Article Text

Abstract
Importance COPD is the third leading cause of death worldwide. Mortality trends offer an indication of how well a society is doing in fighting a disease.
Objective To examine trends in all-cause, lung cancer, cardiovascular and COPD mortalities in people with COPD, overall and in men and women.
Design, setting, participants Population, cohort study using health administrative data from Ontario, Canada, 1996 to 2011.
Exposure A previously validated COPD case definition was used to identify all people with COPD.
Main outcomes and measures All-cause, lung cancer, cardiovascular and COPD mortality rates were determined annually from 1996 to 2011 overall, and in men and women. All-cause trends were compared with all-cause trends in the non-COPD population. All rates were standardised to the 2006 Ontario population.
Results The prevalence of COPD was 11.0% in 2011. Over the study period, all-cause mortality decreased significantly more in men with COPD than the non-COPD population. The same was not observed in women. COPD-specific and lung cancer mortalities, which started higher in men with COPD, decreased faster in them than in women with COPD with the two rates becoming more similar over time. Cardiovascular disease mortality declined at a relatively equal rate in both sexes.
Conclusions and relevance Mortality in people with COPD has decreased; however, the decrease has been greater in men than in women. Public health interventions and medical care appear to be improving mortality in individuals with COPD but more research is needed to determine if they are benefiting both sexes equally.
- COPD epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
-
What are mortality trends in people with COPD and are they the same in men and women?
What is the bottom line?
-
Declines in mortality over the years may have benefited men but not women.
Why read on?
-
We need public health interventions and medical care that will benefit people of both sexes who have COPD.
Introduction
Mortality trends offer an indication of how well a society is doing in fighting a disease. COPD is the third leading cause of death worldwide and a highly prevalent, preventable and manageable chronic disease associated with significant morbidity.1–3 Unlike cardiovascular disease and stroke which have had declining mortality for decades, COPD-specific mortality rates appeared to be increasing until as recently as 2002.4 Since then declining COPD mortality rates1 have been attributed to reductions in smoking and the development of newer COPD medications and other management practices.1 ,5
People with COPD also commonly die of other causes—most notably cardiovascular disease and lung cancer—and their COPD likely contributes to these deaths either by contributing to its underlying cause or by reducing patients’ physiological reserve.6 Consequently, since COPD is also often underreported as a cause of death,7 all-cause mortality might be a better indicator than COPD-specific mortality of the burden of disease in this population. Previously we demonstrated a declining trend in all-cause mortality in the COPD population8; however this could have been because of decreasing mortality trends, led by improvements in cardiovascular mortality, in the general population.9 Ideally this all-cause trend would be referenced to trends in the non-COPD population to see if they differed. There is also little known about how all-cause mortality trends differ between men and women with COPD.
Therefore, to determine how well society is doing to combat COPD we conducted a population-based study to examine and compare trends in all-cause, lung cancer, cardiovascular and COPD mortalities in men and women with COPD using the non-COPD population as our reference. We also examined potential years of life lost (PYLL).
Design and methods
Study design and setting
We conducted a longitudinal, population study of mortality trends of people with COPD from 1996 to 2011 in Ontario, the largest province of Canada with a large, diverse multicultural population of more than 13 million residents.
Data sources
Residents of Ontario have universal public health insurance under the Ontario Health Insurance Plan, the single payer for all medically necessary services across the full spectrum of residents, providers and hospitals. Service details are captured in health administrative databases which can be linked on an individual level to provide a complete health services profile for each resident. Three Ontario population health administrative databases were used. The Registered Persons Database contains basic demographic information, including date of death from probabilistic linkage of death-certificate information which is cross-referenced with records of deaths from hospitals and long-term care facilities.10 The Canadian Institute of Health Information Discharge Abstract Database contains information on all discharges from acute care hospitals. The Ontario Health Insurance Plan Physician Claims database contains information on all services provided by fee-for-service physicians and ‘shadow-billings’ for the few physicians paid under alternate payment plans that do not include a fee-for-service component (but who are expected to maintain their shadow billings at certain levels or else have their remuneration decrease). These databases provided data from 1 April 1996 to 31 March 2012 (fiscal years 1996–2011). We also used Statistics Canada annual population estimates based on census counts and on projected intercensal counts to obtain number of persons living in the province of Ontario on 1 July of each study year. Finally, we used the Ontario Registrar General Death database which captures all deaths and their causes for all residents of Ontario from calendar years 1996 to 2009. Using similar methods as those used in other countries,11 ,12 the Registrar General Death database classifies cause of death using up to two diagnostic fields before 2002 and one primary and up to 12 contributing diagnostic fields from 2003 onwards. In this study, we classified cause of death using the two diagnostic fields (immediate or antecedent if the immediate field was empty) before 2002, and the primary cause of death diagnostic field from 2003 onwards. Diagnostic coding is based on WHO's International Classification of Diseases (ICD)-9 before 1999, and ICD-10 from 2000 onwards.
Study population and exposure
All individuals living in Ontario were included. Individuals with physician diagnosed COPD were identified using a case definition of one or more COPD physician billing claims and/or one or more COPD hospital discharges. Individuals had to be over the age of 35 years when their claims or discharge occurred. This COPD case definition was previously validated against a clinical reference standard and found to have a sensitivity of 85.0% (95% CI 77.0% to 91.0%) and a specificity of 78.4% (95% CI 73.6% to 82.7%).13 Once patients were identified as having COPD, they were presumed to have it for life.
Mortality
Deaths due to all causes in the COPD and non-COPD population were identified using the Registered Persons Database. The Ontario Registrar General Death database was used to determine deaths due to a primary cause of COPD, cardiovascular disease or lung cancer in the COPD population between 1996 and 2009 (see online supplementary eTable 1).
Covariates
To describe the cohort, age, sex, place of residence (rural or urban), socioeconomic status, history of cardiovascular disease and lung cancer in the past 5 years were determined as of 1 April 2011. Rural status was based on Statistics Canada's definition of rurality.14 Socioeconomic status was inferred from neighbourhood income derived from postal codes and census data.15 A history of cardiovascular disease and lung cancer in the previous 5 years was defined using the same ICD codes as used to define mortality (see online supplementary eTable 1).
Analysis
Annual all-cause mortality rates were calculated for the COPD and non-COPD populations by dividing the number of all-cause deaths in each by their total populations. Annual COPD, cardiovascular disease and lung cancer mortality rates were calculated for the COPD population by dividing the total number of deaths for each by the COPD population. All results were stratified by sex.
To compare mortality rates among different years, age-sex direct standardised rates were calculated using the 2006 Ontario population as the reference year (a census year). We calculated 95% CIs using the gamma distribution and the relative percentage changes in rates between two fiscal years using the rate in the earlier year as the reference. We tested for trends over time using the Cochran-Armitage trend test. A negative binomial regression with interaction terms between year, population (COPD and non-COPD population) and sex, adjusting for age was used to determine if mortality rates in those with COPD differed from those without or if rates differed by sex over time. The yearly non-COPD population estimates were used as the offset.
The annual rates of PYLL per 1000 Ontarians among the COPD and non-COPD populations were calculated by multiplying the number of deaths in each age group by the age weights divided by the number of people in that group and then multiplying by 1000. We used Ontario's standard life expectancy of 77.4 years for men and 82.0 years for women. Results were stratified by sex.
All statistical tests used p<0.05 as the level of significance and were performed using SAS, V.9.1 (SAS Institute, Cary, North Carolina, USA).
Research ethics approval
Research ethics approval was obtained from the institutional review board at Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada.
Results
There were 415 311 people with COPD in Ontario in 1996 (7.5% of the population) which increased to 836 139 in 2011 (11.0% of the population). Individuals with COPD were older, less likely to live in urban areas, more likely to be of lower socioeconomic status, and more likely to have cardiovascular disease and lung cancer than the non-COPD population, see table 1.
Demographic and clinical characteristics of individuals with COPD and the non-COPD population, Ontario, Canada
All-cause mortality
After adjusting for age, all-cause mortality in the COPD population was more than three times higher than mortality in the non-COPD population (rate ratio 3.57, 95% CI 3.49 to 3.64; p<0.001). Between 1996 and 2011, there was a 0.98 reduction in mortality in each year (95% CI 0.97 to 0.98; p<0.001).
Age-adjusted all-cause mortality was plotted by sex and COPD over time (figure 1). Mortality among men was 1.41 times higher than in women (95% CI 1.38 to 1.44; p<0.0001) in the main model. All-cause mortality declined more in men than in women in the COPD population (40.6% compared with 30.0%, p=0.008) but fell a similar amount for men and women in the non-COPD population (33.0% compared with 34.9%, p=0.631). Mortality rates in men with COPD declined more than men in the non-COPD population (p=0.047), while mortality rates in women with COPD declined the same amount as women in the non-COPD population (p=0.214).

Adjusted all-cause mortality rates per 1000 Ontarians with and without COPD from 1996 to 2011, overall and stratified by sex. aOverall mortality rates are adjusted for age and sex. Mortality rates stratified by sex are adjusted for age. bYears represent fiscal years, for example year 1996 represents 1 April 1996 to 31 March 1997.
COPD mortality
Age-sex standardised COPD mortality was 2.9 per 1000 persons (95% CI 2.8 to 3.0) in 1996 and fell 34% to 1.9 per 1000 persons (95% CI 1.8 to 2.0) in 2009 (p<0.001). COPD mortality started out higher but declined faster in men than in women (p=0.004) (figure 2). In contrast, the absolute number of people dying with COPD increased by 28% from 1996 to 2009. This increase was mostly borne by women (figure 3).
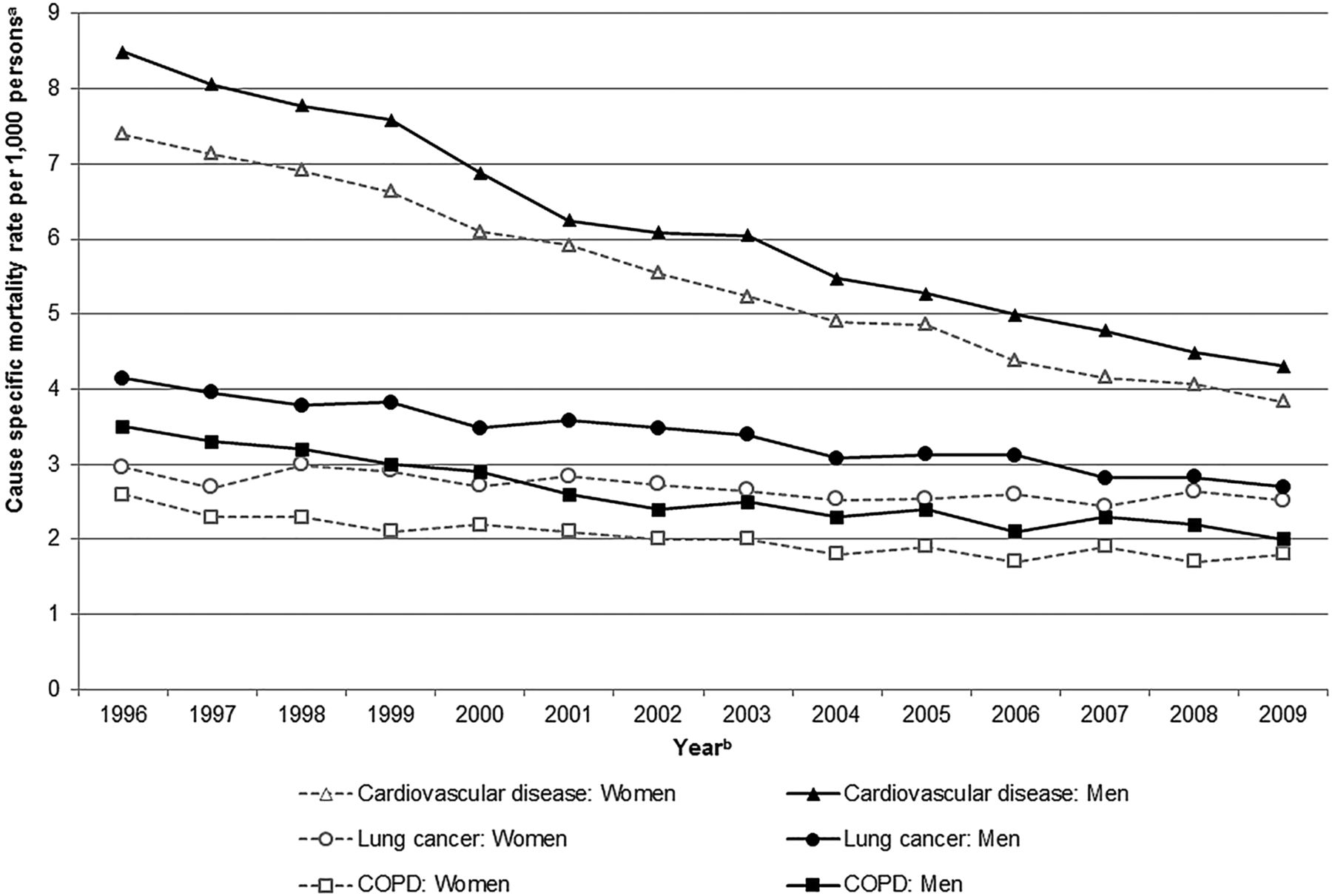
Adjusted mortality rates per 1000 individuals with COPD by cause of death in Ontario, Canada from 1996 to 2009, stratified by sex. aMortality rates are adjusted for age. bYears represent calendar years. Data for cause-specific mortality was only available up to 31 December 2009.

Absolute number of deaths from cardiovascular disease, lung cancer and COPD in individuals with COPD by sex and absolute number of people with COPD by sex, 1996–2009. aYears represent calendar years. Data on cause-specific death was only available up to 31 December 2009. Dark bars represent men and light bar represent women.
Cardiovascular and lung cancer mortality trends in the COPD population
Age-sex standardised mortality rates for cardiovascular disease and lung cancer declined in the COPD population between 1996 and 2009 (p<0.001 for both) (figure 2). Lung cancer mortality rates started off higher in men but declined faster (p<0.001) to be similar to rates in women. Cardiovascular mortality declined at similar rates in men and women (p=0.804).
The absolute number of people with COPD dying of cardiovascular disease increased by 5% and the absolute number dying of lung cancer increased by 44% (figure 3). The increase in number of deaths due to lung cancer was more notable in women than in men.
Potential years of life lost
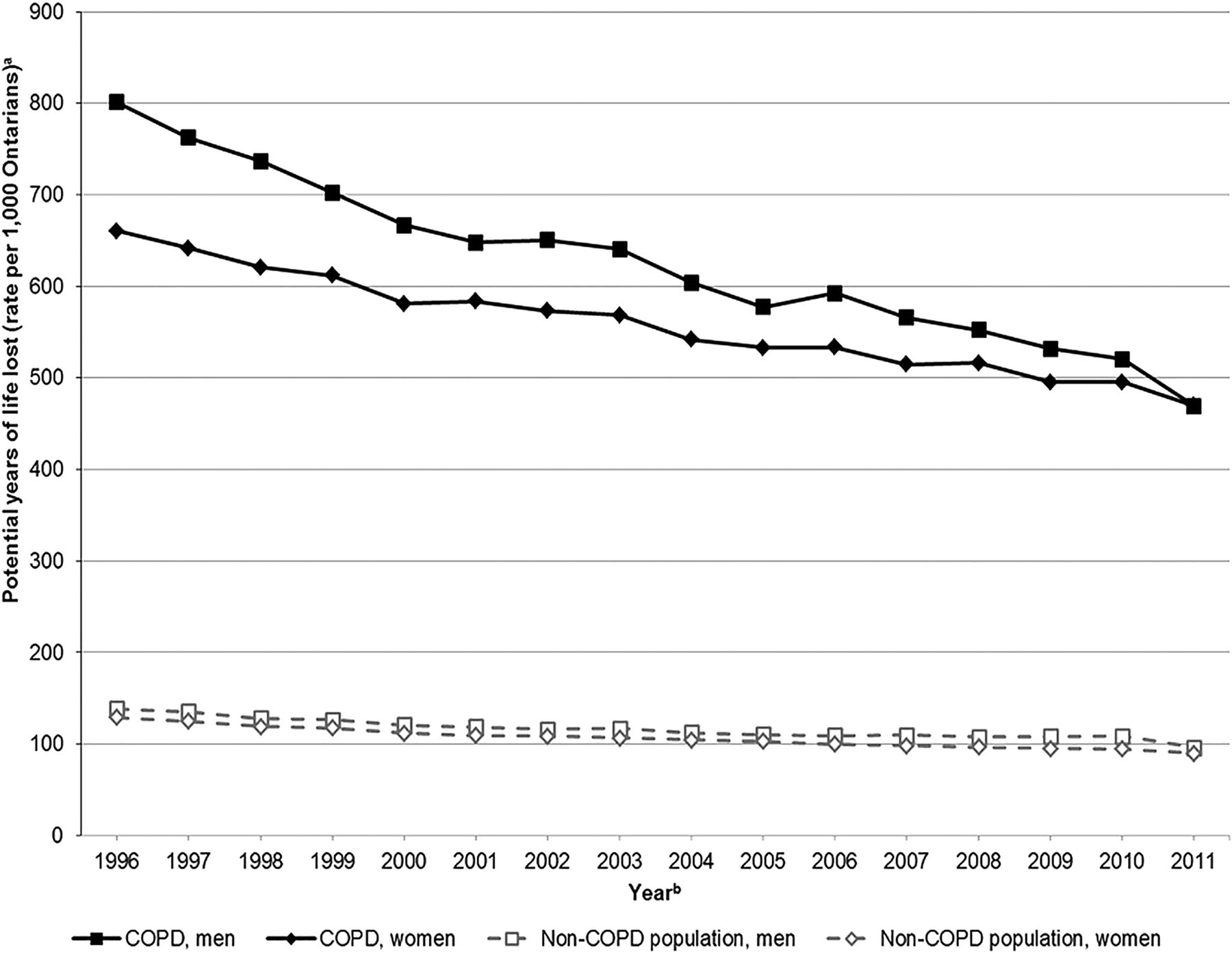
The rates of PYLL for men and women in the COPD population were more than five times the rates for men and women in the non-COPD population (figure 4). Rates in men started out higher than in women in 1996 and then declined faster so that rates between men and women were roughly equal in 2011.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rate of potential years of life lost per 1000 Ontarians with and without COPD from July 1996 to December 2011, stratified by sex. aPotential years of life lost was calculated using all-cause mortality and Ontario's mean life expectancy of 77.4 years for men and 82.0 years for women. bYears represent fiscal years, for example year 1996 represents 1 April 1996 to 31 March 1997.
Discussion
We conducted a comprehensive study of mortality trends in a large, complete real world COPD population and found that, relative to the non-COPD population, all-cause mortality decreased in men but not in women with COPD. We also found that all-cause, COPD-specific and lung cancer mortality rates, which started higher in men, decreased faster in men than in women becoming more similar over time. While such declines in mortality are encouraging and suggest that improvements in smoking rates and COPD management have led to better COPD health outcomes, the imbalance in improvements between sexes is concerning.
Our finding of a modest decrease in overall mortality is consistent with studies from other countries demonstrating decreasing COPD mortality trends as well.1 They also update our previous all-cause mortality findings.8 They expand upon these previous studies by comparing all-cause, COPD-specific, lung cancer and cardiovascular mortalities in men and women with COPD—thus offering a more complete understanding of mortality in this population.
The relative decrease in mortality observed in men but not in women with COPD compared with men and women, respectively, in the non-COPD population is consistent with lung cancer statistics16 and suggests that women are at higher risk of death from COPD and/or not benefiting as much from advancements in COPD care than men. It is notable that differences in declines in mortality between men and women exist despite similar decreases in smoking prevalence, and despite women smoking fewer cigarettes than men on average.17
The differences we observed between men and women, as mentioned, could be due to women being at higher risk of death from COPD or having different care. Compared with men, women with COPD appear to have earlier onset18 and a more rapid decline in lung function despite a lesser smoking history.19 ,20 Women have also been shown to have more small airway predominant pathology, increased hyperresponsiveness,21 and be more symptomatic than men.22 In terms of COPD care, primary care physicians have been shown to be significantly more likely to underdiagnose COPD in women than in men.22 ,23 More study is needed to determine how these factors impact risk of COPD, responses to management and mortality.
Greater declines in mortality in men than in women could also be because rates started higher in the former than the latter thus they had more to gain from advances in disease management. More study is needed to determine if the greater decline in men is due to this or other factors such as those described above. Of note, cardiovascular mortality also started off higher in men, meaning they also had more to gain in this area, however, their decrease in cardiovascular mortality was similar to women.
We found that improvements in all-cause mortality for people with COPD seemed largely driven by improvements in cardiovascular prognosis. While this is not unique to people with COPD,9 it is notable in this population with high cardiovascular comorbidity.4 ,5 ,24 At the same time, as lung obstruction is a risk factor for cardiovascular disease, improvements in COPD management might have played an even larger role in improving all-cause mortality in this group than is apparent.25 Overall, this complex interaction further suggests that improved all-cause mortality might be a better marker of overall health in people with COPD than COPD-specific mortality.
Improvements in COPD, cardiovascular disease and lung cancer age-standardised mortality rates, while encouraging, failed to reduce the absolute number of deaths due to these diseases which were still increasing—likely due to increasing population growth and aging. The minimal increase in absolute deaths caused by cardiovascular disease suggests improvements in its treatment over the years have had a large effect in stabilising the number of people with cardiovascular disease at the population level. In contrast, the large absolute increase in COPD deaths suggests this is not the case for COPD, and highlights the importance of continuing to search for better ways to improve health outcomes for people with this common disease.
Our study also found a decreasing trend of PYLL which appeared to outpace the decreasing trend of the non-COPD population. This finding is consistent with other studies and is likely due to the same factors that contributed to decreased mortality.26 Like with mortality, PYLL started off higher in men and decreases faster, becoming more similar to PYLL in women over time.
The strengths of our study were its ability to follow all individuals in Ontario, with and without COPD, longitudinally for many years and measure their all-cause and cause-specific mortality. It also had weaknesses which merit emphasis. First, its identification of individuals with COPD using a health administrative data case definition is subject to some misclassification. Nonetheless, we have no reason to believe such misclassification would change over time and affect trends in mortality. Second, cause of death depends on proper reporting to the medical examiner or coroner and previous studies have suggested that COPD is often underreported. This means that an individual with COPD that died of a cardiac arrest due to an exacerbation of their COPD is more likely to be classified as a cardiovascular death than a COPD death. When we included deaths due to COPD as coded by secondary diagnoses, we found that deaths due to COPD doubled (data not shown). This suggests that we might have underestimated the absolute number of people who died from COPD. Nonetheless, we have no reason to believe that such misclassification changed over time influencing trends. Such potential misclassification underscores the importance of considering all-cause mortality when describing mortality in people with COPD. Third, we did not have information on smoking or body mass index which influence mortality and comorbidities in COPD and would have been of interest to examine. Finally, we did not perform a competing risk analysis to determine how the different causes of death changed over time in comparison with each other. This would be an important area for future study.
Conclusions
We conducted a comprehensive study of mortality trends in a large, complete real world COPD population and found that all-cause, COPD-specific and lung cancer mortality rates, which started higher in men, decreased faster in men than in women, becoming more similar over time. Thus, while it appears that public health interventions and medical care are making a significant difference for individuals with this progressive, disabling disease, more study is needed to determine if they are benefiting both sexes equally.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All of the authors participated in the design, analysis and interpretation of the data and critical revision of the manuscript, and all approved the final version. Additionally, AG participated in the conception of the study, acquisition of data, supervision, drafting and obtaining funding. JH participated in the drafting and statistical analysis. AW participated in the statistical analysis. RW participated in the conception of the study. JCV and TT participated in the design, interpretation of the data and critically reviewed the manuscript. AD interpreted the data and critically reviewed the manuscript.
-
Funding Funding for this project was made available through the Government of Ontario who had no role in study design, collection, management, analysis, interpretation of data, writing of the report, or in the decision to submit the report for publication. This study was also supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or any of the funding agencies is intended or should be inferred. AG is currently supported by a Fellowship in Translational Research from The Physicians’ Services Incorporated Foundation, Toronto, Ontario, Canada and was supported by a New Investigator Award funded by team grant OTG-88591 from the Canadian Institutes of Health Research while working on this study. TT is supported by The Dales Award in Medical Research from the University of Toronto, Toronto, Ontario, Canada.
-
Competing Interests None.
-
Ethics approval Sunnybrook Health Sciences Centre Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.