Article Text

Abstract
Objectives Improved biomass cookstoves may help reduce the substantial global burden of morbidity and mortality due to household air pollution (HAP) that disproportionately affects women and children in low and middle income countries (LMICs).
Design Systematic review and meta-analysis of (quasi-)experimental studies identified from 13 electronic databases (last update: 6 April 2018), reference and citation searches and via expert consultation.
Setting LMICs
Participants Women and children
Interventions Improved biomass cookstoves
Main outcome measures Low birth weight (LBW), preterm birth, perinatal mortality, paediatric acute respiratory infections (ARIs) and COPD among women.
Results We identified 53 eligible studies, including 24 that met prespecified design criteria. Improved cookstoves had no demonstrable impact on paediatric lower ARIs (three studies; 11 560 children; incidence rate ratio (IRR)=1.02 (95% CI 0.84 to 1.24)), severe pneumonia (two studies; 11 061 children; IRR=0.88 (95% CI 0.39 to 2.01)), LBW (one study; 174 babies; OR=0.74 (95% CI 0.33 to 1.66)) or miscarriages, stillbirths and infant mortality (one study; 1176 babies; risk ratio (RR) change=15% (95% CI –13 to 43)). No (quasi-)experimental studies assessed preterm birth or COPD. In observational studies, improved cookstoves were associated with a significant reduction in COPD among women: two studies, 9757 participants; RR=0.74 (95% CI 0.61 to 0.90). Reductions in cough (four studies, 1779 participants; RR=0.72 (95% CI 0.60 to 0.87)), phlegm (four studies, 1779 participants; RR=0.65 (95% CI 0.52 to 0.80)), wheezing/breathing difficulty (four studies; 1779 participants; RR=0.41 (95% CI 0.29 to 0.59)) and conjunctivitis (three studies, 892 participants; RR=0.58 (95% CI 0.43 to 0.78)) were observed among women.
Conclusion Improved cookstoves provide respiratory and ocular symptom reduction and may reduce COPD risk among women, but had no demonstrable child health impact.
Registration PROSPERO: CRD42016033075
- COPD epidemiology
- paediatric lung disaese
- pneumonia
- clinical epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
Pending the much-needed transition to using cleaner fuels, can improved cookstoves help reduce morbidity and mortality due to household air pollution (HAP) from biomass combustion among women and children in low and middle income countries?
What is the bottom line?
Meta-analyses indicate that improved biomass cookstoves can decrease respiratory and ocular symptoms among women; no demonstrable impact on perinatal or child health was observed.
Why read on?
This is the first meta-analysis assessing the health impact of improved cookstoves, providing valuable information for agenda setting to reduce the substantial global burden of morbidity and mortality from HAP.
Introduction
Solid biomass fuel is used as a primary cooking source by more than half of the world’s population.1–3 About three-fourths of this use occurs in low and middle income countries (LMICs).1 The combustion of biomass fuels results in pollutants such as carbon monoxide (CO) and particulate matter (PM), creating household air pollution (HAP) when produced inside.2 HAP results in a high burden of morbidity and mortality globally, disproportionately affecting LMICs.1–5 Globally, HAP was estimated to have caused 2.8 million deaths and 85.6 million disability-adjusted life years in 2015.4
In LMICs, women are traditionally at home taking care of the household, cooking and tending to the children, whereas men usually work during the day, away from home. Young children are often carried on their mothers' back while the latter carry out household chores inside.3 6 As a result, women and young children are particularly exposed to HAP from cooking and heating and are therefore at highest risk of developing HAP-associated adverse health conditions.2 Several studies have linked maternal exposure to biomass smoke during pregnancy to increased risks of stillbirth, preterm delivery, low birth weight (LBW) and other adverse health effects.7–9 Exposure to biomass smoke furthermore increases the risk of respiratory infections among children and of COPD in adults.3 7
Switching the use of biofuels for cooking purposes towards clean(er) fuels such as liquefied petroleum gas, electricity or solar energy would be the preferred solution to reduce HAP and improve population health.3 10 11 However, this transition is difficult in low income countries, due to lack of infrastructure, financial constraints and poor living conditions of households.1 10 11 As a result, an estimated 1.8 billion people will still be reliant on solid biomass for cooking by 2040.1 It is therefore essential that alongside facilitating the transition to cleaner fuel options, other measures continue to be developed, tested and—when successful—implemented to reduce HAP from cooking using solid biomass.5 Such biomass cookstove improvements include, for example, adding chimneys and using better combustion centres to increase efficiency. Biomass cookstove improvements are currently more cost-effective than switching to cleaner fuels and may be the only affordable short-term solution to reduce HAP for billions of people living in LMICs.3 11 12
Several studies have examined the effectiveness of improved biomass cookstoves in reducing HAP and improving health outcomes among its users, yielding seemingly inconsistent findings.3 11 13 14 Given the substantial global burden of death and disease associated with HAP and the significant contribution of biomass combustion—both current and projected—to this burden, a comprehensive assessment of the available evidence on the effectiveness of biomass fuel cookstove improvements in terms of health benefits is urgently needed. This will provide essential information to policy-makers to guide implementation of measures to reduce the burden from HAP associated with biomass combustion in LMIC areas where transition to cleaner fuels is not yet feasible. We conducted a comprehensive systematic review and meta-analysis to investigate the effectiveness of improved cookstoves to reduce adverse pregnancy outcomes and adverse health outcomes in women and children, as well as HAP exposure.
Methods
Protocol and registration
The systematic review protocol is registered with PROSPERO (CRD42016033075) and can be accessed at http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016033075.
Eligibility criteria
Following Cochrane Effective Practice and Organisation of Care (EPOC) guidelines,15 we included randomised controlled trials (RCTs), non-randomised controlled trials (NRCTs) and quasi-experimental studies (ie, controlled before–after (CBA) studies and interrupted time-series studies) studying the impact of an improved biomass cookstove on pregnancy outcomes, child and/or women’s health and/or exposure to HAP. We also identified any studies addressing the research question that had a longitudinal design but did not fit EPOC criteria. Studies were eligible when they were conducted in LMICs and included women aged 15–65 years and/or children aged 0–14 years. Any study in which more than 50% of the study population fulfilled these age criteria was included. From studies performed among the general population (ie, including men and women), only women were included, provided they had been analysed as a subgroup. Studies or study arms evaluating cookstoves that did not use solid biomass were not included.
Primary and secondary outcomes were selected based on their established associations with HAP and their relative contributions to the global burden of mortality and morbidity in the prenatal, paediatric and adult periods.3 4 7–9 16–18 The primary and secondary pregnancy, child and women outcomes are listed in table 1.
Information sources
We carried out a systematic and comprehensive bibliographic search using electronic databases: PubMed, EMBASE, Google Scholar, WHO Global Health Library (in addition to MEDLINE covering African Index Medicus, LILACS, Index Medicus for the Eastern Mediterranean Region, Index Medicus for South-East Asia Region, Western Pacific Region Index Medicus, WHO Library Database and Scientific Electronic Library Online) and the Cochrane Central Register of Controlled trials for relevant published studies, and the WHO International Clinical Trials Registry Platform for unpublished studies. References and citations of each eligible study were also checked by hand for additional studies that met our eligibility criteria. An expert in the field was approached in an attempt to identify any additional eligible studies.
Search
The initial search was conducted on 22 February 2016 and was updated on 6 April 2018. Full electronic searches for each database are provided in web supplementary appendix pages 2–3. No restrictions were imposed with regard to language in which the report was published or publication date.
Supplementary file 1
Study selection
The selection process consisted of two rounds: a selection based on title and abstract, and then screening of full-text articles for eligibility. Two reviewers (MT and PAWN) independently performed the searches and assessed eligibility. The final selection was based on consensus, with arbitration by a third reviewer (JVB or OCPvS) in the case of disagreement.
Primary and secondary outcomes
Data collection process
Two reviewers independently extracted relevant data from eligible studies (MT and PAWN for (quasi-)experimental studies; JFK and EAB for longitudinal observational studies) using a customised form based on the Cochrane Public Health Group data extraction form.19 Extracted data items were cross-checked between the reviewers, with any disagreement being resolved through consensus or via arbitration by a third reviewer if necessary (JVB or OCPvS).
Data items
A comprehensive set of data items was extracted, including full reference, publication type, year of publication, setting (country, rural vs urban), study design, duration of the study, sample size, type of intervention, type of control, type of participants, outcomes (including definition and measurement level/location) and follow-up time.
Risk of bias in individual studies
Two reviewers independently assessed the risk of bias in individual studies (MT and PAWN for (quasi-)experimental studies; JFK and EAB for longitudinal observational studies) using the Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies.20 Any disagreement was resolved by consensus or by consulting a third reviewer if necessary (JVB or OCPvS). Risk of bias was not used to determine eligibility of individual studies to be included in this review.
Summary measures
The following effect measures were extracted: numbers of participants with adverse outcomes by intervention allocation and corresponding ORs/risk ratios (RRs) for dichotomous outcomes; mean and SD and/or median and IQR for continuous outcomes within groups and corresponding between-group differences. Where possible, 95% CIs were calculated for each measure if these had not been provided in the article. If relevant data items were missing from reports, authors were contacted to obtain these.
Statistical analysis
Main findings from the systematic review, including characteristics and key findings of individual studies, are presented in tabular form. Where possible, we combined data from individual studies in random-effects meta-analysis. If authors adjusted for confounders, we selected the effect estimates of the most adjusted model presented. Effect estimates from cluster RCTs were combined with those from non-clustered studies only when the cluster RCTs had been analysed at the individual level, with clustering having been accounted for. One study reported separate effect estimates for two regions21; these were pooled using meta-analysis prior to pooling with effect estimates from other studies. Heterogeneity across studies was assessed both qualitatively as well as quantitatively using I2 test. Due to the low number of studies in individual meta-analyses, I2 results were not used to assess whether meta-analysis was appropriate. Risk of bias across studies was assessed visually using funnel plots when at least 10 studies were available for an outcome. We prespecified to conduct subgroup analyses for children under 5 years of age, and according to whether cooking was done in a separate kitchen. In an attempt to minimise risk of bias introduced by study designs with limited potential for attributing causality, our primary analyses were conducted using only (quasi-)experimental studies. In a sensitivity analysis for the primary outcomes, we conducted separate meta-analyses also including any longitudinal observational studies. All analyses were done with Stata SE 14.
Results
Study selection and characteristics
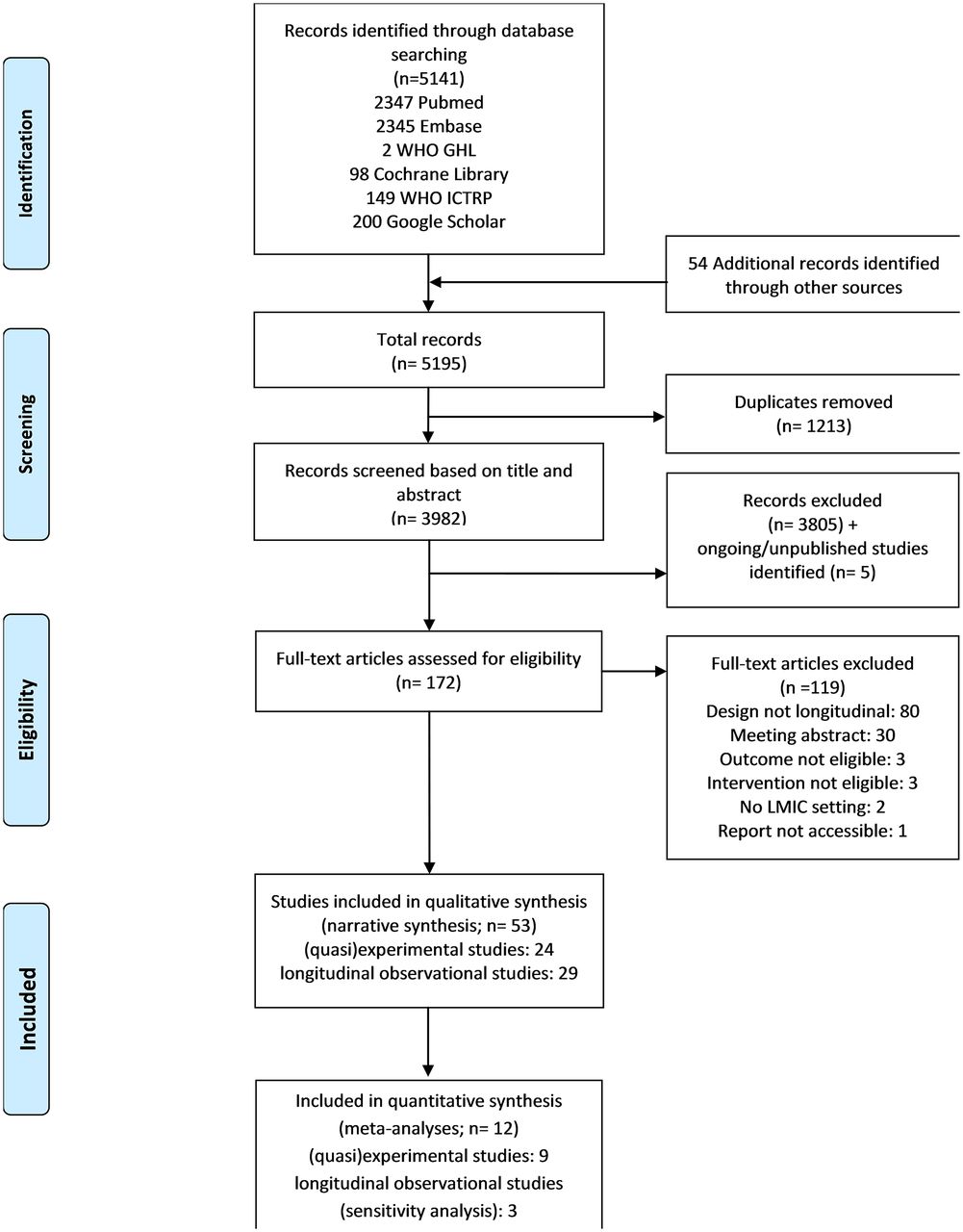
We screened 5195 records and identified 24 (quasi-)experimental and 29 longitudinal observational studies as eligible for inclusion in our review (figure 1). Five ongoing studies were identified (web supplementary appendix page 4). Study characteristics for (quasi-)experimental studies are provided in table 2 and for longitudinal observational studies in web supplementary appendix pages 5–14. Among the (quasi-)experimental studies, 21 were RCTs (six cluster RCTs),22–42 two were NRCTs21 43 and one was a CBA study.44 (Quasi-)experimental studies were conducted in rural areas across Asia, Africa and Central America: China (n=1),44 Ghana (n=2),24 31 Guatemala (n=9),25 28–30 36–39 43 India (n=2),26 42 Malawi (n=2),27 41 Mexico (n=3),5 31 33 Pakistan (n=1),21 Peru (n=1),40 Rwanda (n=1)34 and Senegal (n=2).22 23 Eight reports described findings from the RESPIRE trial in Guatemala,25 28–30 36–39 three were part of the same RCT in Mexico31 33 35 and two reports from Senegal described the same data.22 23 All studies had traditional stove use as control group, including open fires, three-stone stoves and brick, clay or coal stoves. The most common cookstove improvements were: better conservation of heat, optimised combustion centres and the addition of chimneys to vent smoke away (web supplementary appendix pages 15–16). Pregnancy outcomes were assessed in two studies,26 39child health outcomes in six studies26 28 36 40 41 43 and health outcomes among women in 16 studies.21 23–27 29 30 32–34 36 38 39 42 43 HAP was assessed at individual level in 14 studies (2 in children28 36; 11 in women24 25 27 29–32 36 38 39 42;and 1 in both women and children26) and at household level in 5 studies.21 31 34 36 44 The 29 longitudinal observational studies included in this review were carried out in rural settings across Latin America (11 studies),45–55 Asia (9 studies)56–64 and Africa (9 studies).65–73 Twenty-two were uncontrolled before–after studies,45–49 51 53–56 58–61 63 65 66 68–73 four were prospective cohort studies50 52 64 67 and three were retrospective cohort studies.57 61 62 Additional details on the longitudinal observational studies are provided in web supplementary appendix pages 5–14.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram outlining study selection. GHL, Global Health Library; ICTRP, International Clinical Trial Registry Platform; LMICs, low and middle income countries.
Characteristics of included (quasi-)experimental studies
Risk-of-bias assessment
Fourteen (quasi-)experimental studies were deemed to have a low risk of bias, nine had moderate and one had a high risk (web supplementary appendix pages 17–18). Among longitudinal observational studies, risk of bias was high for 4, moderate for 19 and low for 6 studies (web supplementary appendix pages 19–20).
Impact of improved cookstoves on primary outcomes
Primary analyses using (quasi-)experimental studies
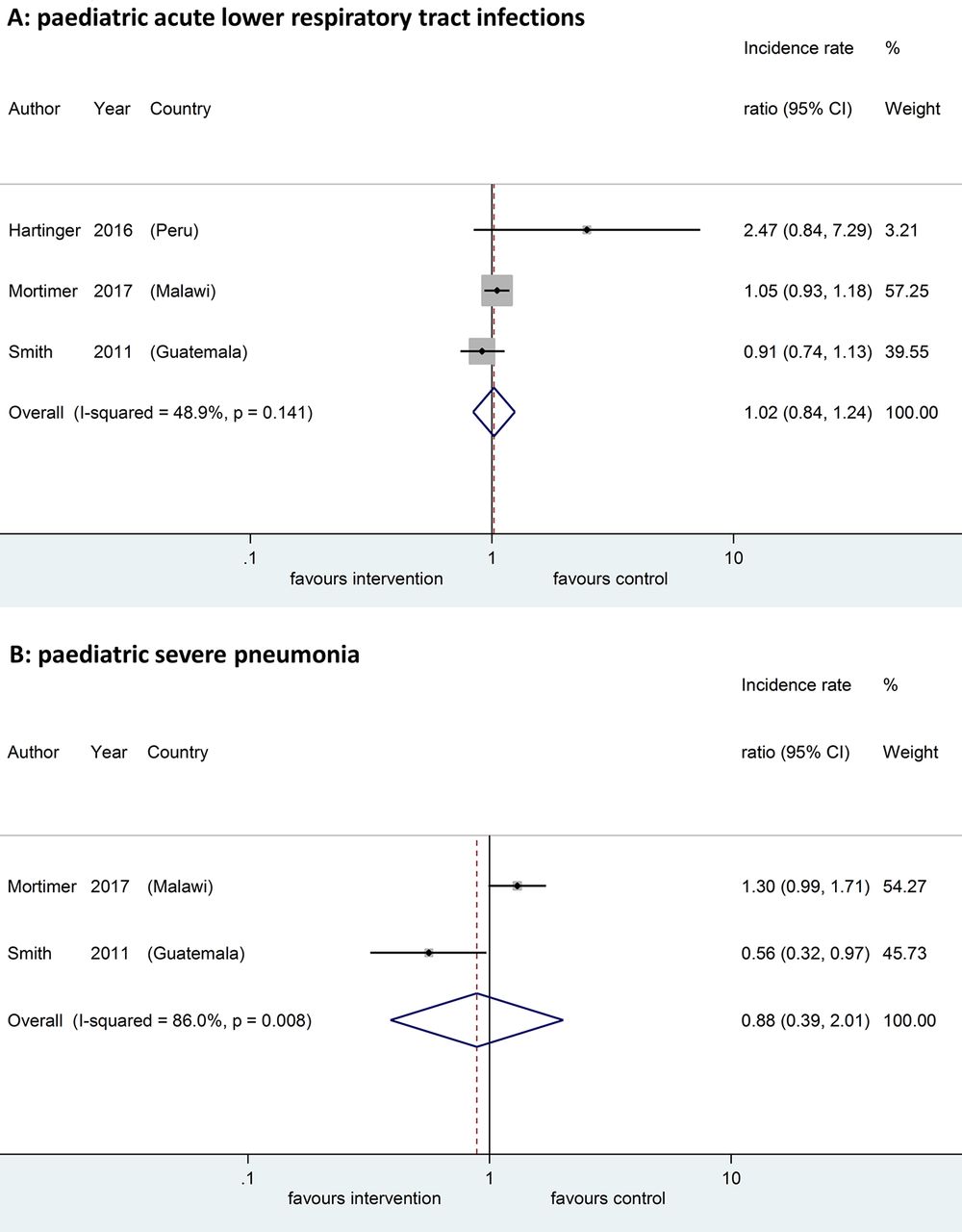
Six (quasi-) experimental studies reported effect estimates for the primary outcomes (table 3).26 35 37 39–41 All relevant cluster RCTs were analysed at the individual level and accounted for clustering; effect estimates could thus be combined with those from individual-level RCTs in meta-analyses. Among the primary outcomes, meta-analysis of (quasi-)experimental studies was only possible for paediatric acute respiratory infections (ARIs). There was no significant change in paediatric lower ARIs (including pneumonia; three studies, 11 560 children; incidence rate ratio (IRR): 1.02 (95% CI 0.84 to 1.24); figure 2A)37 40 41 or in severe pneumonia in meta-analysis (two studies, 11 061 children; IRR 0.88 (95% CI 0.39 to 2.01); figure 2B).37 41 In another study, improved cookstoves significantly decreased the duration of upper and lower respiratory infections (IRR 0.79 (95% CI 0.70 to 0.89) and IRR 0.41 (95% CI 0.21 to 0.80), respectively), with evidence of a dose–response relationship, with health impact in the intervention group being larger in households using mainly the improved cookstove versus those co-using the traditional cookstove.35

Meta-analyses of primary outcomes. (A) Acute lower respiratory tract infections in children and (B) severe pneumonia in children.
Primary outcomes of included (quasi-)experimental studies
No observable effects of cookstove improvements on LBW (174 babies; OR 0.74 (95% CI 0.33 to 1.66))39 or infant mortality, stillbirths and miscarriages (1176 babies; relative risk (RR) change 15% (95% CI –13 to 43))26 were seen in individual studies. No (quasi-)experimental studies assessed the impact of improved cookstoves on preterm birth or COPD among women. One study described a trend towards reduction in ‘respiratory system disease’ among women responsible for cooking who were allocated an improved cookstove: RR 0.51 (95% CI not reported, P=0.07).23 This was defined as cough, wheezing and/or difficulty breathing, and may in part reflect COPD.
Sensitivity analyses using (quasi-)experimental and longitudinal observational studies
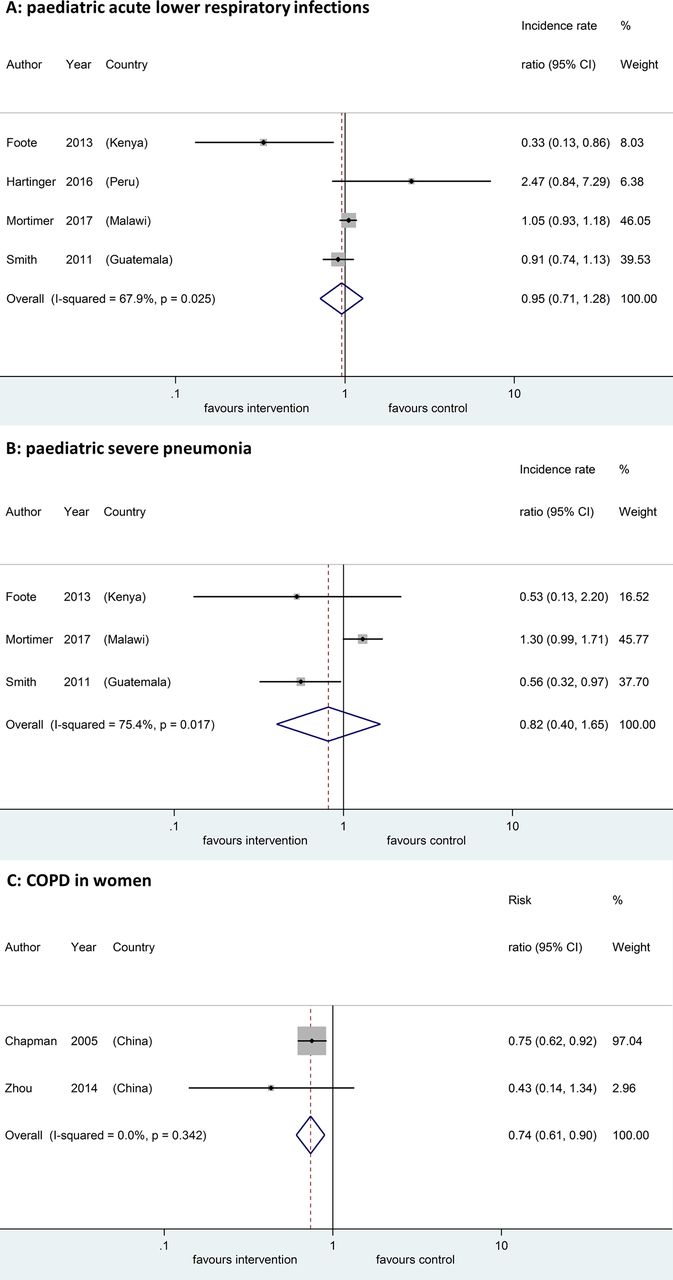
Consistent with our primary analyses, no significant impact of improved cookstoves on paediatric ARIs was observed in prespecified sensitivity analyses including findings from longitudinal observational studies (figure 3A and B). Improved cookstoves were, however, associated with a significant reduction in COPD among women when combining data from longitudinal observational studies: two studies,57 64 9757 participants; RR 0.74 (95% CI 0.61 to 0.90; figure 3C).

Sensitivity analyses of primary outcomes. (A) Acute lower respiratory tract infections in children; (B) severe pneumonia in children and (C) COPD in women.
Impact of improved cookstoves on secondary outcomes
Analyses using (quasi-)experimental studies
Effect estimates from (quasi-)experimental studies for the secondary outcomes are shown in web supplementary appendix pages 21–28. Meta-analyses were possible for birth weight (continuous scale) and maternal respiratory and ocular symptoms. Improved cookstoves had no statistically significant impact on birth weight in meta-analysis (two studies, 694 babies; difference in means: 82 g (95% CI –22 to 185 g; figure 4A).26 39 Meta-analyses indicated that, among women, improved cookstoves significantly reduced the incidence of cough (four studies21 24 27 33; 1779 participants; RR 0.72 (95% CI 0.60 to 0.87; figure 4B)), phlegm (four studies21 24 27 33; 1779 participants: RR 0.65 (95% CI 0.52 to 0.80); figure 4C), wheezing/breathing difficulty (four studies21 24 27 33; 1779 participants: RR 0.41 (95% CI 0.29 to 0.59); figure 4D) and conjunctivitis (three studies; 892 participants: RR 0.58 (95% CI 0.43 to 0.78), figure 4E).21 26 33

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analyses of secondary outcomes. (A) Birth weight (continuous scale); (B) cough in women; (C) phlegm in women; (D) wheezing/breathing difficulty in women and (E) conjunctivitis in women.
Other secondary outcomes were only described in individual studies or in ways that precluded meta-analyses to be performed. Improved cookstoves had no impact on child deaths due to respiratory disease in one study (IRR 0.76 (95% CI 0.17 to 3.37)).41 No significant impact on cough incidence or duration was observed among children in three studies,26 40 43 although in a subgroup analysis a significant reduction in cough duration was observed among girls in one study.43 CO exposure among children living in households with improved cookstoves was significantly decreased compared with controls in two reports from the same study (relative change in geometric means: −0.52% (95% CI −0.56 to −0.47)).28 36 The impact of improved cookstoves on lung function was reported in four studies.21 26 33 38 Decline in FEV1 across the study period was significantly smaller in women using an improved cookstove as compared with controls in one study: difference in FEV1 decline 31 mL/year (95% CI 7 to 55).33 In another study, the mean peak expiratory flow rate improved significantly among women in one out of two communities where improved cookstoves were introduced.21 Both studies assessing exhaled CO in women found significant reductions in those who had improved cookstoves.25 27 Two out of seven studies found significant reductions in personal CO exposure,36 38 and one out of three in cooking area CO levels.34 All three studies assessing cooking area PM2.5 levels found significant reductions in the improved stove group.21 31 34 Four out of five studies assessing changes in personal PM2.5 exposure found significant reductions in the intervention group.30–32 34 No studies assessing any of the other predefined secondary outcomes were identified.
Findings from longitudinal observational studies
Overall, findings from the longitudinal observational studies suggest that improved cookstoves are associated with reductions in adverse respiratory health outcomes: one study found significant reductions in paediatric pneumonia and severe pneumonia67; two of three studies that evaluated chronic respiratory diseases found statistically significant decreases among improved stove users57 61 64; three out of six studies found significant improvements in lung function51 64 65 and four out of six studies found significant decreases in self-reported respiratory symptoms.58 65–67 Additionally, these studies provide evidence that improved cookstoves reduce HAP levels: 12 out of 17 studies found that improved cookstoves were associated with significantly decreased kitchen levels of PM pollutants,46 47 49 53 54 59 62 63 69–71 73 and 13 out of 17 studies found significant decreases in indoor CO levels among improved cookstove users.45–47 49 50 54 59 60 63 69–71 73 Three out of five studies measuring PM levels,47 49 54 and 11 out of 12 studies measuring CO levels,46–50 54–56 68 71 73 found statistically significant reductions in personal exposure among improved cookstove users.
Discussion
Our systematic review provides mixed evidence regarding the impact of improved biomass cookstoves on health outcomes among women and children in LMICs. Few methodologically robust studies assessed our prespecified primary outcomes. Cookstove improvements had no demonstrable impact on child health outcomes in meta-analyses. No significant impact on adverse pregnancy outcomes was observed in individual studies, and no (quasi-)experimental studies assessing COPD among women were identified. In a prespecified sensitivity analysis, improved cookstoves were associated with a 26% reduction in the incidence of COPD among women. Meta-analyses of secondary outcomes among women further showed reductions in cough by 28%, phlegm by 35%, wheezing by 59% and conjunctivitis by 42%. Many studies showed that improved cookstoves significantly reduced indoor CO and PM2.5 levels and exposure, which likely mediated the observed health benefits.
To our knowledge, this is the first meta-analysis assessing the impact of improved biomass cookstoves on women’s and child health in LMICs.5 11 13 Using a highly comprehensive search strategy as part of a prespecified review protocol, we identified 53 studies relevant to our research question. In our interpretation, we focused primarily on evidence derived from studies using the most robust designs as advocated by the EPOC group.15 There was considerable variation between studies in which outcomes were evaluated and how these were defined, measured and how effect estimates were expressed. Also, several included reports originate from the same studies, in particular many reports described various findings from a large-scale RCT conducted in rural Guatemala (RESPIRE).25 29–31 36–39 These aspects eventually restricted the number of studies that could be combined in meta-analyses of individual outcomes, in particular of our predefined primary outcomes. For pragmatic reasons, we sometimes combined in meta-analyses outcomes which were slightly diverse but likely to assess the same concept (eg, conjunctivitis and sore eyes; wheezing and/or breathing difficulty). Conducting meta-analyses with few studies is methodologically sound74 75; however, the findings should be interpreted with care and additional studies are needed—with several already being underway—to increase confidence in the effect estimates. It should furthermore be noted that our prespecified primary outcomes were often not the primary outcomes of individual studies and hence these studies and the meta-analyses combining them may have had limited power to assess the actual impact of the intervention. Follow-up time was likely too short in some studies to effectively assess health impact, whereas studies with longer term follow-up sometimes noted that the health impact waned off, as use of the improved cookstoves was not sustained. Ineffective and unsustained use of improved cookstoves affected outcomes from a number of studies and may have biased the findings towards the null, although at the same time these may be argued to reflect—to some extent—the real-world situation. Given the low number of studies that could be combined in meta-analysis, we were unable to assess the relative effectiveness of the different cookstoves or cookstove improvements. Likewise, there were too few studies to allow for our predefined subgroup analyses by age group and cooking location to be conducted.
We are aware of two previous systematic reviews assessing the impact of improved biomass cookstoves on HAP indicators.13 14 Meta-analyses from one review indicated significant reductions in personal PM exposure and kitchen CO and PM concentrations, but were not performed for health outcomes.14 These HAP improvements are in line with our systematic review findings, where many studies reported positive findings in terms of HAP reduction. Similar to Thomas and colleagues,13 we experienced that variations in measurement location, expression of between-group differences and study set-up precluded pooling of HAP indicators in meta-analyses. We identified a greater number of eligible studies assessing the health impact of improved biomass cookstoves than previous reviews despite applying narrower study selection criteria,13 14 making meta-analysis of health indicators possible for the first time. This is important because, contrary to Quansah and colleagues who based on their qualitative review conclude that ‘current stand-alone household air pollution interventions yield little if any health benefit’,14 findings from our meta-analyses in fact suggest that improved biomass cookstoves provide significant symptom relief and potential health benefits among women. Importantly, no adverse effects were identified. Ongoing work is thus needed to locally develop, tailor, evaluate, implement and upscale effective cookstove improvement programmes in close collaboration with end-users. Experiences from earlier programmes across the globe have generated transferrable lessons in terms of which are the main facilitators and barriers to uptake of improved biomass cookstoves and these should be taken into account when designing local programmes.13 14 76 Likewise, a clear understanding of what enables or precludes sustained use of the improved stoves can help maximise long-term health benefits. Platforms such as the online HAP Intervention Tool enable policy-makers to estimate the potential health benefits of stove improvements locally, taking aspects such as acceptability and sustained use into account.77
Several knowledge gaps remain in understanding the health impact of improved cookstoves. Whereas many studies have evaluated their impact on HAP indicators, more work is needed to quantify the potential health benefits. In addition to evaluating health symptoms and short-term benefits, more studies should investigate long-term health impact. Significant reductions in COPD and lung cancer mortality among women were identified in studies in this review,57 61 64 indicating that the potential health gain may indeed be substantial. Also, more work is needed on evaluating whether improved biomass cookstoves may help reduce adverse pregnancy outcomes. Comparative studies are required to study which particular cookstoves or cookstove improvements (eg, stoves, more efficient combustion) are most effective, and more studies should take into account cost-effectiveness. It should furthermore be noted that no studies in urban areas were identified by our search. By 2030, an estimated five billion people will live in urban areas, of which two billion will live in slums in LMICs, mainly in Africa and Asia.78 Many differences exist between rural and urban settings, for example, regarding cooking location (eg, in the possibilities to cook outside) and background environmental air pollution. It is therefore essential that the existing knowledge gap of the potential health impact of improved cookstoves in urban—in particular slum—areas is filled in future research.79
From both the health and the environmental perspective, switching from using solid fuels for cooking to using cleaner fuels would be preferred over using improved cookstoves for solid biomass combustion.10 However, as pointed out earlier, financial and infrastructural constraints will likely hamper the transition to cleaner fuel options in the near future.1 10 Meanwhile, improved cookstoves can help temporarily and cost-effectively reduce some of the health risks associated with cooking using biomass.12 The consistent signal of symptom reduction and the potential health benefit observed among women in our meta-analyses suggest that future studies should move away from using control groups without intervention, at least in rural areas in LMICs. Rather, we suggest that outside the urban context, where randomised studies are still needed, implementation and upscaling studies including quasi-experimental evaluations may be a more appropriate approach to identify context-specific barriers and facilitators in developing culturally appropriate, locally relevant implementation while evaluating and expanding the associated health benefits to wider populations.
Conclusion
Improved biomass cookstoves had no demonstrable impact on child health but reduce airway symptoms and conjunctivitis, and potentially also COPD incidence, among women in LMICs. Considering that billions of people continue to rely on biomass combustion for cooking over the next decades, improved biomass cookstoves may help realise population health gains among women in LMICs pending the transition to using cleaner fuels.
Acknowledgments
We thank Gunther Bensch, Jason Burwen, Esperanza Diaz, Daniel Pope and Rufus Edwards for providing additional information about their studies. We thank Daan Nieboer for statistical support.
References
Footnotes
MT and PAWN contributed equally.
Contributors MT and PAWN performed electronic searches and study selection, extracted data and performed risk-of-bias assessment for (quasi-)experimental studies and wrote the first version of the manuscript. EAB and JFK extracted data and performed risk-of-bias assessment for longitudinal observational studies and assisted in updating electronic searches and study selection. TF checked the extracted data and performed meta-analyses. GRB co-wrote the manuscript. OCPvS and JVB supervised the various stages of the study and writing of the manuscript. All authors were involved in designing the study and interpreting the findings and have read and approved the final version of the manuscript.
Funding GRB is supported by an Intermediate Fellowship by the Wellcome Trust DBT India Alliance (Clinical and Public Health Research Fellowships). JVB is supported by fellowships from the Netherlands Lung Foundation (4.2.14.063JO) and the Erasmus MC.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Full data set and statistical codes are available from the corresponding author.
Linked Articles
- Airwaves