Article Text

Abstract
Background Climate change increases global mean temperature and changes short-term (eg, diurnal) and long-term (eg, intraseasonal) temperature variability. Numerous studies have shown that mean temperature and short-term temperature variability are both associated with increased respiratory morbidity or mortality. However, data on the impact of long-term temperature variability are sparse.
Objective We aimed to assess the association of intraseasonal temperature variability with respiratory disease hospitalisations among elders.
Methods We ascertained the first occurrence of emergency hospital admissions for respiratory diseases in a prospective Chinese elderly cohort of 66 820 older people (≥65 years) with 10–13 years of follow-up. We used an ordinary kriging method based on 22 weather monitoring stations in Hong Kong to spatially interpolate daily ambient temperature for each participant’s residential address. Seasonal temperature variability was defined as the SD of daily mean summer (June–August) or winter (December–February) temperatures. We applied Cox proportional hazards regression with time-varying exposure of seasonal temperature variability to respiratory admissions.
Results During the follow-up time, we ascertained 12 689 cases of incident respiratory diseases, of which 6672 were pneumonia and 3075 were COPD. The HRs per 1°C increase in wintertime temperature variability were 1.20 (95% CI 1.08 to 1.32), 1.15 (1.01 to 1.31) and 1.41 (1.15 to 1.71) for total respiratory diseases, pneumonia and COPD, respectively. The associations were not statistically significant for summertime temperature variability.
Conclusion Wintertime temperature variability was associated with higher risk of incident respiratory diseases.
- COPD epidemiology
- pneumonia
Statistics from Altmetric.com
Key messages
What is the key question?
Is seasonal temperature variability associated with increased risk of respiratory disease hospitalisations among elders?
What is the bottom line?
Wintertime temperature variability was associated with higher risks of incidence of total respiratory diseases, pneumonia and COPD and such associations were stronger in females and participants in a lower social-economic position.
Why read on?
This large prospective cohort study is the first to show the impact of seasonal temperature variability on respiratory diseases admissions, and it highlights the potential role of changing seasonal temperature variability introduced by climate change on respiratory system.
Introduction
Respiratory diseases, including pneumonia and COPD, contribute to substantial health burden worldwide. Pneumonia affects approximately 450 million people a year and is a leading cause of hospitalisation and death worldwide.1 A total of 3.2 million people died of COPD in 2015, which is the fourth leading cause of death in the world.2
It is now well recognised that climate change has increased global temperature over the past few decades, primarily due to the increased emissions of anthropogenic greenhouse gases.3 Climate change is also projected to cause changes in the frequency, severity and duration of extreme weather events, including changing temperature variability in short-term (eg, diurnal temperature range) and long-term (eg, intraseasonal) ways.4–7 It is expected that climate change will affect respiratory diseases significantly through influencing viral activity and transmission (eg, respiratory syncytial virus), altering vectors and the host immune response and changing in allergen disposition.8 9
Mean and variability are two main characteristics of temperature. Numerous time-series and case-crossover studies have reported that short-term exposure to both cold and hot temperatures were associated with increased risks of respiratory mortality10 and hospital admissions.11 Most of those studies focused on the adverse health effects of short-term mean temperature. A few studies also assessed the health effects of short-term temperature variability (eg, diurnal temperature range and temperature change between neighbouring days or diurnal temperature range). For example, Lim et al 12 reported that diurnal temperature range was significantly associated with respiratory hospitalisations using four metropolitan areas in Korea with a total population of 18.3 million. To the best of knowledge, no study has been conducted to investigate the impacts of seasonal (long-term) temperature variability on incident respiratory disease hospital admissions.
The present study aimed to estimate the association between seasonal temperature variability, the SD of daily mean summer (June–August) or winter (December–February) temperatures and the incidence of respiratory disease hospital admissions in a prospective Chinese elderly cohort in Hong Kong. We also assessed whether the associations were modified by age, sex, marital and socioeconomic status and housing type to identify vulnerable subpopulations.
Methods
Study population
The Chinese elderly cohort in Hong Kong is a prospective cohort, into which all residents of Hong Kong aged 65 years or older (≥65 years) were eligible to enrol. From 1998 to 2001, 66 820 elders, about 9% of older people in Hong Kong, enrolled in the 18 Elderly Health Centres of the Department of Health, one in each of the 18 districts in Hong Kong, and were followed up until December 2010. Each participant had physical examinations and face-to-face interviews by registered nurses or doctors using a standardised structured questionnaire during each year of follow-up.13 The collected information included demographic characteristics (eg, age and sex), socioeconomic status (eg, personal monthly expenditure), lifestyle (eg, smoking status and physical activity) and body mass index (BMI). Details of this cohort profile were described elsewhere.13
Health outcomes
We used a common unique identifier (the Hong Kong identity card number) to link the cohort with the Hospital Authority Corporate Data Warehouse, which covers all publicly funded hospitals that provide 24-hour accident and emergency services and covers 90% of hospital beds for Hong Kong residents.14 Hospital admissions were identified using primary discharge diagnoses for emergency hospital admissions for respiratory diseases (International Classification of Diseases, Ninth Revision: 460:519), pneumonia (480:486, 487.0) and COPD (490:492, 494:496). Incident cases for respiratory diseases were ascertained as the first occurrence of emergency hospital admissions after enrolment.
Ambient temperature
We extracted daily mean ambient temperature data from the 22 weather monitoring stations in Hong Kong within a land area of 1104 km2 from 1998 to 2010 (figure 1). Among various algorithms (eg, kriging, inverse distance weighting and trend surface analysis) to spatial interpolate daily mean ambient temperature, the kriging method yields a more realistic spatial behaviour of the climatological variable of interest.15 16 Ordinary kriging is the most commonly used kriging method, which estimates daily temperature at locations without monitors based on the weighted average of adjacent observed sites within a given area. Ordinary kriging has been described as the ‘anchor algorithm of geostatistics’ because of its remarkable robustness under a range of conditions.17 We used ordinary kriging to interpolate the daily ambient temperature based on the 22 weather monitoring stations for each participant according to his or her residential address. The performance of the ambient temperature prediction model was validated by leave-one-out cross-validation. The R2 of leave-one-out cross-validation was found to be very high (R2=0.93). We then calculated the SD of daily mean summer (June–August) temperature (summertime temperature variability) and the SD of daily mean winter (December–February) temperature (wintertime temperature variability) for each participant’s residential address. High or low temperature variability was dichotomously defined as higher or lower than the median of seasonal temperature variability.

Locations of participants in the prospective Chinese elderly cohort (n=61 446) at baseline (1998–2001) and weather monitoring stations (n=22) in Hong Kong.
Fine particulate matter (PM2.5) exposure
We estimated PM2.5 exposure based on Surface Extinction Coefficients (SEC) from aerosol optical Depth (AOD) retrieved from remote sensing data of the two National Aeronautics and Space Administration Earth Observing System satellites.18 AOD data were originally retrieved at a 10×10 km resolution and were refined into 1×1 km resolution by modifying the Moderate Resolution Imaging Spectroradiometer algorithm.19 The relationship between SEC and PM2.5 for each year from 1998 to 2010 was calibrated using grid cells with both SEC and PM2.5 measurements. This yearly calibration was then used to estimate PM2.5 at the residential location of each participant. The estimated PM2.5 concentrations have been used in earlier studies in this cohort to reveal the association of PM2.5 with mortality or hospital admissions.20–22
Individual and ecological covariates
We controlled for individual-level potential confounders, including age, sex, marital status, BMI, physical activity, housing type, education attainment, smoking status, medication taken and personal monthly expenditure. As tertiary planning units (TPUs) are the most commonly used units in the population census report in Hong Kong, we calculated the social deprivation index (SDI) to control for TPU-level social deprivation. Details for the calculation of SDI were described elsewhere.23 24 We also controlled for smoking rate (>15 years of age) at the district level.
Statistical analysis
We used Cox proportional hazards models to estimate the association between seasonal temperature variability and incident respiratory diseases. Survival time was calculated from enrolment date to the first hospital admission to respiratory diseases or death or 31 December 2010 (censoring), whichever came first. In order to separate the independent effects of summertime or wintertime temperature variability, we included yearly mean temperature and summertime and wintertime temperature variability simultaneously in the model and treated them as time-varying exposures. To do this, we used the counting process approach to the Cox proportional hazards model.25 We controlled for individual-, TPU- and district-level risk factors as mentioned above and included a linear term for year of follow-up to adjust for time trends. To allow for possible non-proportionality of hazard, age in years was treated as the stratification variable. We also examined age (≤70 years and >70 years), sex (female and male), marital status (married and unmarried), education attainment (below primary, primary and secondary or above), personal monthly expenditure (low, medium and high) and housing type (public and aided, private and others) as the potential modifiers of the effects of seasonal temperature variability by including an interaction term between seasonal temperature variability and one effect modifier at a time in the model, and p value of the interaction term was used to indicate statistical significance.
We performed a number of sensitivity analyses to test the robustness of our results. First, we used inverse distance weighting to spatially interpolate daily temperature for each participant, and then refitted the Cox proportional hazards regression model. Second, to control for competing diseases, we excluded participants who died or who had incidence of respiratory diseases during the first year after enrolment or excluded those who self-reported COPD/asthma at the baseline. Third, considering PM2.5 concentration may vary from year to year, we controlled for time-varying PM2.5 in addition to all potential confounders mentioned above. We did not control for PM2.5 in the main analysis as the role of air pollution on the association between ambient temperature and morbidity or mortality is complex and has not be fully elucidated.26 Fourth, participants might move their homes during the 10–13 years of follow-up, so we excluded participants who changed their home addresses. Finally, we tested the assumption of linearity for seasonal temperature variability by using natural cubic spline functions with three df.
The results were expressed as HR per 1°C increase in seasonal temperature variability. All analyses were conducted in R statistical environment V.3.3.0, with packages ‘geoR’ to interpolate individual’s daily ambient temperature using ordinary kriging methods and ‘survival’ for survival analysis to estimate the HR.
Results
A total of 66 820 older people were enrolled in the initial study cohort. After excluding participants without sufficient address information for geocoding or with missing covariates, a final sample of 61 446 (92.0%) was included in the final analyses. The spatial distribution of these 61 446 older people is shown in figure 1.
Table 1 shows the baseline descriptive characteristics of the 61 446 participants included in this study. The mean age at entry of this cohort was 72 years old and female participants accounted for 65.9%. A total of 14 168 (23.1%) participants’ BMI were less than 21.6, and 16 100 (26.2%) participants’ BMI were greater than 26.3. The majority of participants did physical activity seven days/week. About one-fifth (19.3%) were former smokers, and 9.6% were current smokers. About half of the participants (46.0%) had education attainment below primary. Nearly half of the participants (53.1%) took regular medication. Participants who were exposed to a higher wintertime temperature variability were more likely to be older, female, smokers and have lower personal monthly expenditure but less likely to have a secondary or higher education and live in private house when compared with those exposed to a lower wintertime temperature variability (table 1). There were no apparent long-term trends for yearly mean and seasonal mean temperatures from 1998 to 2010 based on temperatures monitored by the 22 weather stations (online supplementary figure S1).
Supplementary file 1
Descriptive characteristics of the prospective Chinese elderly cohort at baseline (1998–2001) by seasonal temperature variability
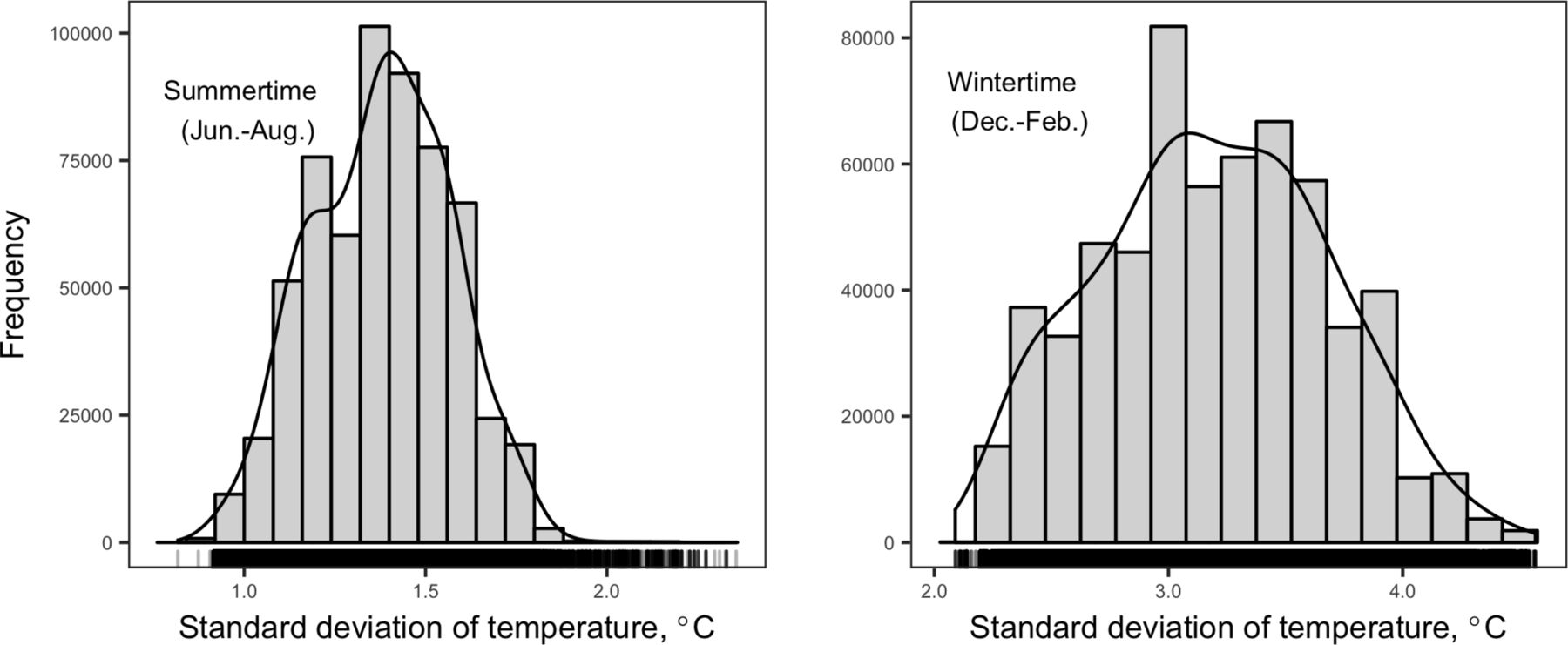
During the study period, summertime and wintertime temperature variability both approximated a normal distribution (figure 2) with mean SDs of 1.4°C and 3.2°C for summertime and wintertime, respectively. After 10–13 years of follow-up (from 1998 to 2010), there were 12 689 emergency hospital admissions for respiratory diseases, among them pneumonia and COPD accounted for 52.6% (6672) and 24.2% (3075), respectively (table 2).
{kind=link}
{kind=link}
Distribution of the SD of daily mean summer and winter temperatures.
HR and 95% CI per 1°C increase of seasonal temperature variability on incident respiratory diseases in the prospective Chinese elderly cohort in Hong Kong
Seasonal temperature variability and incident respiratory diseases
The associations of summertime and wintertime temperature variability with total incident respiratory diseases, pneumonia and COPD were presented in table 2. In the basic models stratified by age in years and adjusted for sex and year of follow-up, summertime temperature variability was not associated with increased risks of total incident respiratory diseases, pneumonia or COPD. The associations between wintertime temperature variability and incident respiratory diseases were all statistically significant. The HRs were modestly attenuated for summertime temperature variability in the fully adjusted models with additional adjustment for yearly mean temperature, marital status, housing type, BMI, education attainment, personal monthly expenditure, physical activity, medication taken, smoking status, SDI and smoking rate at the district level. For example, the fully adjusted HR for total respiratory diseases was 1.02 (0.80 to 1.29) compared with 1.12 (0.91 to 1.39) in the basic model. Results for wintertime temperature variability were also modestly attenuated in the full models but remained statistically significant. The HR was 1.20 (1.08 to 1.32) for total incident respiratory diseases, 1.15 (1.01 to 1.31) for pneumonia and 1.41 (1.15 to 1.71) for COPD per 1°C change in wintertime temperature variability in the fully adjusted models.
In this Hong Kong elderly cohort, about 11.1% elders changed home addresses during the follow-up period. Excluding those participants from the analysis did not change the Cox regression results substantially (online supplementary table S1). Sensitivity analyses excluding participants according to other criteria or further controlling for time-varying PM2.5 exposure gave similar results (table 3). We also used inverse distance weighting to spatially interpolate daily temperature for each participant and refitted the Cox proportional hazards regression, and we found results were similar to those using the ordinary kriging method (online supplementary table S2). By comparing the linear and natural cubic spline models, we did not find any evidence of departure from linearity for the association between seasonal temperature variability and respiratory diseases hospitalisations.
HR and 95% CI per 1°C increase of seasonal temperature variability on incident respiratory diseases in the sensitivity analyses
Effect modification for seasonal temperatures variability
We examined associations of seasonal temperature variability with incident respiratory diseases in the fully adjusted models stratified by age (≤70 years and >70 years), sex (female and male), marital status (married and unmarried), education attainment (below primary, primary and secondary or above), personal monthly expenditure (low, medium and high) and housing type (public and aided, private and others). No significant difference was observed by stratified characteristics, except for sex and personal monthly expenditure for the wintertime temperature variability (table 4). Female and those with lower personal monthly expenditures had greater HRs when exposed to wintertime temperature variability. Female also exhibited increased risk of respiratory hospitalisations after exposure to summertime temperature variability (online supplementary table S3).
HR and 95% CI per 1°C increase in wintertime temperature variability stratified by population characteristics in the prospective Chinese elderly cohort in Hong Kong, 1998–2010
Discussion
We found associations between wintertime temperature variability and total incident respiratory diseases, pneumonia and COPD among a prospective Chinese elderly cohort that accounted for about 9% of all elders in Hong Kong. Such associations were stronger in females and participants in a lower socialeconomic position. We did not find any association between summertime temperature variability and incident respiratory diseases.
In the literature, temperature variability within a day or a few neighbouring days has been consistently associated with respiratory mortality or hospitalisations.12 27–30 For example, diurnal temperature change was generally associated with emergency hospital admissions for total respiratory, pneumonia and COPD in four largest cities in Korea using a temperature-matched case-crossover study design.12 Zhan et al 28 used the National Morbidity, Mortality, and Air Pollution Study data from 106 communities of the USA during 1987–2000 to investigate the effect of temperature change between neighbouring days (TCNs) on mortality and found that prominent effects of TCNs on mortality for total respiratory, pneumonia and COPD diseases.
Temperature variability over a longer time duration (eg, intraseasonal), however, has rarely been studied for its potential health effects. We identified three epidemiological studies that had previously examined the health impacts of seasonal temperature variability, measured as the SD of intraseasonal temperature, and all of these studies focused on mortality.31–33 To our knowledge, this is the first study to link seasonal temperature variability with incident respiratory hospitalisations; thus, our findings may enrich our understanding towards the health impacts of seasonal temperature variability.
In our study, we found a positive association between wintertime temperature variability and incident respiratory diseases. This is consistent with previous studies using mortality as the health outcome. For example, Shi et al 32 reported that for each 1°C increase in SD of winter temperature associated with 4.1% (95% CI 3.0% to 5.2%) increases in annual deaths using Medicare data with 2.7 million residents aged 65 years and older for the years 2000–2008 in the New England region of the USA.
Summertime temperature variability was not associated with incident respiratory diseases in our analyses, which is inconsistent with previous studies.31 33 This difference may be due to differences in city climates. Multicity studies have suggested that warm regions or areas with moderate winter climates have more significant cold effects than hot effects.34 35 This phenomenon can be explained by long-term adaptation, as people in warm areas are generally more sensitive to cold weather.36 Hong Kong has a subtropical climate, of which the summer is hot and humid. Epidemiological studies have suggested that heat effects in Hong Kong are not that evident,14 37 38 possibly due to extensive use of air conditioning.
The biological mechanisms linking seasonal temperature variability with incident respiratory diseases have not been elucidated, although plausible explanations have been postulated. Temperature variability has been shown to affect the immune system’s capability to resist infectious agents and cause inflammatory nasal responses in patients with persistent allergic rhinitis, which may trigger respiratory events.39 40 Also, exposure to seasonal temperature variability has been reported to impede one’s ability to adapt to local climate, which may increase the likelihood of adverse health outcomes like respiratory diseases.41 42 For example, locations with larger seasonal temperature variability produced stronger associations between daily temperature and mortality.35 43
We found greater effects of wintertime temperature variability among females, which is consistent with previous short-term temperature variability studies.44–46 The reason for that is probably due to biological difference. We found elders with lower personal monthly expenditure were more sensitive to increased wintertime temperature variability. Low personal monthly expenditure is regarded as an indicator of low socioeconomic position. The increased vulnerability of people with low socioeconomic status may be related to poor baseline health status, limited access to healthcare and poor living conditions.46 47
This study has some limitations. First, we obtained first occurrence of hospital admissions for respiratory diseases after enrolment. Respiratory disease hospitalisations prior to enrolment were not available so we could not identify participants who previously had respiratory diseases. However, sensitivity analysis excluding the participants with self-reported COPD/asthma at baseline gave similar estimates, which confirmed the robustness of our findings. Second, participants were volunteers; all residents aged 65 years or older were eligible to enrol. Thus, the participants in this study cohort could be more health conscious than the rest of the elderly population in Hong Kong.13 Third, the observed association between seasonal temperature variability and respiratory disease admissions might relate to the residents’ perception of temperature modified by humidity and wind chill, for which not any fine resolution spatial data are available yet. Finally, individual household adaptation behaviours, such as heater or air conditioner usage, may affect the residents’ personal exposure to seasonal temperature variability, measured only by outdoor weather stations. Although we did include house type in the regression model, it is still possible that the observed associations might be affected by temperature exposure misclassification. Despite these limitations, this is one of the few studies to examine the impacts of seasonal temperature variability on hospitalisations. Our findings might help better understand the impacts of climate change.
In conclusion, this study provides evidence that wintertime temperature variability increases the risks of incident total respiratory, pneumonia and COPD in older people. These findings should help better understand the health impacts of climate change.
Acknowledgments
We would like to thank The Elderly Health Service of the Department of Health for providing the cohort data, the Hospital Authority for providing the hospital admission data and the Environmental Protection Department for providing the air pollution data.
References
Footnotes
Contributors FL and LT contributed to the conception and design and interpreted the results; RSL and CMW collected the cohort data; SS and HQ conducted statistical analyses; SS, FL, JEH, YW and LT drafted the manuscript for important intellectual content. All authors critically reviewed and accepted the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Ethics approval was obtained from the Ethics Committee of the Faculty of Medicine, The University of Hong Kong and of the Department of Health of Hong Kong.
Provenance and peer review Not commissioned; externally peer reviewed.