Article Text

Abstract
There is evidence to demonstrate the ongoing symptoms of COVID-19; however, there are currently no agreed outcomes to assess these symptoms. This study examined the use of the chronic obstructive pulmonary disease (COPD) assessment test (CAT) for patients recovering from COVID-19. 131 patients who were admitted with COVID-19 were followed up over the phone to assess symptoms. The median (IQR) CAT score was 10 (5–16). Cough, phlegm and chest tightness domains were within range for healthy people, but there was evidence of significant breathlessness, loss of energy, and activity and sleep disturbance. The CAT is a useful tool to assess symptoms of COVID-19 recovery.
- pulmonary rehabilitation
- respiratory infection
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Symptoms due to the SARS-CoV-2 (COVID-19) are varied but the chief respiratory symptoms are cough, sputum and breathlessness.1 It is not clear how long these specific symptoms persist after the initial acute event but it is becoming clear that some patients will have complex rehabilitation needs.1 2 Due to the novel nature of the disease, there are no outcome measures specifically designed to assess patients following COVID-19. The chronic obstructive pulmonary disease (COPD) assessment test (CAT) is an eight-item questionnaire designed to assess common COPD symptoms but has been used in many respiratory diseases and is widely used within respiratory medicine and pulmonary rehabilitation.3 It uses an eight-point differential item response scale to assess: cough, sputum, chest tightness, breathlessness, activity limitation, confidence leaving the home, sleep and energy. These domains have significant overlap with the commonly reported symptoms for patients experiencing COVID-19. The CAT has been used in healthy subjects in whom the mean score was 6.9 (SD 6.2),3 with 83% of healthy volunteers screened having a CAT score of <10.4 These normative data allow us to assess patients with COVID-19 in the absence of a previous CAT score. The aim of this study was to assess the use of the CAT total and item scores in patients recovering from COVID-19 in order to assess symptom-based needs.
Methods
This was an observational cohort study of patients discharged from hospital following an admission of COVID-19, either by positive swab or clinical diagnosis. All patients admitted with COVID-19 to the University Hospitals of Leicester were eligible for this study. Patients were followed up by a phone consultation after discharge to assess symptoms and rehabilitation needs. Participants were excluded if their primary cause for admission was not COVID-19 or its related symptoms. They were recruited and completed the CAT over the phone. Participants also completed the Functional Assessment of Chronic Illness Therapy (FACIT)5 and Hospital Anxiety and a Depression Scale (HADS)6 questionnaire, alongside baseline demographic information and self-reported physical activity (categorised as no exercise experience, exercised previously but not currently or currently undertakes exercise, or reports 30 min of activity per day for 5 days). Information was collected about their admission including hospital bed days and number of days ventilated.
Data were analysed using SPSS V.25. Associations between length of stay, ventilation status and questionnaires and CAT total and item scores were tested using Spearman’s rank order correlation.
Results
One hundred and thirty-one patients were recruited, 30.5% had a pre-existing respiratory condition, mainly asthma (15.3%) and COPD (9.9%). The mean (SD) time to telephone call post discharge was 32 (18) days. Participants were predominantly men (58.8%) with a mean (SD) age of 60 (14) years. The average length of stay was 10 (12) days with 21 (16%) patients requiring ventilation (invasive n=18 or non-invasively n=3). One-third of which, (34%) had a pre-existing respiratory condition and the mean (SD) number of comorbidities was 1.9 (1.5), ranging from 0 to 7.
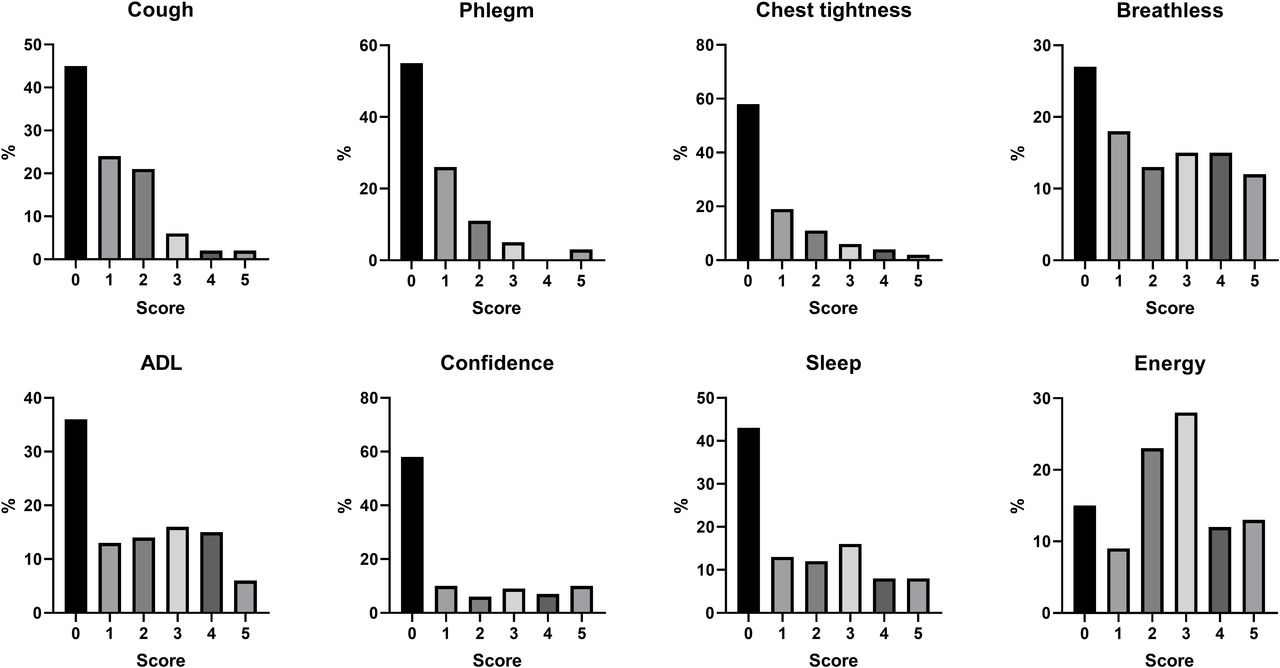
Median (IQR) CAT total and item scores are shown in table 1 and figure 1. In the whole population, 52% had CAT total scores ≥10. Of the patients with no pre-existing lung disease 42% had score ≥10, and in the patients with pre-existing lung disease this proportion was 75%.
Mean (SD) for all patients and split by presence or absence of pre-existing respiratory disease

Percentage of participants scoring 0–5 per domain of the COPD assessment test. ADL, activities of daily living; COPD, chronic obstructive pulmonary disease.
There were no statistically significant correlations with the CAT with length of stay (r=−0.07, p=0.41), number of days ventilated (r=0.10, p=0.69) or FACIT (r=0.05, p=0.57). There were statistically significant moderate correlations with the HADS anxiety (r=0.51, p<0.01) and depression (r=0.57, p<0.01) scores and self-reported physical activity (r=0.26, p<0.01). There were no correlations between CAT score and time between discharge and telephone call (r=−0.14, p=0.13) (figure 2) or time between admission and follow-up call (r=0.07, p=0.46). The mean (SD) FACIT Score was 27.7 (13.9) with n=58 (54%) demonstrating ‘severe fatigue’, but there were no statistically significant differences in those with/without severe fatigue in length of stay, number of days ventilated, CAT total or item scores, or HADS.

{kind=link}
{kind=link}
COPD assessment test (CAT) total score and time to phone call from discharge. COPD chronic obstructive pulmonary disease.
Discussion
These results demonstrate a high CAT total score for patients following an admission of COVID-19. Symptoms relating to the airways (cough, phlegm and chest tightness) scored close to previously reported healthy persons of a similar age4; however, those with a pre-existing respiratory disease had higher phlegm scores. In contrast, breathlessness, activity limitation, confidence to leave the home, sleep and energy were worse, even in patients with no previous diagnosed lung disease. Confidence leaving the house appears to be a concern, but this should be framed in the context of lockdown and social distancing measures, so it is difficult to ascribe causality to this item score. There was a relationship between CAT and anxiety and depression and it is possible that a higher burden of symptoms can lead to anxiety and depression but also anxiety and depression may lead to increased severity of symptoms. Unlike other critically ill patients, patients with COVID-19 are exposed to mass media reporting of their condition and the impact this may have on symptom reporting or anxiety and depression is unknown.
Patients with pre-existing lung disease were more likely to have CAT scores ≥10 than those without due to more breathlessness, activity limitation and sleep disturbance, but loss of energy was similar in the two groups. This similarity is unlikely to be due to a ‘floor effect’; since the scoring range for each item is 0–5 and scores are ≈2.6 for both groups. We conclude that poor energy is principally due to the post-COVID-19 state.
The time to follow-up call from discharge varied between patients, with a large SD and while we may have expected a trend to reducing symptoms over time, the length of follow-up did not affect the results. This suggests either limited/slow natural recovery or potentially higher initial CAT scores if patients were followed up earlier. The time to first contact was affected by staffing and high numbers of discharge early on. Follow-up would ideally be within 1 week of discharge. The study sample demonstrated a higher presence of respiratory conditions and a younger group than previously reported. This sample was representative of those who were admitted to the University Hospitals of Leicester, which is a specialist respiratory centre and may explain the increased presence of pre-existing respiratory disease. As this was an observational cross-sectional analysis, the change in CAT score over time is yet to be explored. Additionally, the CAT was administered over the phone; however, it has previously been demonstrated to have high validity when conducted over the phone, which is comparable to face to face administration.7 This study explored the use of the CAT in previously hospitalised patients and its exploration in patients with COVID-19 (symptoms or diagnosis) in the community is important, given that their experiences may be different; however, it is quick and easy to administer and could add value to assessments in primary care and the community.
The results of this study demonstrate higher reported symptoms for four out of eight items on the CAT and that total scores ≥10 were seen in over half of patients including those without previous lung disease. Global Initiative for Chronic Obstructive Lung Disease8 has recommended that CAT scores ≥10 in patients with COPD should be the threshold for maintenance treatment in COPD. While the CAT score can assess needs for rehabilitation, there is no defined threshold for patients whom might benefit from intervention post-COVID-19. It is important that a recovery programme addresses all aspects of the condition including anxiety and depression. There is an established minimal clinical important difference of two points in patients with COPD9; however, the application of this to a COVID-19 needs to be assessed due to social influences on symptom perception and expectations of treatment benefit in this condition. While the CAT can be used to guide treatment but further research is needed to identify impact of interventions.
The CAT can provide insight into the severity of symptom burden for patients following a hospitalisation for COVID-19 and could be considered to assess ongoing symptoms following COVID-19.
Footnotes
Twitter @EnyaDaynesPT
Contributors ED and SJS developed the protocol. ED, CG and SB-P contributed to the data collection. The data analysis was completed by ED with support from PJ and SJS. All authors contributed to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PJ is an employee of GSK.
Patient consent for publication Not required.
Ethics approval It is a substudy of the Training to Improve Dyspnoea Study (ISRCTN ISRCTN45695543) and gained ethical approval in May 2020 (REC number 17/EM/0156).
Provenance and peer review Not commissioned; externally peer reviewed.