Article Text

Abstract
Background Physical recovery following critical illness is slow, often incomplete and is resistant to rehabilitation interventions. We aimed to explore the contribution of persisting inflammation to recovery, and investigated the potential role of human cytomegalovirus (HCMV) infection in its pathogenesis.
Methods In an a priori nested inflammatory biomarker study in a post-intensive care unit (ICU) rehabilitation trial (RECOVER; ISRCTN09412438), surviving adult ICU patients ventilated >48 h were enrolled at ICU discharge and blood sampled at ICU discharge (n=184) and 3 month follow-up (N=123). C-reactive protein (CRP), human neutrophil elastase (HNE), interleukin (IL)-1β, IL-6, IL-8, transforming growth factor β1 (TGFβ1) and secretory leucocyte protease inhibitor (SLPI) were measured. HCMV IgG status was determined (previous exposure), and DNA PCR measured among seropositive patients (lytic infection). Physical outcome measures including the Rivermead Mobility Index (RMI) were measured at 3 months.
Results Many patients had persisting inflammation at 3 months (CRP >3 mg/L in 59%; >10 mg/L in 28%), with proinflammatory phenotype (elevated HNE, IL-6, IL-8, SLPI; low TGFβ1). Poorer mobility (RMI) was associated with higher CRP (β=0.13; p<0.01) and HNE (β=0.32; p=0.03), even after adjustment for severity of acute illness and pre-existing co-morbidity (CRP β=0.14; p<0.01; HNE β=0.30; p=0.04). Patients seropositive for HCMV at ICU discharge (63%) had a more proinflammatory phenotype at 3 months than seronegative patients, despite undetectable HMCV by PCR testing.
Conclusions Inflammation is prevalent after critical illness and is associated with poor physical recovery during the first 3 months post-ICU discharge. Previous HCMV exposure is associated with a proinflammatory phenotype despite the absence of detectable systemic viraemia.
Trial registration number ISRCTN09412438, post results.
- Innate Immunity
- Exercise
- Assisted Ventilation
Statistics from Altmetric.com
Key messages
What is the key question?
Is systemic inflammation prevalent during recovery from critical illness and is it associated with physical recovery?
What is the bottom line?
Systemic inflammation is highly prevalent during recovery from critical illness and is independently associated with physical recovery.
Why read on?
We present inflammatory persistence as a plausible mechanism for poor physical function after critical illness and intriguing data that raise the possibility that human cytomegalovirus infection may contribute.
Introduction
Survivors of critical illness suffer physical weakness and functional impairment that can be severe and long-lasting.1 ,2 Understanding of the pathophysiological processes that result in neuromuscular dysfunction during critical illness is improving,3 ,4 but there is little evidence that interventions delivered after injury has occurred can improve physical outcomes.5 A systematic review of exercise-based rehabilitation trials initiated after intensive care unit (ICU) discharge,6 and our recently published rehabilitation trial (RECOVER)7 suggest no effect on physical recovery when the intervention is started during the post-ICU period. Reasons for this lack of response are uncertain, but could include an established neuromuscular deficit or persisting pathophysiological processes blocking muscle recovery. The inflammatory nature of most critical illness raises the possibility that persisting inflammation could directly interfere with neuromuscular regeneration.
Damage to the neuromuscular unit occurs early during an episode of critical illness; identified risk factors include sepsis, inflammation, multiple organ failure and hyperglycaemia.8 Multiple studies have observed associations between inflammatory markers and muscle function in chronic inflammatory diseases,9–12 making it a plausible risk factor for poor physical recovery after critical illness. The prevalence of persisting inflammation and its association with recovery have not been described in unselected critical care cohorts.13
The factors that modulate persistence and resolution of inflammation after critical illness have also not been studied. A possible mechanism of persistence is viral reactivation, particularly of human cytomegalovirus (HCMV), which frequently reactivates during ICU admission in previously exposed individuals and is associated with poorer ICU outcomes and higher mortality.14–19 HCMV infection (both latent and lytic) can modify the innate immune response,20 ,21 providing a biologically plausible mechanism for persisting inflammation.
In the RECOVER trial, we included, a priori, a nested study of inflammatory mediators in patients agreeing to regular blood sampling between enrolment (ICU discharge) and the primary outcome assessment (3 months postrandomisation).22 As the trial showed no effects on clinical outcomes, these data were suited to a cohort study design using both clinical and inflammatory mediator data as exposures, and the measures of physical function at 3-month follow-up as outcomes. We hypothesised that systemic inflammation is prevalent in ICU survivors following ICU discharge, and that the presence of persisting systemic inflammation is associated with poorer physical recovery. As an additional mechanistic analysis, we explored whether HCMV infection was associated with systemic inflammation and physical recovery.
Methods
RECOVER was a randomised trial of increased hospital-based physical rehabilitation and information provision for ICU survivors. The protocol, description of the intervention and trial results have been published.7 ,22 ,23 Participants were recruited from two ICUs in Edinburgh, Scotland from 1 December 2010, through 31 January 2013. Inclusion criteria were: receipt of >48 h of continuous mechanical ventilation and deemed fit for ICU discharge. Exclusion criteria included a primary neurological diagnosis, receipt of palliative care, receipt of home ventilation, considered unable to provide informed consent, follow-up not feasible, discharge to a non-study hospital, aged <18 years and enrolment in another randomised controlled trial (RCT) with similar end points.
Both groups received existing ward-based physiotherapy, dietetics, occupational and speech/language therapy until hospital discharge. The intervention patients received enhanced hospital-based physical rehabilitation and information provision that increased the frequency and intensity of multiple aspects of rehabilitation between enrolment and hospital discharge.
RECOVER was approved by the Scotland A Research Ethics Committee (10/MRE0018). Patients provided specific consent for inclusion in the blood sampling substudy during consent for the main study. The between-group comparison of outcomes in the trial found no clinically or statistically significant differences in measures of physical function, health-related quality of life (HRQoL), psychological morbidity or self-reported symptoms.7
Sampling
Blood was sampled at the time of randomisation (ICU discharge), and 3 months after ICU discharge by venepuncture or from an arterial line if present. Blood was stored at room temperature for 30 min and then centrifuged at 2500 g for 10 min. Serum and plasma were stored at −70°C prior to assay.
Physical outcome
Physical assessments included the Rivermead Mobility Index (RMI) (a validated measure of physical mobility ranging from 1 (unable to turn over in bed) to 15 (able to run)),24 handgrip strength (HGS; a measure of forearm muscle strength in kg)),25 the timed up and go test (TUG; a measure of lower limb strength and balance)26 and the physical component of the Medical Outcomes Study Short Form 12 version 2 (PCS); a validated measure of HRQoL.27
Biomarkers
To detect ongoing inflammation we measured C-reactive protein (CRP) concentration. To further characterise inflammatory phenotype, we measured cytokines active during the initiation (interleukin 1β (IL-1β), IL-6), propagation (IL-8) and resolution (transforming growth factor β1 (TGFβ1) and secretory leucocyte protease inhibitor (SLPI)) of inflammation. In addition, we measured human neutrophil elastase (HNE), a marker of ongoing neutrophil degranulation or non-apoptotic neutrophil death, to assess persisting neutrophil activation. The biomarkers measured were prespecified in an analysis plan submitted to the trial statistician (SL) prior to trial data being made available.
Inflammatory biomarkers were assayed by ELISA. All assays were carried out in duplicate. Coefficients of variation (CVs) were calculated for each duplicate pair. Where CVs were >15% pipetting error was assumed, and assays were repeated.
Human cytomegalovirus
To establish prior exposure to HCMV, a quantitative indirect antiglobulin enzyme immunoassay (VIDAS CMV G, bioMérieux, Lyon, France) was used. HCMV IgG antibody was quantified in arbitrary units per millilitre (aU/mL). As per the manufacturers instructions, patients with serum concentration of >6aU/mL were considered to have positive serology (evidence of previous exposure). In patients with evidence of previous exposure, quantitative HCMV PCR was carried out to establish the presence of active lytic infection (detectable HCMV DNA). The lower detection limit of this assay was 160 IU/mL.
Analysis
All analyses were carried out using IBM SPSS Statistics V.21. p<0.05 was defined as statistically significant.
Prevalence of systemic inflammation
Inflammation prevalence was estimated with reference to CRP measurements in healthy adults. The percentage of surviving patients at each time point that had a serum CRP concentration of >3 and 10 mg/L representing the 90th and 99th centiles, respectively, was calculated.28
Inflammatory profile
For patients with complete paired data, biomarker concentration was reported at baseline and 3 months after ICU discharge. The median change in biomarker concentration between the two time points was calculated and assessed using Wilcoxon signed rank tests. To place data in a clinical context, upper reference limits for biomarkers were derived from published studies of healthy cohorts, and proportions of patients exceeding these limits calculated.
Relationship with physical recovery
The relationship between RMI and each of the inflammatory biomarkers was tested using univariable linear regression. This analysis was repeated for HGS, TUG and PCS.
To control for the effects of confounding, multivariable linear models were constructed to account for relevant pre-existing patient characteristics (age, gender and functional co-morbidity (as measured by the functional co-morbidity index (FCI)), and acute illness severity (APACHE 2 score and days of mechanical ventilation during ICU stay). The FCI is a validated 18-point measure capturing coexisting co-morbidity and concurrent disease, which is strongly associated with self-reported physical HRQoL.29
Due to violation of linear regression model assumptions (non-normal distribution of predicted values of the outcome variable around the regression line) RMI, which was negatively skewed, required inverse natural log transformation (16-ln(RMI)) prior to regression analysis. Inflammatory biomarkers, ventilator days and TUG were positively skewed and required natural log transformation prior to regression analysis. For zero value biomarker concentrations, 0.001 was added to allow transformation.
Role of cytomegalovirus in post-ICU inflammation and recovery
The percentage of patients with prior exposure to HCMV (HCMV IgG positive) and the proportion of these with lytic infection (detectable HCMV PCR) were reported at ICU discharge and at 3 months. The concentration of each inflammatory biomarker was compared between patients previously exposed to HCMV and those not previously exposed. To explore the potential for HCMV to affect physical function, physical outcomes were compared between these groups using an independent samples median test. In addition, to test whether HCMV seropositivity confounds the association between inflammation (as measured by CRP and RMI) tested in the previous section, we added HCMV seropositivity as an additional variable in the multivariable linear regression model. Our analysis plan aimed to assess the relationship between ongoing lytic infection and measures of recovery, but the low number of patients with lytic infection meant meaningful comparisons could not made.
Missing data
The primary analysis was a complete case analysis. To ensure that the results of this analysis were not subject to bias introduced by assuming the missing patients were similar to those included, a sensitivity analysis was carried out imputing data according to two different assumptions (see online supplementary data).30 ,31
Supplemental material
Results
Patients
Two hundred and forty patients were recruited to the RECOVER study; of these, 193 (80%) consented to blood sampling (figure 1). Baseline characteristics of the included patients are shown in table 1.
Patient characteristics presented for all consenting patients (n=193), and for patients grouped according to CRP tertile at 3 months after ICU discharge (n=123)
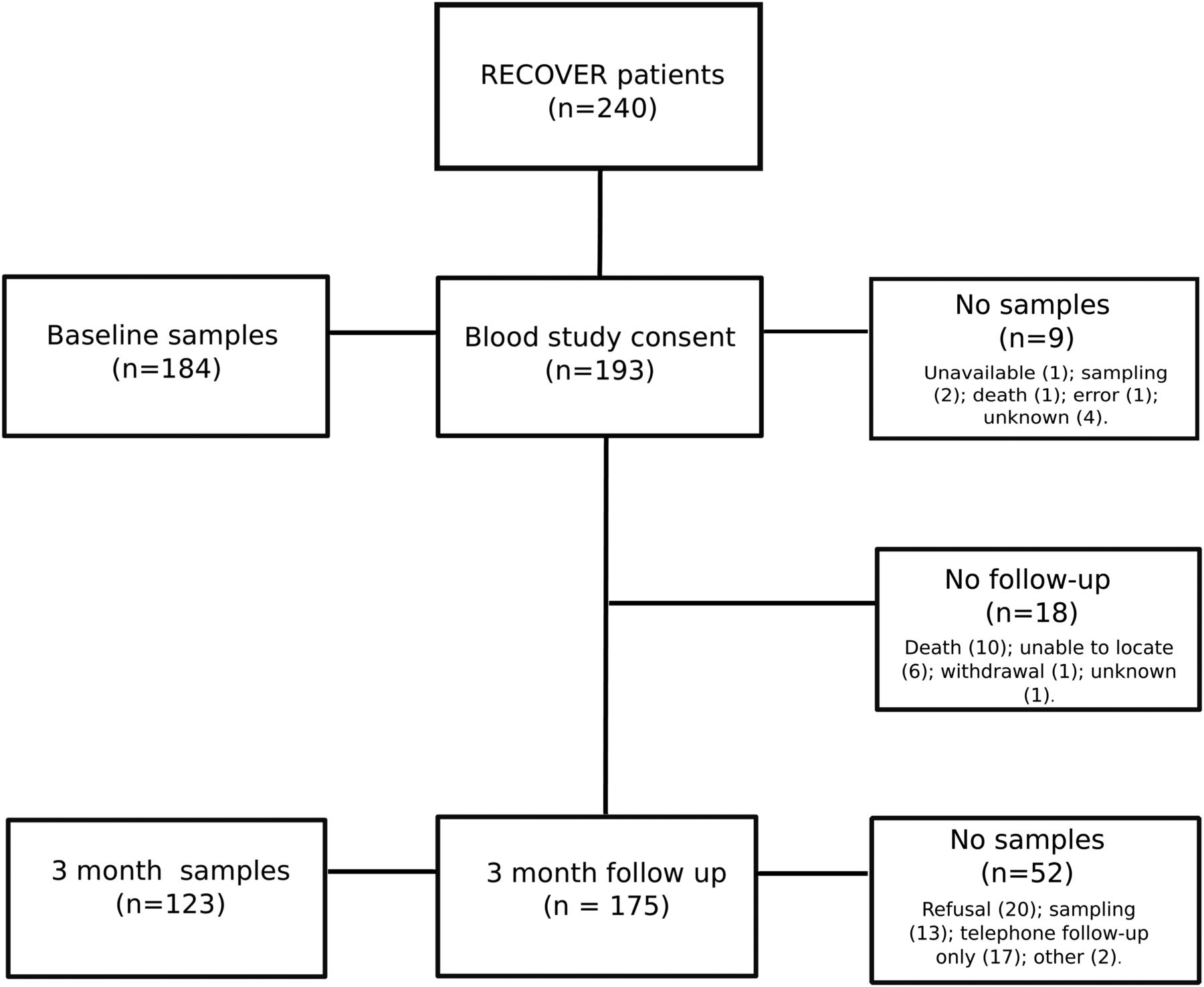
Study flow diagram.
Physical outcomes
The 3-month outcome data showing central tendency and dispersion are presented in table 2.
Physical outcome at 3 months
Prevalence of systemic inflammation
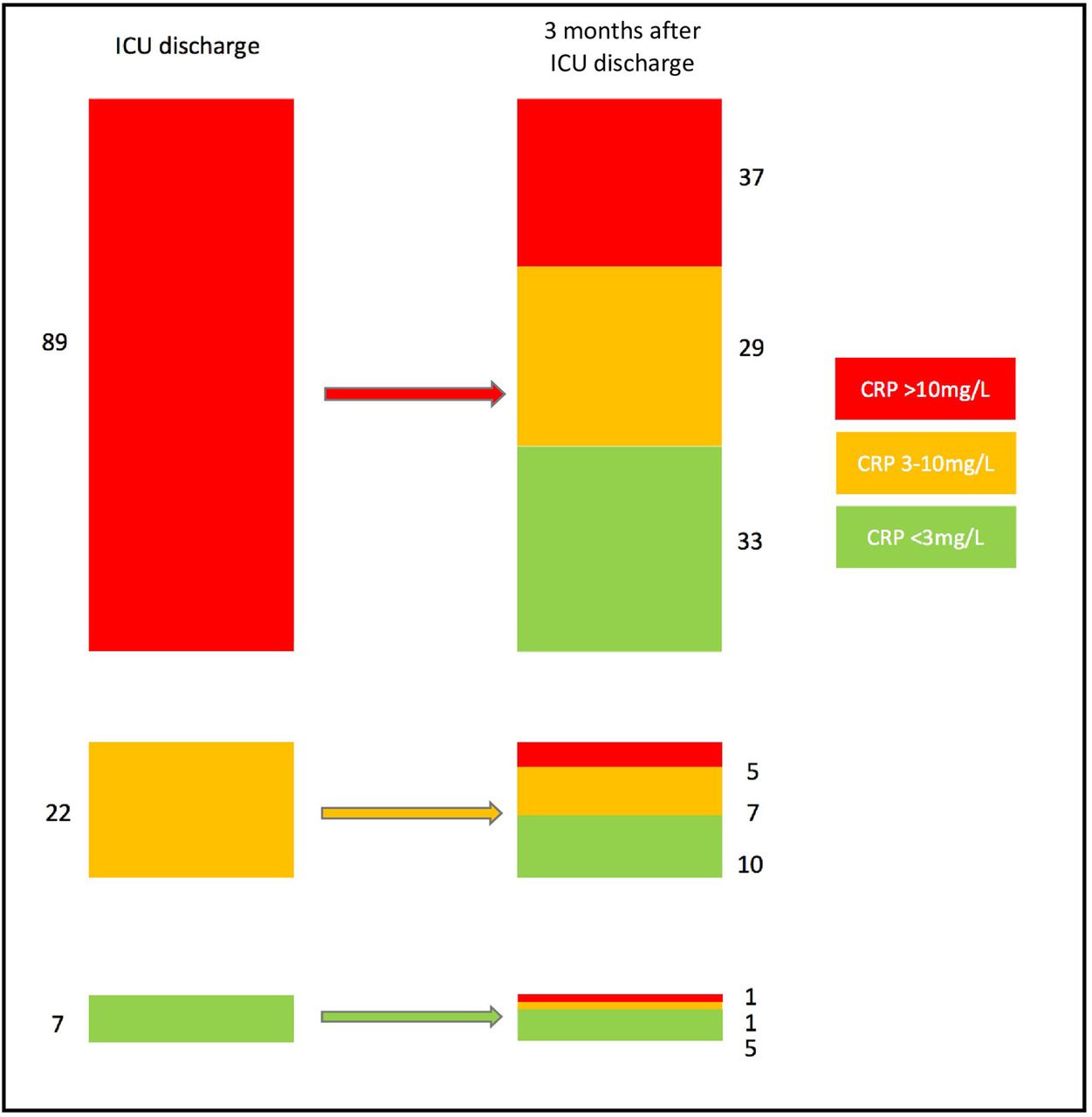
At ICU discharge, 141/184 (77% (95% CI 70% to 82%)) of patients had a CRP concentration of >10 mg/L and 173/184 (94% (95% CI 90% to 97%)) had a CRP concentration of >3 mg/L. Three months after ICU discharge, 34/123 (28% (95% CI 21% to 36%)) of patients had a CRP concentration of >10 mg/L and 72/123 (59% (95% CI 50% to 67%)) of patients had a CRP concentration >3 mg/L. For complete cases (n=118) CRP concentration fell from 27.9 mg/L (10.4–63.1) at baseline to 4.4 mg/L (1.2–12.0) at 3 months with a median change of −20.7 mg/L (95% CI −26.9 to −14.5; p<0.01). For this same complete case cohort (n=118), figure 2 describes the inflammatory outcome of patients with CRP concentrations that had high (>10 mg/L), medium (3–10 mg/L) and low (<3 mg/L) CRP concentration at ICU discharge.
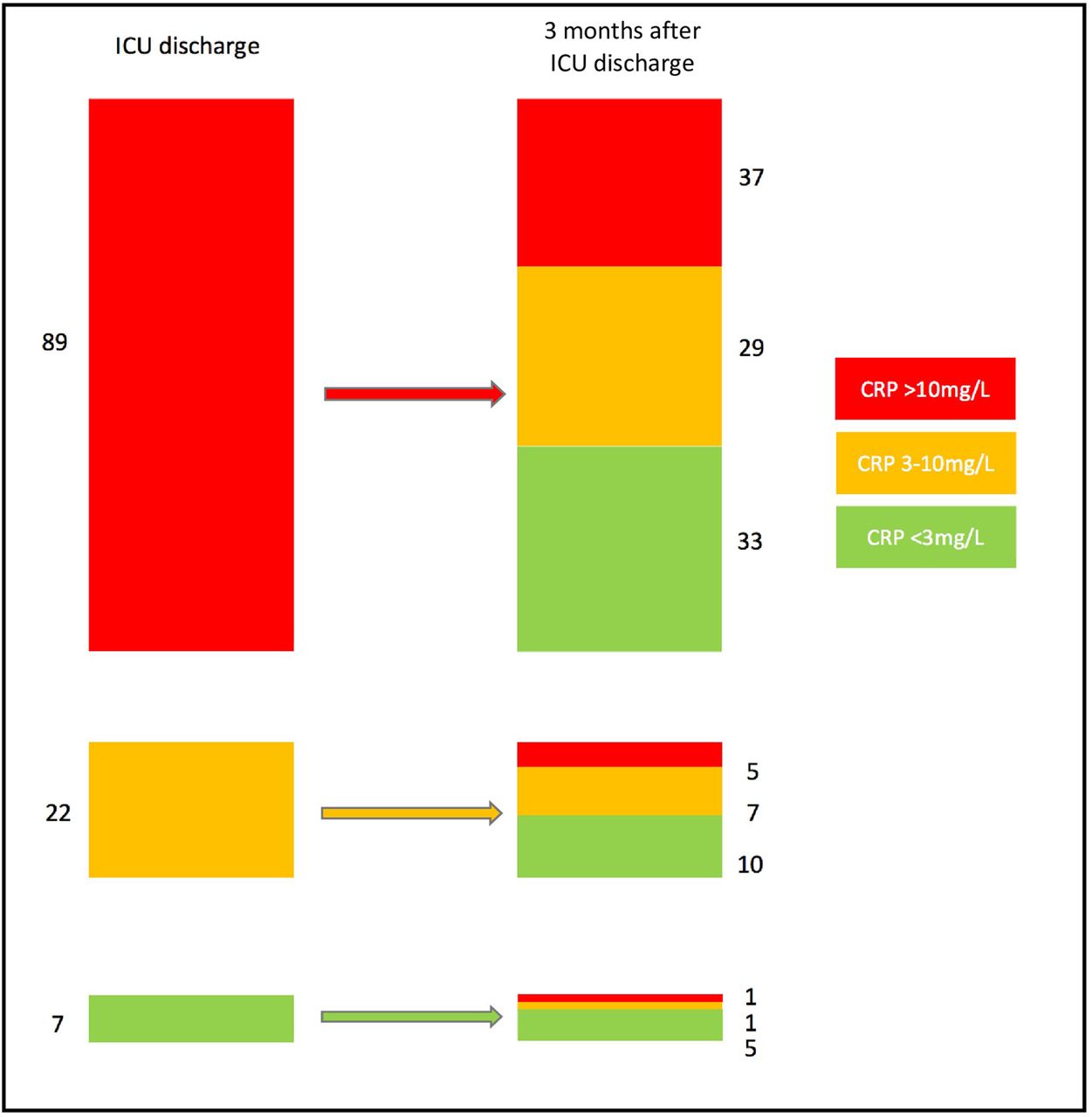
Inflammatory fate of patients with low (<3 mg/L), medium (3–10 mg/L) and high (>10 mg/L) C-reactive protein (CRP) concentration. For the 118 patients with complete data at both time points, patients were categorised at intensive care unit (ICU) discharge, then again at 3 months.
Inflammatory profile
At ICU discharge, HNE, IL-6, IL-8 and SLPI were elevated compared with previously studied healthy populations (table 3). TGFβ1 concentration was reduced. Median concentrations of proinflammatory biomarkers (HNE, IL-6 and IL-8) decreased significantly over the 3-month time horizon (with the exception of IL-1β which was low at both time points). Many patients still demonstrated elevated concentrations compared with the comparative healthy population values. For the proresolution biomarkers, TGFβ1 concentration further decreased at 3 months compared with baseline with values at both time points lower than healthy values. Most patients had suppressed levels of TGFβ1 at both time points. SLPI concentrations decreased over the 3-month period, with most patients having higher values than comparator populations at both time points. Overall, the 3-month pattern at population level was of ongoing inflammation (elevated CRP, HNE and IL8) with evidence of reduced proresolution signalling (reduced/suppressed TFGβ1).
Inflammatory biomarker concentration at baseline and 3 months in patients who survived and had blood sampling at both time points
Relationship with physical recovery
In the univariable analysis, HNE and CRP were significantly associated with RMI 3 months after ICU discharge (table 4), with higher concentrations of these biomarkers being associated with poorer mobility. This association persisted when tested in multivariable linear regression models to adjust for potential confounding factors (age, gender, FCI, APACHE 2 score and days of mechanical ventilation), suggesting HNE and CRP were independently associated with RMI 3 months after ICU discharge.
Linear regression of individual biomarkers with physical outcome measures at 3 months after ICU discharge
IL-8 was significantly associated with HGS at 3 months on univariate testing. After adjustment for confounding, higher concentrations of CRP, IL-8 and SLPI were significantly associated with lower HGS.
There was no significant association observed between inflammatory markers and TUG, or the PCS.
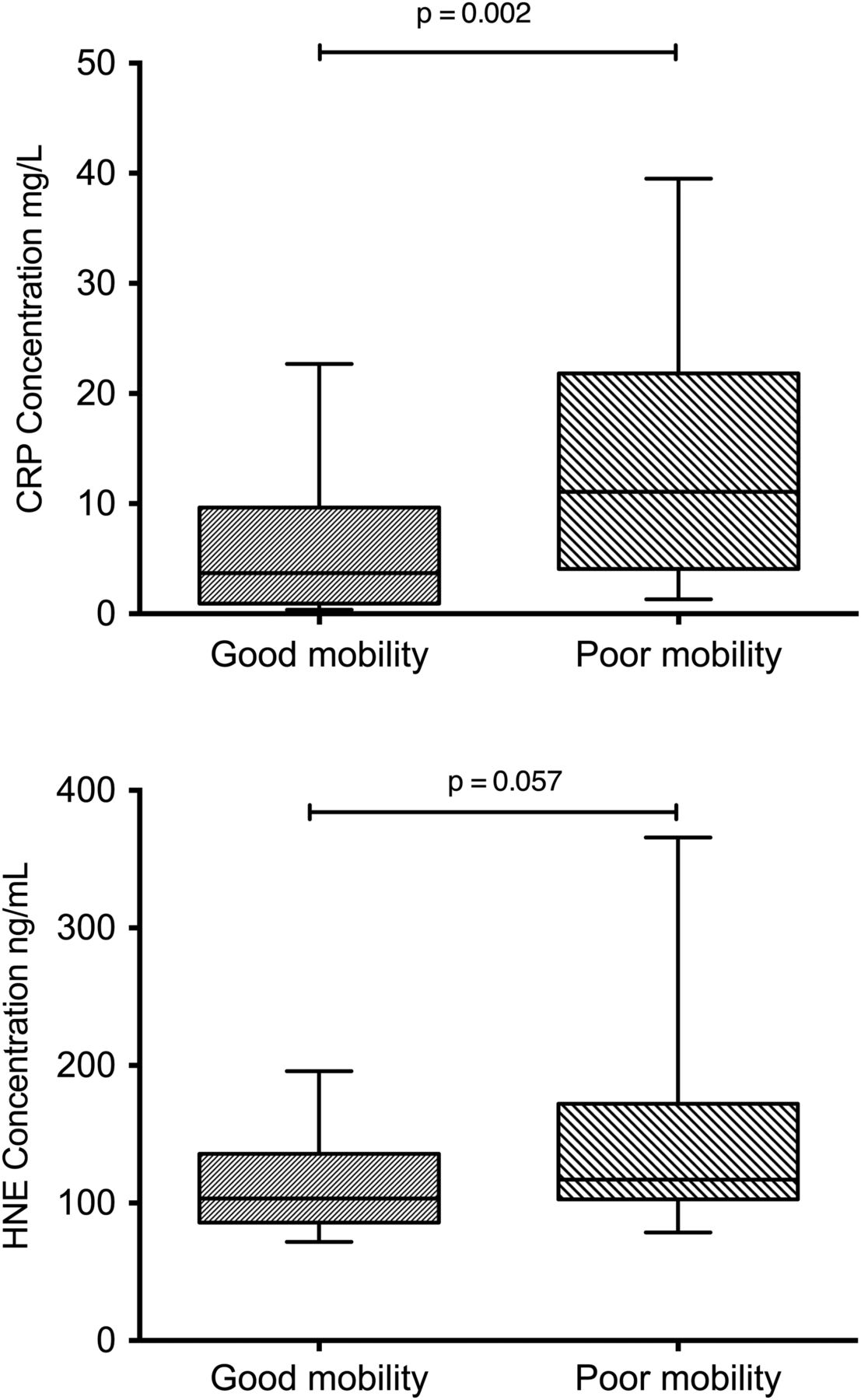
To add clinical context to this relationship we compared HNE and CRP concentration in patients with good mobility (upper three quartiles of RMI (RMI ≥11; n=144)) and poor mobility (lower quartile of RMI (RMI <11; n=31)) at the same time point. Patients with poor mobility had greater CRP concentration (median 11.1 mg/L (IQR 4.1–21.8) versus 3.7 mg/L (IQR 0.9–9.7); median difference 7.3 mg/L (95% CI 2.0 to 10.8; p<0.01)) and HNE concentration (median 117.0 ng/mL (IQR 102.6–172.1) versus 103.2 ng/mL (IQR 85.7–135.8); median difference 13.8 ng/mL (95% CI −1.0 to 42.0; p=0.06)) when compared with patients with good mobility (figure 3).

{kind=link}
{kind=link}
{kind=link}
Box and whisker plots showing C-reactive protein (CRP) and human neutrophil elastase (HNE) concentration in patients with good mobility and poor mobility. Whiskers represent 10th and 90th centiles.
Inflammatory biomarkers at ICU discharge were significantly correlated with biomarkers at 3 months (table 5). To test whether inflammation at ICU discharge was an important confounder of the relationship between persistent inflammation (CRP at 3 months) and recovery (RMI at 3 months), we added CRP at ICU discharge to our earlier linear regression model (table 6). We found no association between CRP at ICU discharge and RMI at 3 months, and adding it as a covariate to the model did not alter the relationship between CRP and RMI when both were measured at 3 months.
Linear relationship between natural log transformed inflammatory biomarkers at baseline (ICU discharge) and follow-up
Sensitivity analysis showing effect of adjusting for CRP at baseline
Role of cytomegalovirus in post-ICU inflammation
At ICU discharge, 115/183 (63%) of patients were HCMV IgG positive indicating previous exposure to HCMV (one patient had insufficient sample to perform IgG analysis). Of the IgG-positive patients, 13/114 of patients (11%) had evidence of lytic infection (detectable HCMV DNA on plasma PCR assay) (one patient had insufficient sample to perform the DNA PCR). At 3-month follow-up, no patients had evidence of ongoing lytic infection.
At ICU discharge, patients previously exposed to HCMV had similar CRP concentrations, but greater concentrations of HNE and a lower concentration of the proresolution mediator TGFβ1 suggesting a more proinflammatory phenotype associated with previous HCMV exposure (table 7). At 3 months, despite an overall fall in inflammatory biomarkers, patients previously exposed to HCMV still had significantly greater circulating HNE and lower circulating TGFβ1. Very small differences in physical outcomes were noted according to previous HCMV exposure, although this reached statistical significance for the TUG test, which was slower in HCMV-positive patients (table 8).
Biomarker concentration according to HCMV exposure group
Comparison of physical outcomes in ICU survivors at 3 months in patients with/without previous HCMV exposure
As HCMV exposure increases with age,37 we assessed the potential confounding role of age (and other baseline variables) in the association between HCMV and physical recovery. Baseline characteristics according to HCMV IgG status are shown in table 9. None of the baseline variables (including age) differed significantly according to HCMV exposure group.
Baseline characteristics according to HCMV exposure
We assessed whether HCMV seropositivity may be a confounder in the relationship between inflammation (measured by CRP) and RMI. We found no independent relationship between HCMV seropositivity and RMI at 3 months. The addition of HCMV seropositivity as a covariate also had no influence on the strength of the relationship between ln(CRP) and ln(16-RMI), which remained highly significant (β 0.15 (95% CI 0.06 to 0.24) p<0.01). These sensitivity analyses are presented in the online supplementary data.
Discussion
In a preplanned secondary analysis of patients enrolled in a randomised controlled trial of a rehabilitation intervention, we demonstrated a high prevalence of systemic inflammation in ICU survivors at ICU discharge and 3 months follow-up. We observed a significant relationship between inflammation and physical recovery that persisted after adjusting for measures of pre-existing co-morbidity and acute illness severity. Patients had evidence of persisting proinflammatory and impaired proresolution signalling during the study period. In an exploratory analysis, we found a more pronounced proinflammatory phenotype in patients previously exposed to HCMV both at ICU discharge and 3 months follow-up. This supports the hypothesis that this might mediate, in part, the association between persisting inflammation and functional recovery.
Our study had a number of strengths. First, the rates of enrolment and follow-up were high, reducing the risk of attrition bias. We also undertook sensitivity analyses in which missing data were imputed to allow us to ensure potential bias from missing data was assessed. Second, we adjusted for likely confounders. The most important was the use of the FCI to adjust for pre-illness physical function (an important determinant of physical recovery after acute illness38). The FCI is a measure of important co-morbidities, which correlates strongly with physical quality of life scores.39 This may not have completely controlled for pre-illness physical function, but is more objective and valid than patient recall of physical abilities. Most previous studies of post-ICU recovery have made no adjustment for preillness health status. We did not adjust for case mix in our analysis primarily because the study was not powered to allow it, but reassuringly observed very little variation in case mix across CRP tertiles. Finally, the measured biomarkers were predefined to reflect initiation, propagation and resolution of the acute inflammatory response to provide a balanced picture of the inflammatory profile.
Our study had limitations. First, our assertion that inflammatory markers were elevated in ICU survivors was based on comparison with previously published data in other populations; these were limited by performance of the assays and the populations studied. Second, our analysis relied on the physical function metrics used in RECOVER, limiting the discriminant ability for studying the pathophysiological processes affecting muscle recovery. Third, our patients were ventilated for >48 h so our findings may not be generalisable to all ICU cohorts. Fourth, we did not adjust our formal analysis for multiple comparisons as it was considered explorative and hypothesis-generating. This may have led to type 1 error. Despite this, for our main end point (adjusted association between CRP and RMI), the p value of 0.001 would remain significant when measured against a Bonferroni-adjusted p value threshold of 0.002. Finally, we could not definitely attribute causality between inflammation and physical recovery because we were unable to establish temporality due to the complex nature of the inflammatory response and the trial design.
Inflammatory persistence in ICU survivors is of potential clinical relevance. We have shown that it is highly prevalent, affecting 50%–67% of survivors 3 months following ICU discharge. This finding is in keeping with a previous study in 24 anaemic ICU survivors who showed elevation of CRP up to 13 weeks after ICU discharge.40 The aetiology of this inflammatory signal is unclear. Persistence of the acute inflammatory response is one mechanism, but other potential explanations such as pre-existing inflammation (with return to baseline), intercurrent infection (eg, subclinical) or an undiagnosed focus of inflammation (eg, within lung or muscle) are also plausible. A high proportion of patients (28%) were readmitted to hospital between ICU discharge and 3 months follow-up in the RECOVER trial. Detailed data concerning the reasons for readmission are not available, and blood for inflammatory profiles was not collected during readmissions. It is possible that the condition requiring readmission resulted in worsening inflammation, which might explain some of our findings. Equally, a persisting inflammatory state may have limited recovery resulting in further hospitalisation. Further research is required to investigate this issue. Of the patients who had blood samples at 3 months, 11/123 (9%) were hospital inpatients at the time. These patients had elevated CRP concentrations (median 15.8 (IQR 11.5–36.0) mg/L versus 3.8 (IQR 1.0–9.4)).
Inflammation at hospital discharge has been associated with higher longer term mortality following acute illness in previous studies,41 but ours is the first to explore the association with physical recovery following critical illness. Persisting physical disability was related to inflammatory response 3 months after ICU discharge but not ICU discharge, suggesting that chronic persistent inflammation is more important than acute inflammation. This may explain why IL-6 and IL-1β, which are early pro-inflammatory mediators, were not associated with late physical function, whereas others (CRP, IL-8, HNE and SLPI) were associated. Another potentially important consideration is that measurement of circulating soluble inflammatory biomarkers may not adequately characterise the host inflammatory response. For example, immune cell functions (eg, neutrophil apoptosis) and inflammatory processes localised to specific sites (eg, skeletal muscle or lung) may not be adequately described. Although our data should be interpreted with caution, they support the hypothesis that a persisting proinflammatory phenotype might mediate poorer physical recovery.
Inflammation is important in acute muscle loss in ICU patients8 and is associated with muscle function in chronic inflammatory disease.9–12 Inflammatory cytokines have an established role in regulating muscle mass; tumour necrosis factor α, IL-6 and endotoxin cause muscle wasting42 due to increased protein catabolism,43 inhibition of protein synthesis,44 inhibition of muscle cell differentiation45 and reduced amino acid uptake.46 It is possible that these processes ‘block’ clinical responses to physical rehabilitation in the early post-ICU period, which might explain the negative results of intervention trials in the early post-ICU period, including the RECOVER trial. Future rehabilitation research should consider including measures of inflammation during recovery in order to understand its importance as an effect modifier, and potentially to inform the optimum timing of interventions. In addition, metrics such as muscle volume and muscle biopsy may provide greater insight into the pathophysiological relationship between inflammation and neuromuscular recovery in future studies.4 ,47
Our finding of a proinflammatory phenotype in patients previously exposed to HCMV was unexpected. The original analysis was planned to explore the importance of active (lytic) infection but the small number of patients that this affected precluded this. Lytic infection is associated with activation of the innate immune system and previous studies have shown that this can last beyond the acute infection and into latency.21 It has been reported that up to 40% of patients reactivate HCMV during critical illness14 so our previously exposed patients may have experienced reactivation at an early stage that was undetectable at our chosen measurement point. It is impossible to discriminate between the relative importance of latent and lytic infection in this study, but our data raise the possibility that HCMV is potentially important in post-ICU inflammation and recovery. Further research in this area is justified, because the clinical effects of HCMV activation are potentially modifiable by antiviral treatment. Two ongoing RCTs (the GRAIL study: NCT01335932 and the CCC study: NCT010503918) may provide more information, but neither will report functional outcome, or longer term inflammatory resolution.
We observed a mean 1 s increase in the time taken to perform TUG in individuals who were HCMV seropositive. While this difference is small, it is a potentially important finding in terms of hypothesis generation, particularly as the RECOVER study found no difference between intervention groups in relation to this measure. Despite this the study was never powered to detect such a difference, and the finding should be interpreted with caution.
In conclusion, we have shown that a systemic proinflammatory state persists for at least 3 months in many patients recovering from critical illness, and is characterised by persisting proinflammatory signals and reduced proresolution signals. Persisting systemic inflammation is associated with poorer physical recovery. Although patients do not demonstrate evidence of ongoing lytic HCMV infection, those with evidence of previous HCMV infection appear to demonstrate a more persisting proinflammatory state that lasts beyond the ICU discharge and is present in some patients 3 months later. Further research is warranted to explore the importance of persisting inflammation as a mediator of recovery following critical illness.
References
Footnotes
Twitter Follow David Griffith at @Griffith_DM
Collaborators RECOVER investigators: T S Walsh, L G Salisbury, J L Merriweather, J A Boyd, D M Griffith, G Huby, S Kean, S J Mackenzie, A Krishan, S C Lewis, G D Murray, J F Forbes, J Smith, J E Rattray, A M Hull, P Ramsay, C Wallis, J Stewart, A Bateman, E Wilson, M Gillies, D Hope, H Dawson, C McCulloch, J Antonelli, L Boardman, L Dow, W Williams, A McCann, S Alexander, J Norrie, M Dennis, C Waldmann and S Brett.
Contributors TSW and DMG conceived the study. TSW, DMG, AGR and SL acquired funding. TSW, DMG, AGR, SL, LS, JM and KT designed the study. DMG and JR performed the biomarker assays. KT coordinated the HCMV analysis. All authors contributed to the interpretation of the summary data and reviewed the final manuscript. All authors approved the final version.
Funding This study was funded by the Chief Scientists Office, Scotland (CZH/4/531, ETM/221).
Competing interests None declared.
Ethics approval Scotland A REC (10/MRE0018).
Provenance and peer review Not commissioned; externally peer reviewed.