Article Text

Abstract
Assessing alterations of the parenchymal architecture is essential in understanding fibrosing interstitial lung diseases. Here, we present a novel method to visualise fibrotic remodelling in human lungs and correlate morphological three-dimensional (3D) data with gene and protein expression in the very same sample. The key to our approach is a novel embedding resin that clears samples to full optical transparency and simultaneously allows 3D laser tomography and preparation of sections for histology, immunohistochemistry and RNA isolation. Correlating 3D laser tomography with molecular diagnostic techniques enables new insights into lung diseases. This approach has great potential to become an essential tool in pulmonary research.
- Interstitial Fibrosis
- Imaging/CT MRI etc
- Allergic Alveolitis
Statistics from Altmetric.com
“It takes more than cells to make a good lung”, as Weibel1 pointed out. The healthy lung is an efficient organ optimised towards a maximised surface and minimal diffusion barrier for gas exchange. The architecture that facilitates this organisation is based on thin elements of connective tissue providing stability and flexibility. Thus, understanding the three-dimensional (3D) architecture and parenchymal topography is essential to understanding lung function. This is not only true for the healthy lung, but even more so for pulmonary diseases where the 3D architecture is compromised, as, for example, in fibrosing interstitial lung diseases (ILD). Fibrotic changes are generally characterised by a spatially defined gain in tissue thickness due to accumulation of extracellular matrix, produced and modified by aggregates of activated myofibroblasts, as in ILD, for example, idiopathic pulmonary fibrosis or exogenous allergic alveolitis (EAA). Generally, the severity of disease is linked to the histopathological pattern and connectivity of fibrosis, which is responsible for the mechanical impairment of parenchymal dynamics.2 ,3 In samples from patients with ILD in areas appearing unaffected in high-resolution CT (HRCT), Coxson and coworkers observed a considerable increase in the thickness of parenchymatous tissue by means of design-based stereology.4 However, initial changes caused by the disease occur at a cellular level on a scale of microns, which cannot be depicted by HRCT scans and are therefore difficult to study in 3D, particularly in humans. Therefore, the goal of our study was to provide a method to visualise fibrotic remodelling of lung tissue in human lung biopsies and to demonstrate the correlation of morphological 3D data from individual fibrotic areas with gene expression analysis by miRNA or mRNA and immunohistochemistry.
Crucial for the analysis was the development of a novel embedding technique that combines different resins in order to clear the embedded samples to full optical transparency. With this novel technical approach the very same biopsy can be used for 3D tomography using scanning laser optical tomography (SLOT) and preparation of thin sections for histology, immunohistochemistry and RNA isolation after laser-assisted microdissection. Using SLOT the lung architecture can be visualised via endogenous absorption and fluorescence characteristics.5
Thereby, 3D imaging at a resolution of 10–12 µm was demonstrated in biopsies of a human lung explant from a patient suffering from end-stage EAA (figure 1). It was possible to identify areas of individual fibrotic remodelling and describe their morphological complexity through intensity, thickness and branching analysis based on absorption data sets. These 3D results of individual fibrotic areas were then correlated with conventional histopathology and gene expression profiles. Finally, virtual endoscopy based on the absorption data set from small bronchi via terminal bronchioles into the alveoli is feasible. For study details, see online supplementary material.
{kind=link}
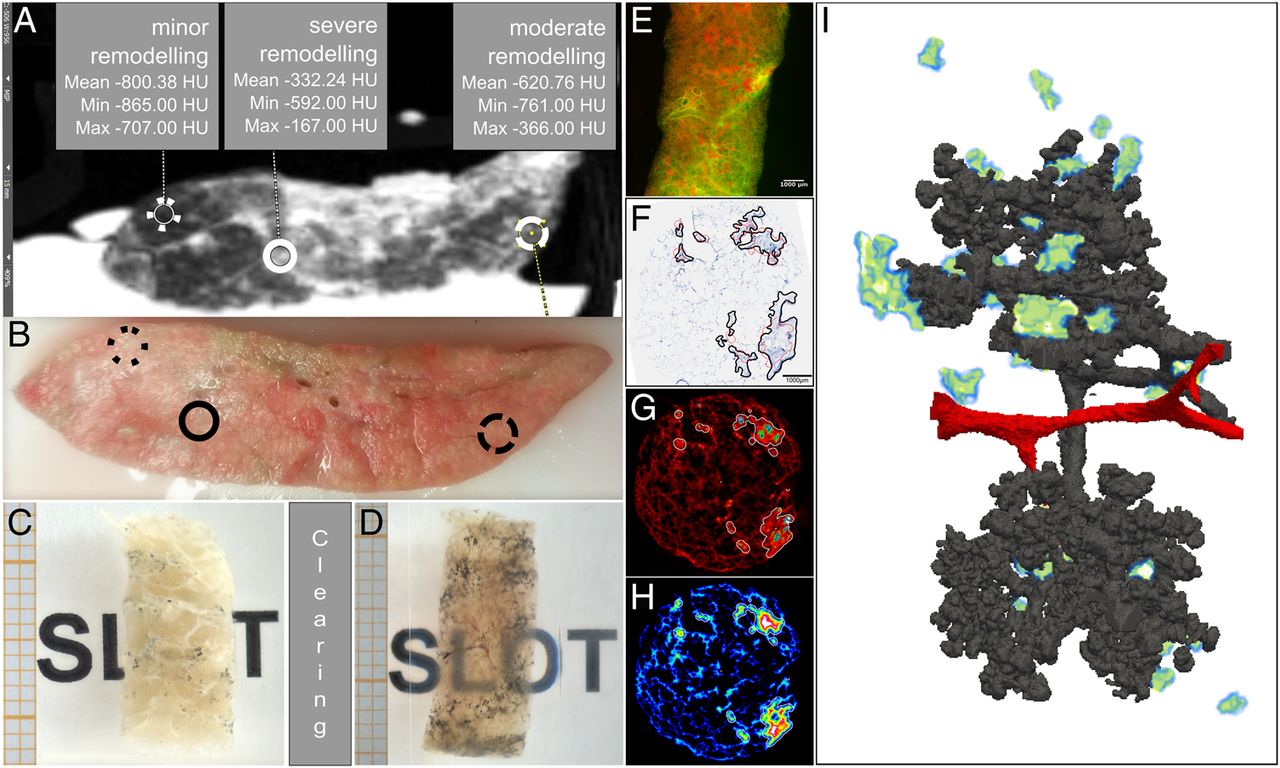
Analysis of the fibrotic architecture in human lungs. Via high-resolution CT scanning of a fresh explanted lung, grading of remodelling intensity was performed (A). Based on this grading, samples were taken at indicated sites and used for solid-block clearing (B). For this, extracted human lung biopsies were fixated (C) and cleared in the resin mixture (D). Scanning laser optical tomography (SLOT) scanning: 800 projection images were taken at a wavelength of 532 nm. (E) shows one of these images combining autofluorescence (green) and absorption (red) signals. Subsequently, histopathological evaluation of the same sample was performed (F) and areas of fibrotic remodelling (black lines) were compared with areas identified as pathological via thickness analysis (red lines represent areas exceeding 300 µm in diameter). The distance cut-off model was based on a thickness analysis of the SLOT data sets (G) and correlated well with an increased absorption of the tissue (H). Segmentation model of airways (grey) and blood vessels (red) in the same sample showing fibrotic areas identified by the distance cut-off model from (F) to (H) in the three-dimensional context (I). For a virtual bronchoscopy through this model, as well as movies of the SLOT projection data sets, distance analysis and the animated segmentation model, see online supplementary movies S1–4.
In summary, optically cleared biopsies from human lung explants can be used to visualise the lung architecture in health and disease. By correlating high-resolution 3D information with histology, immunohistochemistry, mRNA and miRNA expression analysis, new insights into the different stages of (fibrotic) human lung diseases are possible. This diagnostic approach has great potential to become an essential tool in lung research.
Acknowledgments
We would like to express our sincere gratitude to Susanne Kuhlmann and Regina Engelhardt for their excellent technical assistance, as well as Gareth Griffiths and Sheila Fryk for revising the text. Additionally, we would like to thank the developers and mailing list members of the open-source programmes Fiji (fiji.sc/Fiji), ITK-SNAP (itksnap.org/pmwiki/pmwiki.php), Paraview (paraview.org), ITK (itk.org), VTK (vtk.org), VMTK (vmtk.org), ImageMagick (imagemagick.org) and mencoder (mplayerhq.hu).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
- Data supplement 3 - Online video 1
- Data supplement 4 - Online video 2
- Data supplement 5 - Online video 3
- Data supplement 6 - Online video 4
Footnotes
Contributors MK and JW contributed equally to this study and share first authorship. DJ and MPK contributed equally to this study and share senior authorship. MK, JW, DJ and MPK conceived and designed research; MK, JW, GW, MH, NI and MPK performed experiments; MK, JW, JV-C, HM, TR, DJ and MPK analysed data; MK, JW, DJ and MPK interpreted results of experiments; MK, JW, RG and MPK prepared figures; MK and RG prepared movies; MK, JW, DJ and MPK drafted manuscript; MK, JW, GW, MH, NI, JV-C, R-AL, GA, SJ, RG, LK, TR, HM, HK, MO, DJ and MPK edited and revised manuscript; MK, JW, GW, MH, NI, JV-C, R-AL, GA, SJ, RG, LK, TR, HM, HK, MO, DJ and MPK approved final version of manuscript.
Funding The REBIRTH Cluster of Excellence, German Center for Lung Research (DZL) and a habilitation grant from TUI and DFG (grant 30743/1).
Competing interests MH, MK, MPK, R-AL, DJ, NI and HM are involved in a pending patent application for the sample preparation procedure (DE 102014108642.2). Parts of the SLOT imaging technique are patented by the Laser Zentrum Hannover e.V. and are invented by MH, R-AL and HM (among others).
Patient consent Obtained.
Ethics approval Ethikvotum-Nr. 2050-2013 by the ethics committee of the Medical School of Hannover.
Provenance and peer review Not commissioned; externally peer reviewed.