Interaction between asthma and GRS in relation to FEV1/FVC

{kind=link}
{kind=link}
Association between GRS and FEV1/FVC differs by asthma status. FEV1/FVC is regressed on asthma status, GRS and their interaction, adjusting for age, age2, height, height2, state, gender, smoking status, pack-years, and 10 principal components. Shown are the estimated FEV1/FVC values from the model against the range of GRS in our data for the two asthma categories, calculated at the mean values of all continuous variables (GRS, age, age2, height, height2, pack-years and 10 principal components) and 0 value for all categorical covariates (ie, never smoker, female and residing at Iowa). The shaded areas denote 95% pointwise confidence bands. GRS, Genetic Risk Score.
Given the interaction between asthma and the GRS in relation to FEV1/FVC, we evaluated the association between asthma and the GRS for this trait, adjusting for age, age2, height, height2, smoking status, pack-years, state, gender and genetic principal components. The GRS for FEV1/FVC was not significantly related to asthma (β=0.136, SE=0.087, p value=0.116).
Three-way interaction between smoking, asthma and GRSs
For FEV1/FVC, we examined whether the interaction effect between GRS and smoking status differed by asthma. In asthmatics, FEV1/FVC had steeper inverse relationship with increased genetic risk in current smokers (when compared with never smokers) than in non-asthmatics, yielding a statistically significant three-way interaction (online supplemental table E3 and online supplemental figure E2). The interaction effect between GRS and former smoking (in comparison to never smokers) for FEV1/FVC was not significantly different between asthmatics and non-asthmatics (online supplemental table E3).
Three-way interaction between smoking, gender and GRSs
Additionally, we examined whether the interaction effect between GRS for FEV1/FVC and smoking status differed by gender. In women, FEV1/FVC had a steeper inverse relationship with increasing genetic risk in current smokers compared with never smokers, whereas no such difference between current and never smokers was observed in men, yielding a significant three-way interaction effect between GRS, gender and current smoking (vs never smoking) (online supplemental table E4 and figure E3). The interaction effect between GRS and former smoking (in comparison to never smokers) was not significantly different by gender (online supplemental table E4).
Interaction between GRSs and endotoxin
We observed no significant interactions between the GRS and endotoxin for any of the traits (table 6 and online supplemental table E5). Because we had previously reported a stronger association between endotoxin and FEV1/FVC in asthmatics than non-asthmatics,16 we evaluated a possible three-way interaction with asthma but found no evidence for one (pthree-way interaction=0.667, online supplemental table E6).
Interaction between log10endotoxin and GRS in relation to FEV1/FVC
Discussion
As expected, all three pulmonary function traits (FEV1, FVC and FEV1/FVC) were significantly lower among both current and former smokers compared with never smokers, and asthmatics had lower pulmonary function than non-asthmatics. We developed a separate GRS for each of the three pulmonary function traits in our study population using a large-scale meta-analysis of European ancestry populations.8 These GRSs were highly statistically significantly associated with lower values for their corresponding pulmonary function traits. We observed a significant interaction effect where the reduction in FEV1/FVC with increasing GRS was more pronounced among current smokers and former than never smokers. We also found some evidence of interaction where the reduction in FEV1/FVC with increasing GRS was more pronounced among asthmatics than among non-asthmatics.
Although statistical power is reduced for higher level interactions, we evaluated possible three-way interactions in situations where we identified significant two-way interactions. We found some evidence that the interaction between GRS and current smoking on reduced FEV1/FVC was stronger among asthmatics than non-asthmatics and among women than men. However, because of small numbers within these three-way cross-classified strata, interpretation of any significant three-way interactions requires caution.
For FEV1/FVC, we observed significant interaction between its GRS and smoking status; for FEV1 and FVC, we did not find interactions between their GRSs and smoking status. Results were similar for interactions between the GRSs and asthma status: present only for FEV1/FVC. FEV1/FVC is an index of airflow obstruction which is a characteristic of asthma and COPD and occurs with smoking.37 Significant interactions between GRS and smoking or asthma for only FEV1/FVC may reflect the fact that this parameter is independent of lung size. Genetic effects on FEV1 and FVC, which reflect lung size, may have a predominant impact through lung development, which takes place largely in early life, rather than later response to environmental exposures or diseases. We also note that Aschard et al,24 who examined both FEV1 and FEV1/FVC, identified an interaction between GRS and smoking predominantly for FEV1/FVC.
To our knowledge, our study is the first to examine interactions between GRS of pulmonary function traits and asthma or house dust endotoxin exposure. Aschard et al found a significant interaction on FEV1/FVC between an unweighted GRS based on 26 loci and ever versus never smoking, although this finding did not replicate in two independent datasets.24 In the larger meta-analysis of Shrine et al, a single GRS based on 279 SNPs weighted by the effect sizes for FEV1/FVC was constructed. That GRS did not interact with smoking status dichotomised as ever versus never.8 We constructed a separate GRS based on the 278 of the 279 SNPs present in our data and tested for its interaction with smoking status (current, former vs never) in relation to FEV1/FVC. The interaction effects with smoking status were not significant (former smokers: pinteraction=0.11, current smokers: pinteraction=0.20). However, using the more standard approach of creating a GRS based on clumping plus p value thresholding, we observed a significant interaction between our 1691-SNP GRS and smoking status in relation to FEV1/FVC. This observation also highlights the advantage of using clumping plus p value thresholding to create a GRS over simple selection of top SNPs as discussed by Choi et al.38 Shrine et al did not divide ever smokers into former and current for the interactions with GRS in their study. After several years from quitting, the decline in pulmonary function in former smokers tends to level off, so it is important to consider ever smokers in more detail. In our study, rather than creating just one weighted GRS, we created a separate GRS for each pulmonary function trait weighted by the effect sizes for that trait. Our GRSs were based on the same large comprehensive GWAS meta-analysis as Shrine et al,8 and we found evidence of interaction with smoking considering former and current smokers separately. The interaction was most notable in our data for current smokers relative to never smokers.
Our study has some limitations. Because asthma was categorised based on questionnaires, misclassification with COPD is possible. We did not adjust for socioeconomic status (SES). Occupation is often used to adjust for SES. Our participants were enrolled in the parent cohort because they were either farmers or spouses of farmers. By sharing an occupation, they would be regarded as having similar SES. Nevertheless, when we considered education as an alternate proxy for SES, the results did not materially change. Consistent with other genetic studies of pulmonary function, we did not adjust for comorbidities. However, if insufficient adjustment for SES or comorbidities can bias estimates of interaction with the GRS, we cannot exclude the possibility that this occurred. Because this is an agricultural population, participants potentially had higher exposure to endotoxin than the general US population. Additionally, all participants in this study and those in the UK Biobank and the SpiroMeta consortium were of European ancestry. Further, variants included in the GRS have different directions of associations with the pulmonary function traits. Although we recoded these directions to be uniform, combining the variants into a GRS might lose some information. However, assessing interactions using GRS provides greater statistical power than using individual variants.
In most GWAS of pulmonary function, even though multiple correlated traits are examined simultaneously, correction for multiple testing based on the number of traits examined is not usually done.8 9 There are few GWASs focusing on interaction hypotheses. We used a nominal p value of 0.05 for reporting significant interactions. If one were to adjust interaction p values for the three traits and three exposures considered, the p value threshold would be 0.05/9=0.006. At this stricter correction, none of our interaction findings would be significant. Thus, caution is required in the interpretation of our results pending replication in future studies.
A strength of the study is that we developed a separate GRS for each pulmonary function trait using a meta-analysis involving around 400 000 participants of European ancestry,8 the largest GWAS of pulmonary function to date. This large-scale meta-analysis enabled generation of authoritative risk scores for pulmonary function in ALHS; we used these to investigate whether reduced pulmonary function associated with genetic risk is magnified in the presence of smoking or other exposures that have been related to reduced pulmonary function.
In conclusion, we developed separate GRSs for three pulmonary function traits in our study of asthma nested within an agricultural cohort. We identified significant interactions for FEV1/FVC between its GRS and smoking status and marginally significant interactions for FEV1/FVC between its GRS and asthma. Our data support the use of GRS to identify environmental interactions with genetic susceptibility. Although small numbers induced by further stratification require caution, we saw some evidence that, for FEV1/FVC, the interaction between its GRS and smoking status differed by asthma and by gender. While it has been difficult to identify appreciable evidence of gene by environment interactions in genome-wide analyses at the individual SNP level, combining data across SNPs from large-scale GWAS through the use of GRSs can identify such interactions. Using the GRS approach, we find evidence that the impact of genetic susceptibility on reduced FEV1/FVC is enhanced in the presence of smoking or asthma. These findings provide evidence that the population with higher genetic risk for impaired pulmonary function is more susceptible to the deleterious effects of smoking and asthma. Our findings might hint at potential biological mechanisms underlying the interactions between genetic variants and exposure to smoking, or presence of asthma, in relation to lung function. For example, significant interactions between genetic risk for reduced pulmonary function and smoking might suggest that some SNPs related to pulmonary function operate by influencing pathways for response to smoking, even though previous analyses of interaction with the individual SNPs have not identified significant interactions. Studies incorporating additional types of omics data, including proteomics and metabolomics, might help shed light on possible mechanisms. Future studies assessing interaction between GRSs and factors related to reduced pulmonary function would help to support stronger inferences regarding potential relevance in clinical practice.
Data availability statement
Data are available upon reasonable request pending all required approvals.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the institutional review board at the National Institute of Environmental Health Sciences.
Acknowledgments
We thank Dr Jane Hoppin, ScD (North Carolina State University, Raleigh North Carolina), for her important contribution to the Agricultural Lung Health Study during her tenure at the National Institute of Environmental Health Sciences (NIEHS); the numerous study staff at Social & Scientific Systems, Inc, who played a role in the data collection; Dr Frank Day of NIEHS and Dr Jianping Jin of Westat, Inc (Durham, North Carolina), for computational support; and Huiling Li of NIEHS for careful review of the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SS and SJL designed the study and drafted the manuscript. SS performed data analysis with contributions from ABW, MKL, TTH and MR. JLH was responsible for quality control of the pulmonary function data. PST was responsible for the endotoxin measurements. DMU and AM-R provided statistical guidance. All authors provided critical input on the manuscript.
Funding This work was supported by the Intramural Research Programme of the National Institutes of Health, National Institute of Environmental Health Sciences (Z01-ES102385, Z01-ES049030, Z01-ES043012 and, for ABW, contract number HHSN273201600003I) and the National Cancer Institute (Z01-CP010119), and was supported in part by American Recovery and Reinvestment Act funds through National Institute of Environmental Health Sciences (contract number N01-ES-55546). PST was supported by PHR-SUPS2-S-10–00179 and NIH P30 ES005605.
Competing interests AM-R and PST report grants from the National Institute of Environmental Health Sciences during the conduct of the study.
Provenance and peer review Not commissioned; externally peer reviewed.