Article Text

Abstract
Background The size and concentration of exhaled bioaerosols may influence TB transmission risk. This study piloted bioaerosol measurement in patients with TB and assessed variability in bioaerosol production during normal tidal breathing. Understanding this may provide a tool for assessing heterogeneity in infectivity and may inform mathematical models of TB control practices and policies.
Methods Optical particle counter technology was used to measure aerosol size and concentration in exhaled air (range 0.3–20 µm in diameter) during 15 tidal breaths across four groups over time: healthy/uninfected, healthy/Mycobacterium tuberculosis-infected, patients with extrathoracic TB and patients with intrathoracic TB. High-particle production was defined as any 1–5 µm sized bioaerosol count above the median count among all participants (median count=2 counts/L).
Results Data from 188 participants were obtained pretreatment (baseline). Bioaerosol production varied considerably between individuals. Multivariable analysis showed intrathoracic TB was associated with a 3½-fold increase in odds of high production of 1–5 µm bioaerosols (adjusted OR: 3.5; 95% CI 1.6 to 7.8; p=0.002) compared with healthy/uninfected individuals.
Conclusions We provide the first evidence that intrathoracic TB increases bioaerosol production in a particle size range that could plausibly transport M. tuberculosis. There is substantial variation in production within patients with TB that may conceivably relate to the degree of infectivity. Further data is needed to determine if high bioaerosol production during tidal breathing is associated with infectiousness.
- Tuberculosis
- Infection Control
- Respiratory Infection
Statistics from Altmetric.com
Key messages
What is the key question?
Does the presence of active TB increase bioaerosol production during normal tidal breathing in a particle size range that could plausibly transport Mycobacterium tuberculosis?
What is the bottom line?
Our study provides the first evidence that intrathoracic TB increases bioaerosol particle production in a particle size range that could plausibly transport Mycobacterium tuberculosis and that there is substantial variation in production within patients with TB that may plausibly relate to the degree of infectivity.
Why read on?
Our findings suggest that measures of bioaerosol production may contribute to assessments of infectiousness and TB transmission risk.
Introduction
An estimated 9.1 million TB cases occurred worldwide in 2013 and global incidence is declining at <2% per year.1 There are a reported 450 000 new cases of multi-drug-resistant TB (defined as Mycobacterium tuberculosis resistant to at least rifampicin and isoniazid) worldwide who remain infectious for longer periods of time.1 This highlights the importance of identifying better markers of infectivity which would particularly relevant for informing control. Molecular typing studies have shown some individuals generate high numbers of secondary cases.2 This may be due to: behavioural factors; increased transmissibility of infecting strains or host biological/clinical factors affecting how many infectious particles each patient generates. Aside from sputum-smear positivity, presence of cough, pulmonary cavitary disease and laryngeal disease, which are known to be strongly associated with infectivity, other determinants of TB infectivity are poorly defined.
The size and concentration of exhaled particles may influence respiratory infection transmission risk.3 Defining a particle diameter cut-off at which aerodynamic particle behaviour changes is not possible, although the WHO uses 5 µm to distinguish between droplet and airborne transmission.4 Bioaerosols (<5 µm) are responsible for airborne transmission. These smaller bioaerosols once expelled remain suspended in air for long periods of time exposing a greater number of contacts at greater distances to potential infection.3 ,5–7 They are formed in the lower respiratory tract and contain lung mucus, surfactant and pathogens.8–10 While a single cough predominantly produces large droplets measuring >5 µm7 it also produces large numbers of bioaerosols.8 ,11 ,12 However, as normal breathing is continuous, the majority of bioaerosols are in effect produced by normal breathing,11–14 with some studies reporting up to 10 000 bioaerosols per litre.15
Evidence suggests bioaerosols contribute to infectious disease transmission.10 ,15–19 Bioaerosols with a critical size range of 1–5 µm, once inhaled, have a higher probability of reaching and depositing in alveolar regions than those >5 µm.20 The M. tuberculosis bacillus is 0.2–0.5 µm wide and 2–4 µm long and so it is bioaerosols measuring 1–5 µm that may plausibly serve as vehicles of this pathogen, permitting infection of alveolar macrophages in distal portions of lungs.8 Given TB transmits via bioaerosols and most bioaerosols measuring <5 µm are produced during normal breathing, variations in bioaerosol production during normal tidal breathing may be a determinant of infectivity.
Nicas et al21 defined super-spreaders, ‘as those infrequently encountered persons with high cough and/or sneeze frequency, elevated pathogen concentration in respiratory fluid, and/or increased respirable aerosol volume per expiratory event such that their pathogen emission rate is much higher than average’. Modelling studies suggest super-spreading is a normal feature of many infections and have demonstrated substantial heterogeneity in transmission for various respiratory infections.22 ,23 Yet this feature had until recently been largely neglected in transmission models. The lack of data to inform parameters on individual variability in infectiousness over time has been highlighted.24 TB control is highly reliant on transmission models to inform national guidance. Such models may provide more accurate predictions if variations in infectiousness are explicitly considered.
Contact tracing decisions are often guided by perceived infectiousness of index cases and may be based on the presence of sputum-smear-positive disease and extent and duration of cough.25 Additional criteria to identify particularly infectious cases could help target contact tracing activities.
Large-scale prospective studies of TB cases and their contacts are required to assess the importance of variations in bioaerosol production on transmission. We have already shown the feasibility of measuring bioaerosols in healthy volunteers using optical particle counter (OPC) technology that measures the size and concentration of particles in exhaled breath during normal tidal breathing.5 This study makes an important next step by piloting OPC technology in patients with intrathoracic, extrathoracic and latent TB compared with healthy controls.
Methods for data collection
Bioaerosol production measurements were obtained from four groups: healthy/uninfected volunteers recruited as a convenience sample of university personnel (group 1); healthy/M. tuberculosis-infected patients: non-infectious with no evidence of active TB as evidenced by a significant reaction (≥10 mm in duration) to a Mantoux tuberculin skin test and/or a positive interferon-γ release assay (IGRA) result (group 2); patients with active extrathoracic TB (clinical, radiological and pathological evidence of granulomatous lesions external to thoracic cavity and positive cultures for M. tuberculosis but with no clinical or radiological evidence of pulmonary or hilar or mediastinal involvement) (group 3) and patients with active intrathoracic TB (radiological and pathological evidence of lung cavitation and/or caseating and non-caseating granulomas, tubercles and fibro-caseous lesions in lung and/or hilar and/or mediastinal lymph nodes) confirmed by positive cultures and/or PCR for M. tuberculosis (group 4). We grouped those classified as pulmonary or intrathoracic as there was a high degree of overlap and it can be difficult to exclude pulmonary involvement in mediastinal disease.
Group 1 was recruited during the previous study measuring bioaerosol production by healthy volunteers.5 Groups 2–4 were recruited from University College London NHS Foundation Trust (UCLH) TB service. Patients with active TB were enrolled at the start of antituberculous treatment (at baseline) and followed up every 4–8 weeks over the course of treatment. Bioaerosol measurements were also obtained from active cases during the course of treatment and similarly followed up. Repeated cycles of bioaerosol measurements were obtained from all participants (healthy volunteers and patients with TB).
Data on age, smoking history, height, weight, immunological markers (C-reactive protein and erythrocyte sedimentation rate), HIV status, sputum-smear status, presence of prior BCG vaccination, antituberculous treatment start and end dates and any chronic illness were extracted from patient notes. Presence or absence of latent TB infection (based on Mantoux testing and/or IGRA testing) in contacts was obtained through record review.
Bioaerosol measurement procedure
The OPC device (Exhalair (model 102580-AK), Pulmatrix, Lexington, Massachusetts, USA), measured aerosol size and concentration using OPC coupled with respiratory flow rate and volume measurements.
Participants breathed into a disposable mouthpiece while wearing a nose clip to prevent nasal breathing. One-way valves and bacterial/viral high-efficiency particulate air filters in disposable tubing prevented inhalation of infectious particles from the environment. Exhaled particles (range of 0.3–20 µm in diameter) over the course of 15 tidal breaths were measured (marked in green in figure 1).

Respiratory bioaerosol measurement using optical particle counter technology using Exhalair system.
Three bioaerosol measurement cycles were obtained at each participant session from the start of antituberculous treatment (at baseline) and at repeated follow-up sessions every 4–8 weeks (during normal scheduled outpatient visits) over treatment course. Each measurement cycle commenced with an initial calibration to reduce measurement error. Following initial calibration, a washout period followed (which included three deep breaths to clear any ambient particles from the respiratory tract). Exhaled bioaerosols were collected and arranged into four channels according to size ranges: ≥0.3 to ≤0.5 µm, >0.5 to ≤1 µm, >1 to ≤5 µm and >5 µm. Each cycle lasted up to 2 min to complete.
Ethical approval for the initial cohort study for group 1 participants was received by University College London Ethics Committee (reference number 1564/001). Ethical approval for groups 2–4 was secured from National Research Ethics Service (NRES)—City & East (REC study reference number 11/LO/1601) and R&D approval from UCLH/UCL/RF Joint Research Office (reference number 11/0256). All participants provided written informed consent.
Statistical analysis strategy
The dataset included up to three bioaerosol measurement cycles per participant per session, each representing the average number of bioaerosols exhaled over the course of 15 tidal breaths. Given the right-skewed distribution of the 1–5 µm bioaerosol count/L, the data were log-transformed and normality was assessed using kernel density plots. The correlation between repeated measurement cycles (first vs second, first vs third and second vs third) were calculated using linear regression models of log-transformed bioaerosol count data using the Stata regress command. Since this indicated greater correlation between second and third readings than between first readings and subsequent readings we used the mean of the second and third readings as the main measure of bioaerosol production for each session.
The distribution of 1–5 µm bioaerosol counts and log-transformed counts across the four clinical groups were explored using histograms. The geometric mean counts and 95% CIs for these groups were also compared. We focused on this particle distribution size as an M. tuberculosis is 0.2–0.5 µm wide and 2–4 µm long so this size of bioaerosol particles would be plausibly expected to be involved in transmission of M. tuberculosis bacilli. Comparison of bioaerosol counts in each of the four groups was explored further by comparing geometric means counts and 95% CIs.
We explored the effect of demographic, clinical and microbiological risk factors on 1–5 µm and submicron bioaerosol production patterns at baseline using stepwise selection for logistic regression models, using bioaerosol counts as a binary outcome variable (above and below the median count) to control for confounders. The explanatory variables considered included gender, age, ethnicity, immigrant status (ie, UK born or not), current smoking status, BCG vaccination status, sputum-smear status and environmental factors including season, indoor and outdoor temperature and humidity. Univariate models were initially built and variables which predicted the outcome and were associated with the main exposure of interest (as defined by the four clinical groups’ disease category) at p<0.05 were retained for multivariable analysis if they appreciably altered the crude ORs.
Clustering between repeat measurement sessions within individuals was adjusted for in the final multivariable model using robust SEs.
Based on our previous work showing that the first reading within a measurement session was poorly correlated with second and third readings in the session, we excluded the first reading from subsequent analyses.5 All analyses were performed using STATA V.13.0, IC (College Station, Texas, USA).
Results
Baseline characteristics
A total of 188 participants were analysed at baseline (table 1), of which 86 (45.7%) were healthy/uninfected individuals (group 1), 27 (14.4%) were healthy/M. tuberculosis-infected patients (group 2), 11 (5.9%) were diagnosed with extrathoracic TB (group 3) and 64 (34.0%) were diagnosed with intrathoracic TB (group 4). More than half of the cohort, 108 (57.5%) were female. The median age of participants was 33 years old.
Descriptive characteristics of 188 individuals at baseline
Distribution of 1–5 µm diameter bioaerosols in exhaled air
Bioaerosols in the 1–5 µm diameter range expired during normal tidal breathing at baseline by all participants formed a highly right-skewed log-normal distribution. Correlation coefficients from linear regression models showed second and third bioaerosol measurements from within a single session were most strongly correlated, where the correlation coefficient was 0.6 (95% CI 0.5 to 0.7; p<0.001). Subsequent analyses focus on these measurements as the first measurements within a session appeared to be less consistent. The first measurements were excluded from subsequent analyses.
Supplementary table
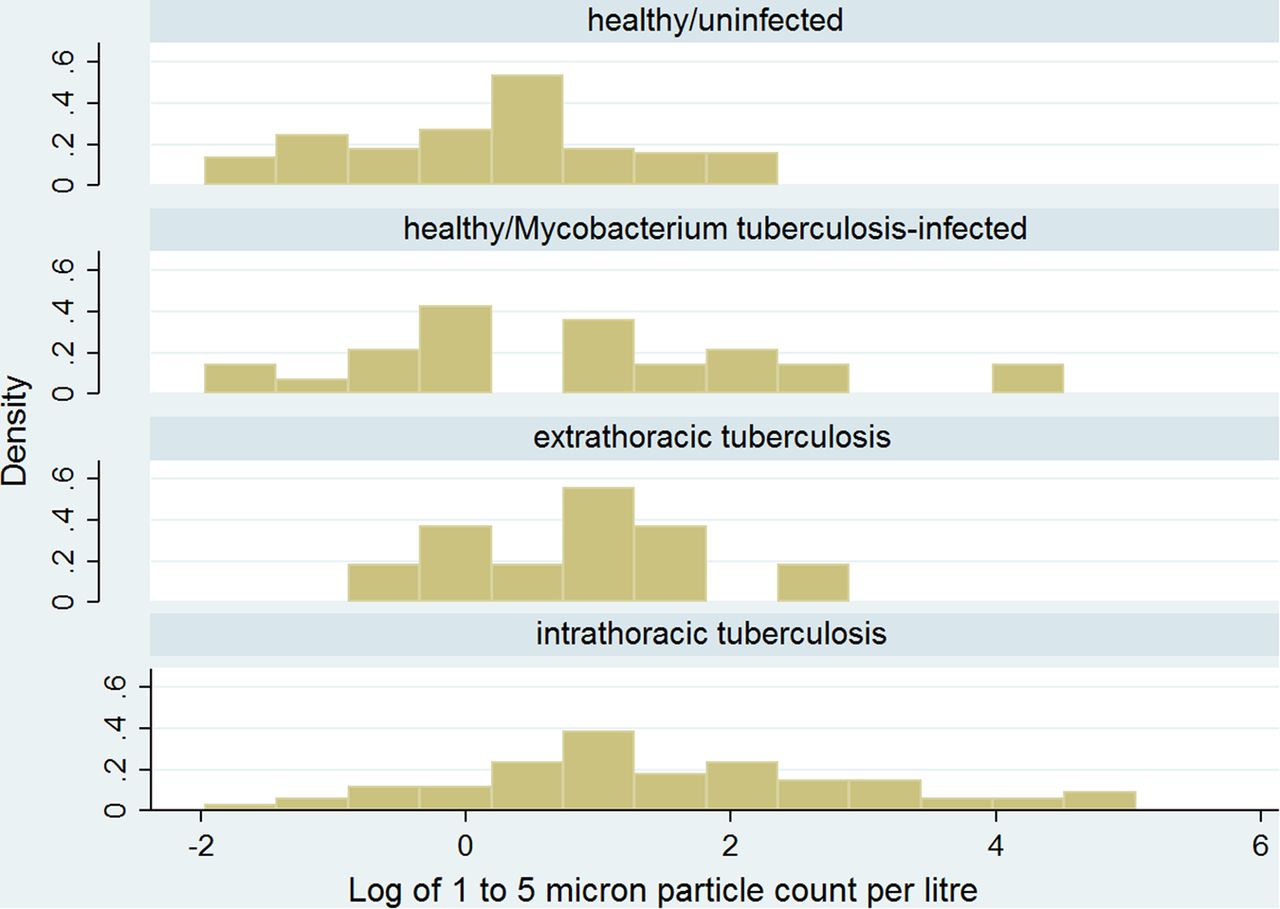
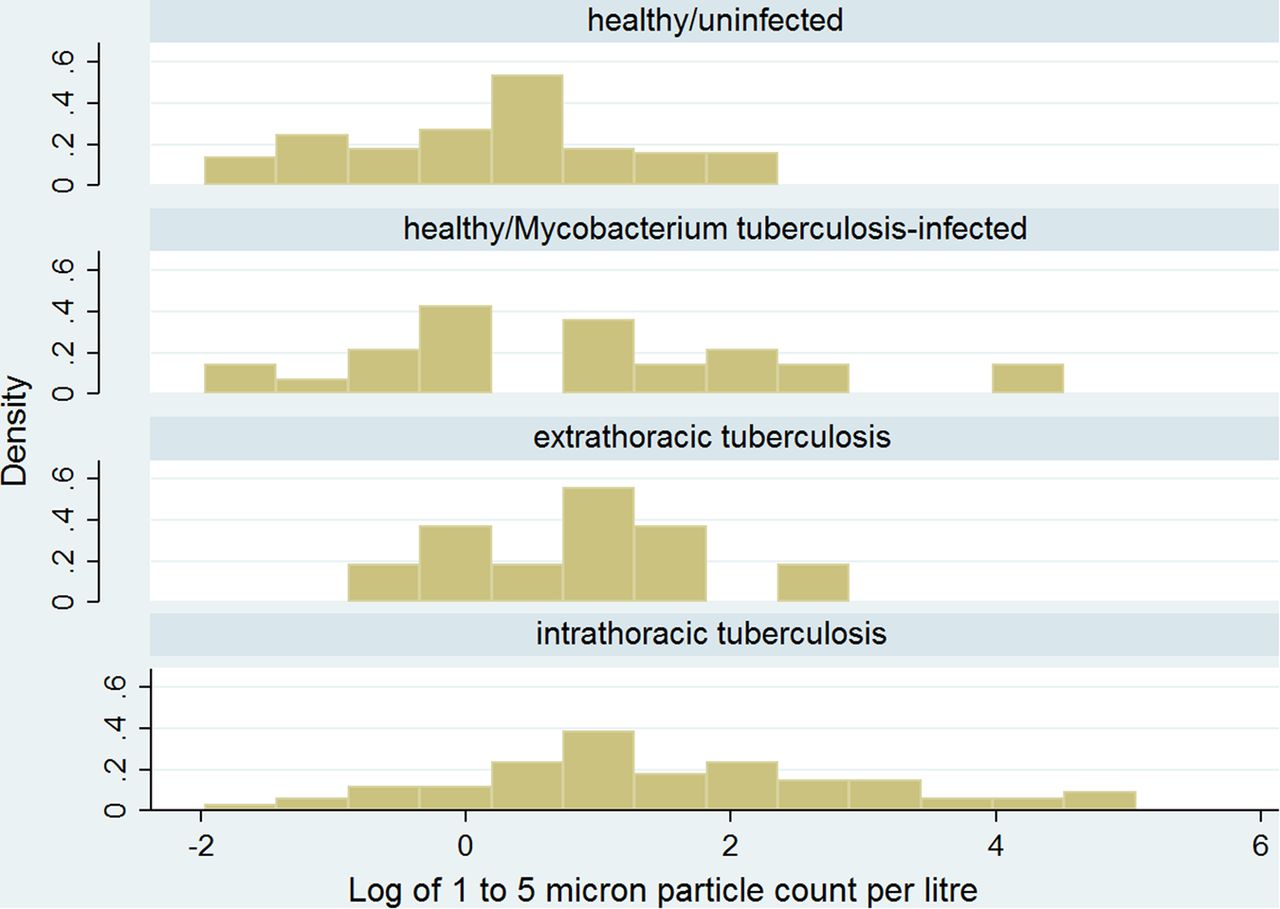
Comparison of distributions of log-transformed 1–5 µm bioaerosol counts across all clinical groups showed participants diagnosed with active TB (irrespective of intrathoracic or extrathoracic disease) had higher baseline bioaerosol counts than those of healthy/M. tuberculosis-infected or healthy/uninfected participants (figure 2). On comparison, the geometric mean for healthy/uninfected participants 36.3 counts/L (95% CI 30.1 to 43.8); for healthy/M. tuberculosis-infected participants 29.7 counts/L (95% CI 16.9 to 52.4); for active extrathoracic cases was 52.6 counts/L (95% CI 16.7 to 166.3) and for active intrathoracic cases was 67.6 counts/L (95% CI 46.3 to 98.8).
{kind=link}
{kind=link}
Log-transformed distribution of 1–5 µm bioaerosol production across all four groups: healthy/uninfected individuals, healthy/Mycobacterium tuberculosis-infected, patients with extrathoracic TB and patients with intrathoracic TB at baseline.
Risk factors associated with 1–5 µm diameter bioaerosol production
High-particle production was defined as any particle count above the median particle count among all study participants (median 1–5 µm, count=2 counts/L). Table 2 shows the relationship between 1 and 5 µm bioaerosol count as a dichotomous outcome variable and risk factors. In multivariable analysis, intrathoracic TB was strongly associated with substantially increased odds of being a high-particle producer (adjusted OR: 3.5; 95% CI 1.6 to 7.8; p=0.002) compared with healthy uninfected controls. There was also a suggestion that those with extrathoracic or latent infection had increased odds of high-particle production, although these trends were not significant and larger studies would be needed to investigate this further. Age group also remained significantly associated in the final model with those aged 40–49 years being most likely to have high bioaerosol counts (adjusted OR: 6.0; 95% CI 2.5 to 14.2; p<0.001). There was insufficient data to examine trends in bioaerosol production over treatment course.
Final multivariable model: relationship between 1 and 5 µm bioaerosol production and baseline characteristics across all groups
Discussion
This is the first time bioaerosol size distribution and variation during normal tidal breathing in patients with intrathoracic and extrathoracic TB has been studied using OPC technology. Our findings demonstrate marked variability in bioaerosol production by patients with TB and provide evidence that those with intrathoracic TB are more likely than healthy controls to produce high levels of bioaerosols in the 1–5 µm range. Substantial variation in bioaerosol production between patients with intrathoracic TB may plausibly be associated with variations in infectivity, since M. tuberculosis is an obligate aerosol transmitter. Given that M. tuberculosis has been found in cough-generated aerosols of the same size range as measured in this study during normal breathing16 and so it is conceivable that bioaerosols produced during continuous tidal breathing could transport M. tuberculosis within a size range that could be inhaled by a susceptible contact and deposited in the distal portions of the lung eliciting M. tuberculosis infection. More research, however, is needed to define how such variations correlate with infectivity and transmission risk. Such research may include, for example, studies of the comparative contribution of normal breathing and explosive respiratory events such as cough or sneezing to bioaerosol production, concentration of pathogen-laden and/or infectious bioaerosols in exhaled breath, and larger studies assessing how baseline measures of bioaerosol production in index cases relate to the risk of infection in contacts. There is also a need to conduct large-scale research to assess whether bioaerosol counts change through the course of treatment.
The mechanics of bioaerosols generation vary depending upon respiratory manoeuvres, namely coughing, sneezing and normal tidal breathing. Bioaerosols are formed through a rapid passage of airflow over the respiratory surfaces leading to shear forces along the mucous layer, creating wave-like disturbances hence bioaerosol formation. In a healthy individual a typical cough has a biphasic profile, starting with an initial high velocity phase and followed by diminishing flow rate, lasting approximately 0.5 s. Coughing is likely to be infrequent and while it results in higher flow velocities, the predictive value of cough-generated aerosols over time and outcomes in susceptible contacts is not fully understood. Furthermore, explosive respiratory manoeuvres-like coughing predominantly generate larger bioaerosols, depositing in the upper respiratory tract than in alveolar regions and so the assessment of cough alone may be a poor index of infectiousness. By virtue of low inertia, pathogen-laden bioaerosols measuring <5 µm produced by continuous normal tidal breathing will travel greater distances potentially reaching a wider range of susceptible contacts than that produced by infrequent coughing.
It is widely accepted that the spread of M. tuberculosis from an index case with pulmonary or laryngeal TB to susceptible contacts underpins transmission of TB. Our findings show that the presence of intrathoracic disease was associated with high bioaerosol production during normal breathing. This offers additional insights into the pathophysiology of active TB and presents implications for the risk assessment of suspected index cases. Persistence of bioaerosol production during normal tidal breathing over treatment course in patients with TB may serve as an additional determinant of infectivity but more large-scale work to explore the relationship between bioaerosol production and treatment needs to be done.
There are some study limitations: our study measures variations in bioaerosol production but did not measure infectious particle concentration, limited numbers of cases with extrathoracic disease limited conclusions in this group, the study was also not sufficiently powered to explain how additional clinical features affected bioaerosol production, whether bioaerosol production changed through treatment or to assess the impact of bioaerosol production on risk of infection in contacts. We only assessed bioaerosol production during normal tidal breathing and not during coughing and we do not know if the bioaerosols we detected contained viable M. tuberculosis bacilli. There would also be valuable in repeating the work in high incidence settings and in settings where HIV is highly prevalent to determine if findings are generalisable. Due to the highly skewed nature of the data, we chose to categorise bioaerosol counts as above and below median rather than model it as a continuous variable. There is no prior literature on what level of bioaerosol count should be considered high, so this cut-off is to some extent arbitrary. However, it has the advantage of being a common and well-understood measure of central tendency and one which helped maintain reasonable sized groups for comparison. Nevertheless, the study provides the first evidence that intrathoracic TB increases bioaerosol particle production in a particle size range that could plausibly transport M. tuberculosis and that there is substantial variation in production within patients with TB that may plausibly relate to the degree of infectivity.
Further research on this phenomenon could inform TB control policy, for example, through better mathematical model parameterisation, improved clinical risk assessment of index cases, targeting of infection control and outbreak investigation strategies and case management decisions for isolation of patients with newly emergent strains and contact tracing measures.
Acknowledgments
We thank the optical particle counter manufacturer, Pulmatrix for technical support throughout the study period. We also acknowledge Dr Katherine Fielding for providing statistical advice. We thank all of the clinicians and TB specialist nurses at UCLH TB service for all their efforts in supporting the recruitment process and referral of patients to the study.
References
Footnotes
Contributors FBW has been the study coordinator and project managed this study since its inception and previous bioaerosol pilot work in healthy volunteers; FBW analysed the data supervised by SDL and ACH; FBW codesigned the study with ACH and PS; led the ethics and R&D approval processes and led recruitment and data collection. PS was the chief investigator for the study. HB served as the local principal investigator at the study site and provided on-site supervision of recruitment and data collection. ACH, SDL and FBW developed the statistical analysis strategy. PS, ACH, SDL and HB provided academic and strategic input throughout the course of the study. All authors have seen and approved the final version of the abstract for publication.
Funding This work was supported by the Clinical Research and Development Committee (CRDC)—UCLH Charities Fast Track grant; CRDC Reference: F170.
Competing interests None declared.
Ethics approval National Research Ethics Service (NRES)—City & East (REC study reference number 11/LO/1601).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves