Article Text

Abstract
Background This study aimed to investigate whether adjunctive inspiratory muscle training (IMT) can enhance the well-established benefits of pulmonary rehabilitation (PR) in patients with COPD.
Methods 219 patients with COPD (FEV1: 42%±16% predicted) with inspiratory muscle weakness (PImax: 51±15 cm H2O) were randomised into an intervention group (IMT+PR; n=110) or a control group (Sham-IMT+PR; n=109) in this double-blind, multicentre randomised controlled trial between February 2012 and October 2016 (ClinicalTrials.gov NCT01397396). Improvement in 6 min walking distance (6MWD) was a priori defined as the primary outcome. Prespecified secondary outcomes included respiratory muscle function and endurance cycling time.
Findings No significant differences between the intervention group (n=89) and the control group (n=85) in improvements in 6MWD were observed (0.3 m, 95% CI −13 to 14, p=0.967). Patients who completed assessments in the intervention group achieved larger gains in inspiratory muscle strength (effect size: 1.07, p<0.001) and endurance (effect size: 0.79, p<0.001) than patients in the control group. 75 s additional improvement in endurance cycling time (95% CI 1 to 149, p=0.048) and significant reductions in Borg dyspnoea score at isotime during the cycling test (95% CI −1.5 to −0.01, p=0.049) were observed in the intervention group.
Interpretation Improvements in respiratory muscle function after adjunctive IMT did not translate into additional improvements in 6MWD (primary outcome). Additional gains in endurance time and reductions in symptoms of dyspnoea were observed during an endurance cycling test (secondary outcome)
Trial registration number NCT01397396; Results.
- pulmonary rehabilitation
- respiratory muscles
- exercise
Statistics from Altmetric.com
Key messages
What is the key question?
Can adjunctive inspiratory muscle training enhance the well-established benefits of pulmonary rehabilitation in selected COPD patients with inspiratory muscle weakness?
What is the bottom line?
Improvements in respiratory muscle function beyond those induced by general exercise training did not result in additional improvements in 6 min walking distance (primary outcome).
Why read on?
The observed between-group difference in endurance cycling time could serve as a basis for sample size calculations using endurance tests as primary outcomes in future studies of adjunct interventions.
Introduction
COPD is a major cause of chronic morbidity and mortality worldwide.1 Respiratory muscle dysfunction, which is frequently observed in patients with COPD,2 plays a key role in the perception of dyspnoea3 4 and contributes to exercise intolerance in these patients.5 6
Pulmonary rehabilitation (PR) is standard care for patients with COPD and results in statistically significant and clinically relevant improvements in exercise capacity and health-related quality of life.7 8 Inspiratory muscle training (IMT) has been extensively studied in the last decades in patients with COPD.9 However, due to differing interpretations of the existing evidence, in combination with limited resources and time constraints during PR programmes, this adjunctive therapy is at this moment not included in about 50% of these programmes.9–14 IMT as a stand-alone therapy improves inspiratory muscle function (strength and endurance), decreases symptoms of dyspnoea and improves exercise capacity.9 The value of adjunctive IMT during PR is less clear. While adjunctive IMT in combination with general exercise training (GET) resulted in significant additional improvements in respiratory muscle function beyond the effects of GET alone, its additional effects on outcomes such as exercise capacity and quality of life are insufficiently supported by data so far.7 9 Based on subgroup analyses in meta-analyses and general physiological considerations, it has been recommended that future studies of adjunctive IMT in patients with COPD should focus specifically on patients with exercise-induced dyspnoea and inspiratory muscle weakness.7 9 15
The present study examined the effects of adding a largely unsupervised, but well-controlled adjunctive IMT programme in the context of an adequately powered, multicentre, double-blind, randomised controlled trial (RCT) design, in selected COPD patients with inspiratory muscle weakness. We wanted to answer the question whether IMT can be a useful adjunctive therapy during PR for patients with COPD. We hypothesised that adjunctive IMT would result in additional improvements in functional exercise capacity (primary outcome) and inspiratory muscle function compared with rehabilitation alone.
Methods
This study was registered in an international trial registry database (ClinicalTrials.gov: NCT01397396). Clinically stable COPD patients with reduced maximal inspiratory mouth pressure (PImax <60 cm H2O or <50% of the predicted normal value) participated in the study between February 2012 and October 2016.9
More information about study procedures can be found in an extended ‘Materials and methods’ section and in a video tutorial (see online supplementary video files 1, 2, 3, and 4), as well as in a previously published study protocol.16
Interventions
Both groups performed an identical GET programme. The training volume ranged from 20 sessions (Germany) to 36 sessions (other centres). Training frequency ranged from 3 to 5 sessions per week. Duration of training sessions was around 60 min. Patients performed endurance training or interval training at moderate to high intensities. Training intensities during GET were progressively increased during the course of the programme based on symptom scores. Training intensities corresponded to Borg CR-10 scale ratings of 4–6 on dyspnoea sensation.16 Physiotherapists providing this intervention were blinded to group allocation of patients. All participants (intervention and control group) were led to believe that they followed an active adjunctive IMT intervention during the GET intervention. This was done in order to improve adherence with the intervention in the control group and to ensure placebo treatment effects in both groups.17 IMT in both groups was performed daily using the PowerBreathe KHP2 device (POWERbreatheKHP2, HaB International, Southam, UK) according to previously described methods.18 The training intensity (average external load (cm H2O)) and training quality (average mean power per breath and total work of breathing during one session of 30 breaths) were registered and stored during all training sessions. During weekly supervised sessions (7% of all training sessions), data on training quality during the unsupervised sessions were reviewed and patients received instructions and feedback on how to optimise their home training efforts. Training intensity in the intervention group was set initially at a load of approximately 50% of patients’ maximal inspiratory mouth pressure (PImax). This initial load was then continuously and gradually increased to the highest tolerable intensity during each of the supervised sessions.18 Training intensity in the control group was set at 10% baseline PImax and was not modified throughout the intervention period.
Outcome measurements
The primary outcome 6 min walking distance (6MWD) was assessed according to a standardised published protocol and related to reference values.19 Secondary outcomes included respiratory muscle function (strength and endurance), maximal and endurance cycling exercise capacity, pulmonary function, limb muscle forces and objectively measured physical activity (DynaPort Minimod, McRoberts, The Hague, The Netherlands). All outcome assessors were blinded to group allocation.
Sample size calculation
To detect a minimally clinically important difference (MCID) between groups of 26 m in the 6MWD,20 assuming an SD of the within-group differences in the 6MWD at the end of the intervention period of 60 m in both groups with a degree of certainty (statistical power) of 80% and a risk for a type I error (α)<5%, minimally 85 patients were calculated to be included in each group, given an anticipated dropout rate of 30%.
Statistical analysis
All data were analysed using a modified intention-to-treat approach (SPSS V.24 (IBM) and SAS V.9.4 (SAS Institute)). This means that we did not consider patients who had missing outcome data due to loss to follow-up in the analysis. Consequently, no imputation for missing data was performed and a so-called ‘complete/available case analysis’ was performed.21 The missing data were interpreted as ‘missing at random’. Differences between groups after the intervention were compared, adjusting for values of the respective outcomes at baseline, using analysis of covariance.22 Because randomisation was performed by centre, the adjustment by centre was tested. Additional exploratory analyses were performed to study (1) the impact of IMT characteristics on improvements in PImax and (2) the relationship between improvements in PImax and GET outcomes. More details on analyses by ‘centre’ and exploratory analyses are provided in the online data supplement. To account for the potential impact of differences in training volume between GET programme offered in the different centres on outcomes, we also tested the effect of ‘centre’ on treatment effects using centre*intervention effect. In post-hoc tests, we subsequently compared the effects in the centre offering 20 sessions GET intervention with the other centres offering 36 sessions.
Supplemental material
Results
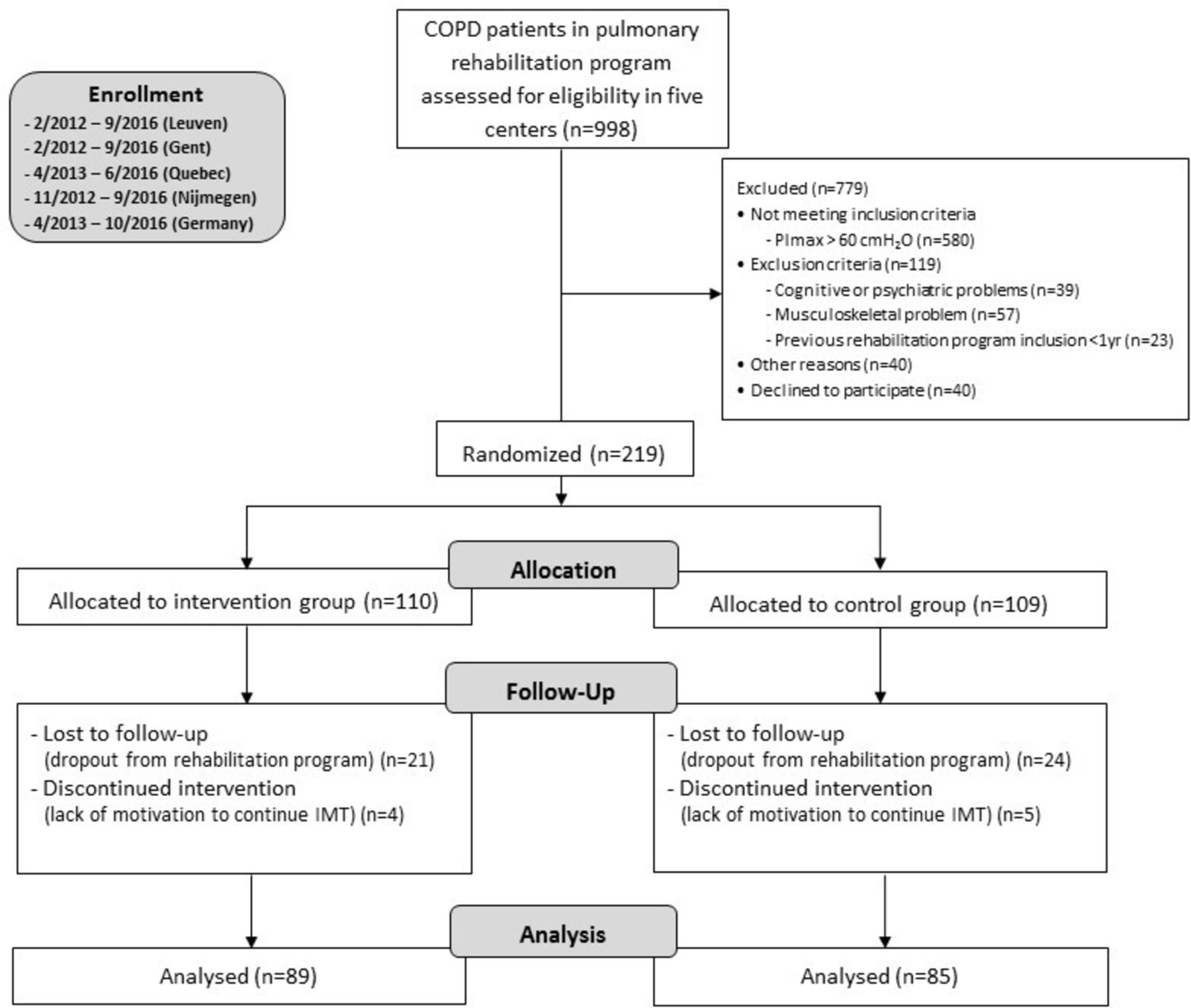
Between February 2012 and October 2016, 998 patients who entered the rehabilitation programme in the different centres were screened for study participation. A diagram summarising the flow of participants through the study is presented in figure 1. The most frequent reason for non-eligibility was not meeting the PImax inclusion criteria (73% of excluded subjects). At the end of the study, data were available for the primary outcome in 85% of subjects from the intervention group and 83% of participants in the control group. Baseline characteristics of included patients were not significantly different between the two groups (table 1). Comparisons between completers and patients who were lost to follow-up are summarised in the online supplementary table E1.

A diagram summarising the flow of participants through the study.
Baseline characteristics of patients
Changes in exercise capacity and GET progression
Results of different tests for exercise related outcomes are presented in table 2. No statistically significant between-group differences in improvements in 6MWD (primary outcome) were observed. Endurance cycling time (secondary outcome) improvement was significantly greater in the intervention group with significant reductions in dyspnoea symptoms at isotime during the test (table 2). Both cycling and treadmill training intensities during GET sessions were slightly higher in the intervention group without reaching statistical significance (p=0.212 and 0.657 for cycling and treadmill walking, respectively; see online supplementary figure E1).
Changes in exercise-related outcomes
IMT progression
The intervention group completed 79%±4% of prescribed IMT sessions while the control group completed 81%±4% of prescribed sessions. The intervention group increased their training load from 47%±2% of their baseline PImax in the first week of training to 84%±4% of their baseline PImax in week 12 (see online supplementary figure E2). Data on the weekly sum of total work performed during all IMT sessions (based on pressure and volume data recorded and stored by the training devices) are presented in figure 2. The average Borg CR-10 scale inspiratory effort scores for breathing during the final minute of the supervised IMT sessions were 3.5±0.3 and 2.6±0.3 for intervention and control group, respectively.

Progression of total work performed during the inspiratory muscle training programme in the intervention and control group. *P<0.05 between groups based on a two-way analysis of variance (ANOVA) analysis with Bonferroni corrections of post-hoc tests, values represented as mean ±SEM.
Changes in respiratory muscle function
Patients in the intervention group exhibited significantly larger improvements in inspiratory, but not expiratory muscle strength compared with the control group (table 3). During the endurance breathing test, the magnitude of improvement in time to the limit of tolerance, average mean power per breath and total work were also significantly larger in the intervention group (table 3).
Changes in respiratory muscle function
Changes in pulmonary function, quality of life and other secondary outcomes
The intervention group exhibited a significantly larger increase in FVC, both in comparison to baseline and to the control group (p<0.001 and p=0.028, respectively). There were no statistically significant changes in other pulmonary function variables between the two groups (online supplementary table E2). While both groups exhibited statistically significant and clinically relevant improvements within groups, there were no statistically significant differences between groups in all domains of the CRQ (online supplementary table E3). Quadriceps and handgrip strength were also both significantly improved within both groups after training with no statistically significant between-group differences. There was no statistically significant difference in the change in the number of steps per day within or between the two groups after the intervention.
Impact of centre on outcomes
Interactions between centres and between-group post-treatment differences in PImax (p=0.007), progression of training intensity during GET (p=0.200), endurance cycling time (p=0.007) and 6MWD (p=0.040) were observed. One of the centres offering a 36 session programme (32% of total inclusions) consistently exceeded between group differences in the centre offering 20 sessions (36% of total inclusions). In the other centres offering 36 sessions (combined 32% of total inclusions), between-group differences in these outcomes were consistently smaller than in the centre offering a lower training volume (see online supplementary table E4).
Correlates of improvements in inspiratory muscle strength
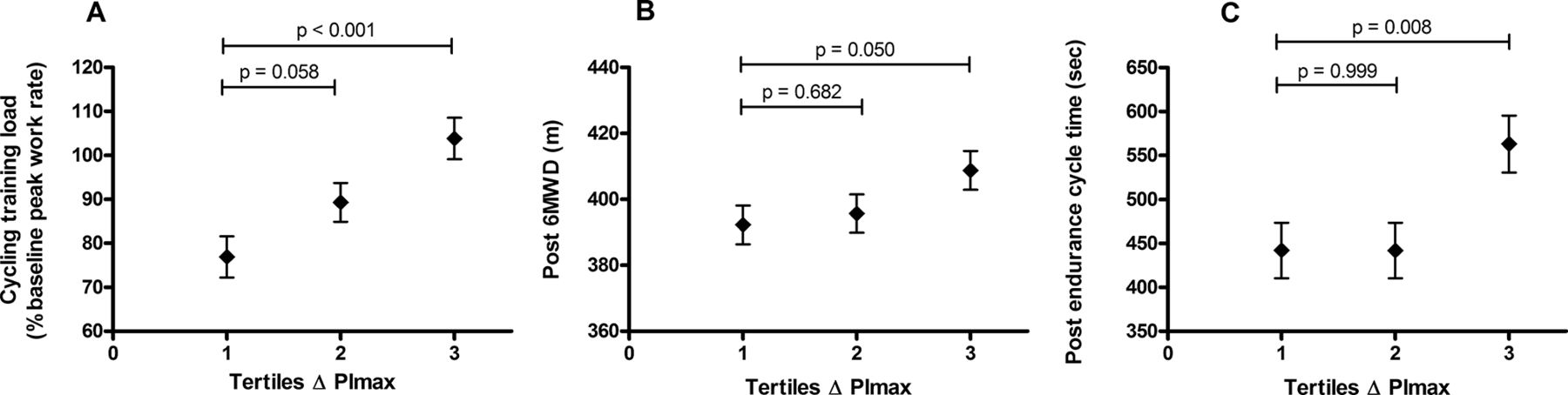
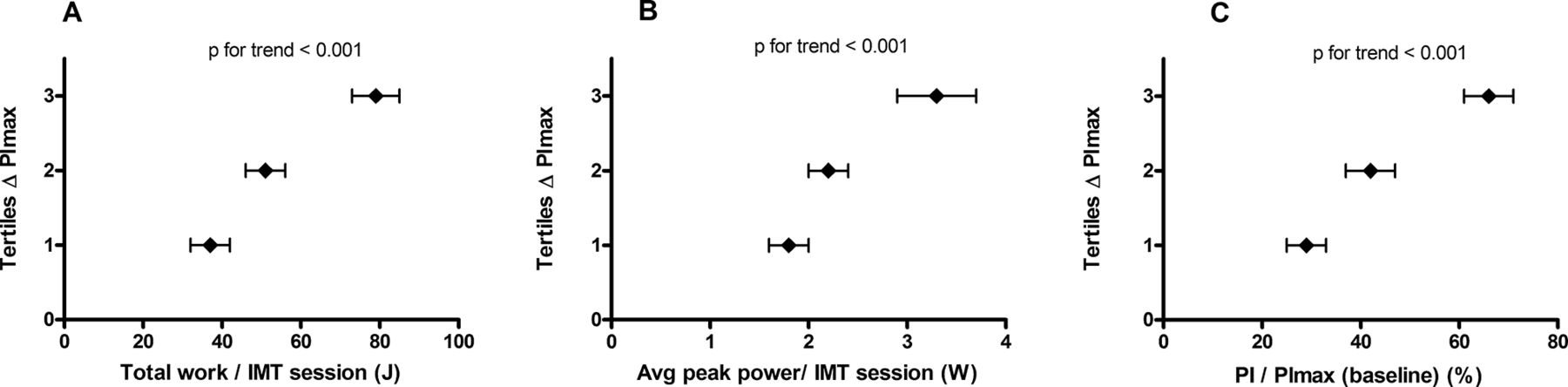
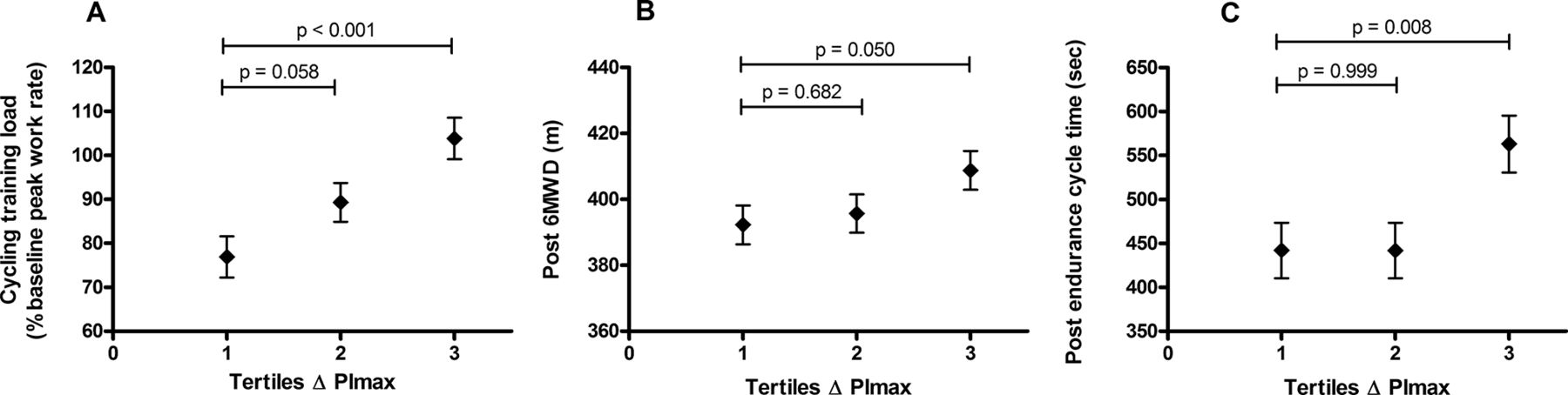
Both training quality indices registered during IMT sessions (ie, total inspiratory work performed per session and average peak power per session) and progression in training intensity were significantly related to the magnitude of improvements achieved in PImax (figure 3A–C). Conversely, average training volume (the number of sessions stored by the TFRL devices) was not significantly associated with changes in PImax (p-for-trend=0.129). In a stepwise multiple regression analyses, total work performed during IMT sessions (partial r2: 0.24), baseline PImax (partial r2: 0.08) and training compliance (partial r2: 0.01) were significantly related to the improvements in PImax after training (F(3, 139)=22.9, p<0.001, R2=0.33). More detailed results of the regression analyses are provided in online supplementary table E5. Subsequently, improvements in PImax were related to the progression in cycling training intensity during the GET programme, as well as to increases in 6MWD and endurance cycling time after the training period (figure 4A–C).

Relationships of training quality indices (total work performed per inspiratory muscle training (IMT) session, average peak power per IMT session; (A, B), and training intensity (defined as inspiratory load (PI) during the final IMT sessions expressed as % of baseline PImax; C), with improvements in PImax. Tertiles based on improvements in PImax were defined as follows: 1st tertile: ∆PImax ≤7 cm H2O (n=56; 29% intervention group and 71% control group), 2nd tertile ∆PImax 8–20 cm H2O (n=60; 48% intervention group and 52% control group), 3rd tertile: ∆PImax ≥21 cm H2O (n=55; 78% intervention group and 22% control group). Data are presented as mean ±SEM.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationships between improvements in PImax and cycling training load during the last week of general exercise training (A), 6 min walking distance (6MWD) (B) and endurance cycling time after training (C). Tertiles based on improvements in PImax were defined as follows: 1st tertile: ∆PImax ≤7 cm H2O (n=56; 29% intervention group and 71% control group), 2nd tertile ∆PImax 8–20 cm H2O (n=60; 48% intervention group and 52% control group), 3rd tertile: ∆PImax ≥21 cm H2O (n=55; 78% intervention group and 22% control group). Data are presented as mean ±SEM.
Discussion
This study is the first adequately powered RCT that investigated the effects of adjunctive IMT on outcomes beyond respiratory muscle function in patients with COPD who had been selected based on the presence of inspiratory muscle weakness. There was no statistically significant difference between groups for improvements in 6MWD (primary outcome). Patients in the intervention group however achieved larger gains in respiratory muscle function and also endurance exercise capacity (prespecified secondary outcome) increased significantly more in the intervention group. Significant reductions in dyspnoea symptoms at isotime during the cycling test were also observed in favour of the intervention group.
Contrary to our initial hypothesis, larger gains in respiratory muscle function in the intervention group did not translate into further improvements in 6MWD compared with the control group. Changes in the intervention group and the control group were both equally large and fall within the range of a MCID of 25–35 m.23 These findings are in line with results from a recent systematic review of RCT’s studying adjunctive interventions during PR. In this meta-analysis, none of the studied adjunctive interventions (eg, leg muscle strength training, IMT, non-invasive ventilation or nutritional supplementation) were able to induce statistically significant additional improvements in 6MWD.24 In contrast to the results of the 6MWD, significantly larger improvements in cycling endurance time and significantly greater reductions in dyspnoea symptoms at isotime were observed in the intervention group in the current study. The average additional improvement in endurance cycling time of 75 s falls within a range of 46–105 s that has recently been defined as an MCID for constant-load cycle endurance time improvements in response to pharmacological interventions.25 The superior responsiveness of endurance exercise tests compared with the 6MWD test is in line with several other recent reports comparing responses in these outcome measures after both pharmacological and non-pharmacological interventions in patients with COPD.26–28 These differences are probably related to the different characteristics of physiological responses elicited by the two tests.26 29 In hindsight we believe that our expected between-group difference in 6MWD of 26 m did not represent a realistic magnitude of between-group differences in 6MWD in studies of adjunct interventions to PR. Our data rather indicate that a more sensitive outcome (ie, endurance walking or cycling test) might be more useful as a primary outcome. In the absence of a clinically meaningful difference for adjunct interventions, the magnitude of our observed between-group differences both in endurance cycling time and symptoms at isotime could serve as a basis for sample size calculations using endurance tests as primary outcomes in future studies of adjunct interventions. It is unlikely that the type of analysis (intention to treat based on ‘complete/available case analysis’) had a major impact on the results since the ‘completers’ of the study did not differ significantly from ‘non-completers’ with regard to baseline characteristics that were identified as confounding variables (see online supplementary tables E1 and E6).
In the current study, we found 23 cm H2O or 42% improvement of PImax in the intervention group compared with 9 cm H2O or 17% in the control group. In a recent meta-analysis, the improvements were 18 cm H2O (29%) in the intervention group and only 5 cm H2O (8%) in the control group.9 This resulted in PImax effect sizes of 1.07 in the current study compared with 0.73 in the meta-analysis. The larger improvements in the control group (17% in our study vs 8% in the meta-analysis) might be explained by the fact that not all control groups in the meta-analysis performed a sham training intervention. Moreover in the current study, all patients (intervention and control group) were maximally familiarised with the PImax measurements which were performed every week during the intervention period. The larger improvements in our intervention group in comparison to previous studies (42% vs 29%) might be related to the well-controlled nature of the IMT programme (despite the fact that it was not performed fully supervised).18 The magnitude of improvements in PImax is comparable to previous studies involving this IMT protocol in patients with COPD.18 30 The large effect size in endurance breathing time of 0.79 was somewhat smaller compared with the results of the meta-analysis (effect size: 1.05).9 This might again be partly explained by the fact that all patients in our study (in contrast to the studies included in the meta-analysis) participated in a sham control training. This sham intervention (ie, performing full vital capacity inspirations while generating high inspiratory flow rates) might even have constituted an endurance-type training stimulus for these patients in addition to the endurance-type training stimulus provided by the GET sessions itself.
Beyond additional improvements in exercise capacity and symptoms during the endurance cycling test and respiratory muscle function, we did not observe any further improvements in quality-of-life domains (including dyspnoea subscales). It might be that the substantial improvements in quality-of-life scores in the control group in response to the comprehensive rehabilitation intervention were already approaching the ceiling effect for improvement. In analogy with the absence of additional improvements in the 6MWD, this might be related to a limited sensitivity of the applied questionnaire (CRQ) to pick up additional improvements on top of an already very significant and clinically important effect. This might be improved in future studies by using other potentially more sensitive dyspnoea scales. One option would be to use scales that are specifically designed to detect different gradations of change like the transitional dyspnoea index.31 Another excellent emerging option is the multidimensional dyspnoea profile which can be specifically focused to assess symptoms during predefined periods (eg, at standardised times during an exercise test).32
With regard to improvements in daily physical activity, we observed similar improvements in both groups. We know that physical activity is a complex behaviour that is determined by multiple factors. A systematic review demonstrated that large improvements in exercise capacity and symptoms after rehabilitation interventions only result in relatively modest increases in physical activity compared with control groups in patients with COPD.33 We therefore believe that it would be unrealistic to expect that the relatively small additional improvements in endurance exercise capacity and dyspnoea symptoms after adjunctive IMT (compared with effects of PR vs control groups) would easily translate into greater participation in daily physical activity.
Correlates of improvements in respiratory muscle function and impact of ‘centre’ on outcomes
A significant relationship was observed between the improvements in PImax and both training quality during IMT (ie, total inspiratory work performed/session, average peak power/session) as well as progression of training intensity. Our results emphasise that external work and power are important training quality parameters of the training stimulus that is delivered to the inspiratory muscles. Training volume or compliance (number of completed training sessions) was not significantly related with the magnitude of changes in PImax. Interestingly, we found in a multiple regression model that from all training variables the total work performed (reflecting pressure and volume responses during individual sessions in combination with the number of training sessions) was the strongest predictor of improvements in PImax (see online supplementary table E5). This underlines that monitoring the quality of the training (total work performed) during IMT is of utmost importance to ensure meaningful training adaptations in response to the intervention.
One participating centre that contributed to 36% of all inclusions offered a 20-session GET programme while all other centres offered a 36-session programme. A priori, we had hypothesised that adjunctive effects in the centre offering fewer training sessions would be smaller. We concluded this since we expected that it would take some weeks before the reductions in exertional dyspnoea induced by IMT would result in higher training intensities during bicycle and treadmill endurance exercises that to be tolerated by the participants of the PR programme. Unexpectedly, compared with the centre that offered 20 sessions, those offering more sessions achieved both consistently larger and consistently smaller between-group differences in several relevant outcomes (ie, increases in PImax, bicycle exercise intensity during PR sessions, 6MWD and endurance cycling time; see online supplementary table E4) compared with the centre that offered 20 sessions. The uniformity of these data (ie, differences in these variables were either consistently larger or smaller) is in line with the presented relationships between improvements achieved in PImax, on the one hand, and the ability to increase exercise intensity during GET and resulting improvements in exercise capacity, on the other hand (figure 4). From these observations, we conclude that factors other than the number of sessions offered (such as contrasts in symptom-based training intensity during GET sessions between groups) probably contributed to the interaction between centre and training outcomes.
Strengths and limitations
One of the major advantages of the IMT intervention compared with previous trials was the ability to record and store training parameters with the training device. The information of recorded data from IMT sessions performed in the home setting was used to provide patients with feedback on their performance during supervised sessions. It also allowed us to reduce the total volume of supervised sessions to only 7% of all training sessions, thereby reducing burden on healthcare providers offering the intervention. Both groups had a high and similar IMT training compliance (training volume). Good compliance in the control group was probably partly related to the fact that all patients were led to believe that they were participating in an active intervention. Fifty-five per cent of patients in the intervention group met the target training intensity (inspiratory load of ≥50% PImax) already from the second week of training and increased their training intensity to an average of 84% of their baseline PImax by the end of the IMT intervention (see online supplementary figure E2). Moreover, patients in the intervention group performed the IMT sessions at this high training intensity while reporting only moderate (3.5±0.3) perceived inspiratory effort scores. The relatively low effort scores at high training intensities might be related to the loading characteristics of the device, providing an adequate volume reward with every inspiratory effort. These factors taken together probably contributed to the good compliance with the training protocol in the intervention group and are in line with a previous study using a similar training protocol.18 The proportion of patients who discontinued the intervention due to lack of motivation was similarly small in both groups (4% and 5% in intervention and control group, respectively). Collectively these observations support the clinical feasibility of implementing this controlled, high-intensity adjunctive IMT protocol during a rehabilitation programme in these patients.
Another strength of the study was that the physiotherapists or exercise specialists who supervised the GET were blinded to group allocation. Training intensity during GET was gradually increased during the course of the programme based on highest tolerable dyspnea symptoms assessed with Borg CR-10 symptom scales.34 The fact that we observed slightly higher (though not significantly different) training intensities especially on the bicycle in the intervention group is another indirect indication that participation in the IMT intervention probably impacted on activity-related symptoms. Another strength of the study is that patient selection, study design, training methods and selected outcomes in the present study followed recent recommendations for this type of intervention.7 9 15 24 A limitation of this approach is that the results are only applicable to a selective group of patients with COPD who have inspiratory muscle weakness. This is a minority of patients since only 22% of all patients with COPD met the criteria to participate in the study. This limits the external validity of our findings to this specific subgroup of patients.
This was also the main reason that the recruitment period had to be extended from 2 to 4 years. Given the absence of any contrast between groups on the primary outcome, we do not believe that the study was underpowered for the primary outcome and that a larger sample might have been necessary to detect an effect on 6MWD. We rather believe that different outcomes (ie, endurance cycling or walking test) should be chosen as a primary outcome for future trials of adjunctive interventions during PR.28 We do also not believe that a non-inferiority trial would be valuable in this specific setting given the initial hypothesis of the study. Our main research question was whether adjunctive treatments can enhance the effectiveness of PR in selected patients for functional outcomes. The effectiveness of our ‘control intervention’ (PR) on 6MWD and quality of life has already repeatedly been demonstrated.8
Clinical relevance for an individual patient will eventually depend on how the achieved benefits are valued compared with both the efforts that had to be invested and the potential discomfort associated with the intervention. Another limitation of the study is that satisfaction of patients with the adjunctive intervention was not directly assessed. Finally, we did not perform serial IC measurements during exercise. This would have made it possible to evaluate whether (1) these severely hyperinflated patients did dynamically hyperinflate during exercise breathing and whether this might be a patient characteristic influencing the intervention effect and (2) whether the combined intervention was able to modify breathing pattern and the degree of dynamic hyperinflation during exercise hyperpnoea. These measurements could be performed in future studies and might facilitate identification of patients who are more or less likely to respond to the adjunct intervention.
Clinical implications and general conclusion
The results of this study do not support the addition of IMT to PR to further enhance the 6MWD. At the same time we believe that the improvements in our secondary outcome (constant workrate endurance cycling) were not negligible (50% greater than rehabilitation alone). We believe that this is an important finding that could guide researchers towards identifying more appropriate primary outcomes for future studies of adjunctive interventions to PR. The multidimensional dyspnoea profile32 might be be an interesting option to assess differences in symptoms at standardised times during an exercise test. The overall good training compliance indicates that it was feasible to implement this adjunctive IMT intervention on a relatively large scale. Across the different centres it was furthermore feasible to implement simple and sensitive clinical assessments of respiratory muscle function (both strength and endurance). The study also highlights the benefits of closely monitoring and controlling IMT sessions since both quality and intensity of training sessions were strongly associated with improvements in respiratory muscle function. Additionally, improvements in PImax were related to the progression in cycling training intensity during the GET programme, as well as to increases in 6MWD and endurance cycling time after the training period.
We also believe that (in addition to using endurance exercise tests as primary outcomes) patient satisfaction with adjunctive interventions should be included as an additional important outcome in similar studies in the future.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Acknowledgments
The authors acknowledge HaB International (Southam, UK) and McRoberts (The Hague, The Netherlands) for providing the equipment for the testing and training in this study. On behalf of IMTCO investigators, the authors would like to acknowledge the physiotherapists from all centres for performing the pulmonary rehabilitation programme, and all measurements of included patients as blinded outcome assessors.
References
Footnotes
Contributors RG, DL and NC had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. DL, NC, RG, MD and AM contributed substantially to the study design. DL, NC, HD, FM, DS, SV, HvH, LG, TS and RG provided data collection. DL, RG, NC and HD contributed to the data analysis and interpretation. DL, RG and NC drafted the report, and all authors then critically reviewed it for important intellectual content.
Funding DL and HD are postdoctoral fellows of Research Foundation Flanders. HaB International (Southam, UK) and McRoberts (The Hague, The Netherlands) provided equipment for testing and training in this study on loan. This study was further supported by local funds throughout the participating centres. The following specific funding sources were reported: University Hospital Leuven, Belgium (FWO grant GOA4516N en KU Leuven grant C22/15/035); Ghent University Hospital, Belgium (UZ Gent grant FS/LGZ/994); Institut Universitaire de Cardiologie et de Pneumologie de Québec, Université Laval, Quebec, Canada (Ordre professionnel de la physiothérapie du Québec).
Disclaimer None of the sponsors had any role in the preparation of the trial design, patient recruitment, data collection, data analysis, interpretation of the data, approval of the report or the decision to submit this manuscript for publication.
Competing interests AM acknowledges a previous (now expired) beneficial interest in the POWERbreathe inspiratory muscle trainers in the form of a share of royalty income to the University of Birmingham, and a potential share of royalty income to Brunel University. In the past, she has also provided consultancy services to POWERbreathe International, but no longer does so. She is named on two patents relating to POWERbreathe products, including the device used in the present study, as well as being the author of two books on inspiratory muscle training. FM reports research support from Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, Grifols and Novartis, advisory board participation for Boehringer Ingelheim and GlaxoSmithKline, and speaking engagements for Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, Grifols and Novartis.
Patient consent Obtained.
Ethics approval University Hospital Leuven Institutional Review Board (approval number ML7489).
Provenance and peer review Not commissioned; externally peer reviewed.