Article Text

Abstract
Background Several factors have been associated with mortality in the months after PE. Factors associated with short-term clinical deterioration or need for hospital-based intervention are less well known.
Methods We prospectively enrolled consecutive emergency department patients with PE and recorded clinical, biomarker and radiographic data. We assessed hospitalised patients daily to identify clinical deterioration or need for hospital-based intervention for 5 days after PE. We captured postdischarge events via 5-day and 30-day interviews. We used univariate and multivariable models to assess associations with clinical deterioration, severe clinical deterioration and 30-day all-cause mortality. We also assessed the test characteristics of three published clinical decision rules.
Results We enrolled 298 patients with PE: mean age 59 (SD±17) years; 152 (51%) male and 268 (90%) white race. 101 (34%) patients clinically deteriorated or required a hospital-based intervention within 5 days, and 197 (66%) did not. 27 (9%) patients suffered severe clinical deterioration and 12 died within 30 days. Factors independently associated with clinical deterioration were hypotension (p=0.001), hypoxia (p<0.001), coronary disease (p=0.004), residual deep vein thrombosis (p=0.006) and right heart strain on echocardiogram (p<0.001). In contrast, factors associated with 30-day all-cause mortality were active malignancy (p<0.001) and congestive heart failure (p=0.009). The sensitivity of clinical decision rules was moderate (39–80%) for 5-day clinical deterioration but higher (67–100%) for 30-day mortality.
Conclusions Most patients do not clinically deteriorate after PE diagnosis. Several factors are associated with short-term clinical deterioration, but these factors differ from those associated with 30-day mortality.
Statistics from Altmetric.com
Key messages
What is the key question?
-
How many patients with PE clinically deteriorate or otherwise need hospitalisation immediately after their diagnosis, and can we identify these patients?
What is the bottom line?
-
Most patients with PE do not clinically deteriorate or require a hospital-based intervention after their diagnosis, and while several factors are associated with clinical deterioration, existing clinical prediction rules have limited accuracy.
Why read on?
-
By following patients every day for 5 days after their PE, this study provides highly granular data on outcomes related to PE occurring during the time patients are usually in the hospital.
Introduction
Outcomes after pulmonary embolism (PE) vary widely. For some patients, PE causes rapid hemodynamic collapse, whereas for others, PE is clinically inconsequential. Identifying patients at risk for short-term clinical deterioration is important and challenging. Increasingly, physicians must determine which patients with PE should be admitted to a hospital floor or an intensive care setting and which patients are safe for discharge from the emergency department (ED).
Several factors are associated with mortality and recurrence in the months after PE, and clinical decision rules (CDRs) have been developed to quantify these risks.1–12 Validation studies and a large clinical trial of outpatient PE treatment have demonstrated a low incidence of death or recurrent PE within 30–90 days in patients with low CDR scores.1 ,8 ,10 ,11 ,13–18 However, these outcomes may not adequately inform the decision to admit or discharge a patient from the ED. A typical hospitalisation for PE lasts 3–5 days. Clinicians consider events during this timeframe more important to the disposition decision than events occurring after a patient would be discharged from the hospital.19 ,20 Also, mortality after PE is frequently due to underlying illness.15 ,18 ,19 The inclusion of ‘host factors’ like malignancy and cardiopulmonary disease in CDRs may inflate their association with all-cause mortality.
Identifying factors associated with patient-oriented outcomes occurring during a typical PE hospitalisation may help clinicians decide which patients benefit from inpatient admission. We therefore performed this study with three goals in mind: (A) to determine the incidence of clinical deterioration or the need for hospital-based intervention occurring during a typical hospitalisation for PE; (B) to identify factors associated with these events, and (C) to determine whether CDRs identify patients at risk for these events. To the authors’ knowledge, this is the first prospective study of factors associated with a wide spectrum of clinical events, occurring in the timeframe of a typical hospitalisation for PE.
Methods
Design
We performed a prospective non-interventional study of consecutive adult ED patients diagnosed with PE between October 2008 and December 2011 in accordance with standards for the reporting of observational studies (STROBE) and best practices.21 The study was approved by the Human Research Committee of Partners HealthCare (2008-P-002001). All patients provided written informed consent.
Setting
Massachusetts General Hospital is an urban, university hospital with an annual ED volume of 95 000 patient visits.
Subject eligibility and enrolment
We used a combination of active screening and review of radiologic tests to identify patients eligible for enrolment, which allowed us to enrol consecutive patients 6 days a week (except Saturday). We enrolled adult (age >17 years) patients diagnosed with radiographically proven PE in the ED. Radiographically proven PE was defined as (A) a filling defect in a pulmonary artery on computed tomography pulmonary angiogram (CTPA); (B) a high-probability ventilation/perfusion scan and (C) a positive leg ultrasound or CT venogram performed to diagnose PE (not isolated deep vein thrombosis (DVT)), confirmed by the treating clinician. PE diagnoses were based on the interpretation of board-certified radiologists not affiliated with the study. CTPA were re-read by two board-certified radiologists affiliated with the study to confirm and quantify PE.
Patients were eligible if PE was diagnosed within 24 h of ED registration. Patients transferred from outside EDs or clinics with a diagnosis of PE were eligible until 24 h after confirmatory imaging. Patients with PE found incidentally (ie, without clinical suspicion) were eligible. Patients were excluded if they were <18 years old, could not provide informed consent or were unable to follow-up. Patients diagnosed with PE >24 h after ED registration were excluded.
Data collection and follow-up
After enrolment, outcomes associated with PE were identified prospectively. Study staff interviewed each patient, their nurses and reviewed the medical record every day for 5 days to identify clinical deterioration events. Five days is consistent with the median length of stay for PE in our institution as well as the timeframe cited as most relevant to the disposition of a patient with PE in a survey of clinicians.20 ,22 ,23
We performed postdischarge follow-up using a validated combination of telephone calls and electronic medical record review.24 On days 5 and 30, we called discharged patients to ask whether they had returned to an ED or clinic for any unscheduled visits and whether a visit was related to recurrent PE or bleeding.
Independent variables
At the time of enrolment, we recorded clinical factors including demographics, ED vital signs and comorbid illness via direct patient interview and confirmed these by review of each patient's electronic medical history/problem list (see online supplement for detailed variable definitions). Discrepancies were adjudicated by two study investigators (CK, IO or PH), with ties broken by a third investigator. To standardise data collection and reduce confounding while capturing results potentially available to an emergency physician, we chose a priori to record radiological, echocardiographic and biomarker results that were available within 24 h of PE diagnosis. Radiological studies and biomarkers were performed at the discretion of the treating physician. However, we also collected blood samples at the time of enrolment and used these to complete biomarker analyses when necessary.
We gathered data required to calculate three published CDRs: the pulmonary embolism severity index (PESI),8 the simplified PESI (sPESI),12 and the Geneva Prognostic Rule.3 As arterial blood gasses are not routinely performed after PE in our institution, we modified the Geneva Prognostic Rule by substituting oxygen saturation (Sa02) <90% measured by pulse oximetry for partial pressure of oxygen in arterial blood (PaO2) <8 kPa.3 ,5
Outcomes
Outcome events were collected after patients were discharged from the ED to the inpatient setting or home. Our primary outcome was designed to include a wide spectrum of clinical deterioration events and interventions that typically require hospitalisation (table 1). We also assessed severe clinical deterioration, defined as an inherently unstable condition or advanced intervention/therapy. Lastly, we assessed all-cause 30-day mortality to facilitate comparison with previous studies. We felt that the variables associated with events secondary to PE were likely to be different than the variables associated with events secondary to treatment, so we did not include bleeding in our primary outcome but did include it in a secondary analysis.
Outcome definitions
Statistical analysis
Demographics were summarised using mean and SD for continuous variables and percentages for categorical variables. We performed χ2 tests to identify univariate associations and multivariable logistic regression to identify factors independently associated with clinical deterioration, severe deterioration and 30-day mortality. Univariate analysis was performed on all variables potentially clinically related to adverse outcomes after PE and variables with p values <0.2 were considered potential predictors for the models. Final models included variables significant at the 0.05 level. Threshold values for continuous measures were based on previous PE literature or, when no accepted threshold was available in the literature (eg, N-terminal brain natriuretic peptide (NT-proBNP)), from exploratory data analysis for choosing optimal cutpoints.
Based on published studies, we defined low risk as PESI categories I–II, sPESI <1 point and Geneva Prognostic Rule ≤2 points.3 ,9 ,10 ,12 For each CDR, we performed receiver operating characteristic (ROC) curve analysis, calculated sensitivity, specificity, positive (PPV) and negative predictive value (NPV), and positive/negative likelihood ratios with 95% CIs. PPV and NPV were calculated based on the outcome prevalence in our study sample. We performed a subanalysis of CDR performance excluding patients with a shock index (pulse rate/systolic blood pressure) ≥1 in the ED. All analyses were done using SAS V.9.3 (The SAS Institute, Inc., Cary, North Carolina, USA). Two-sided p<0.05 was considered as statistical significance.
Results
We identified 403 patients with PE in the ED and enrolled 301 (figure 1). After enrolment, three patients were deemed ineligible: two because PE was diagnosed >24 h before enrolment, and one because the CTPA was re-read as tumour, not PE. We included 298 patients in our final analysis.
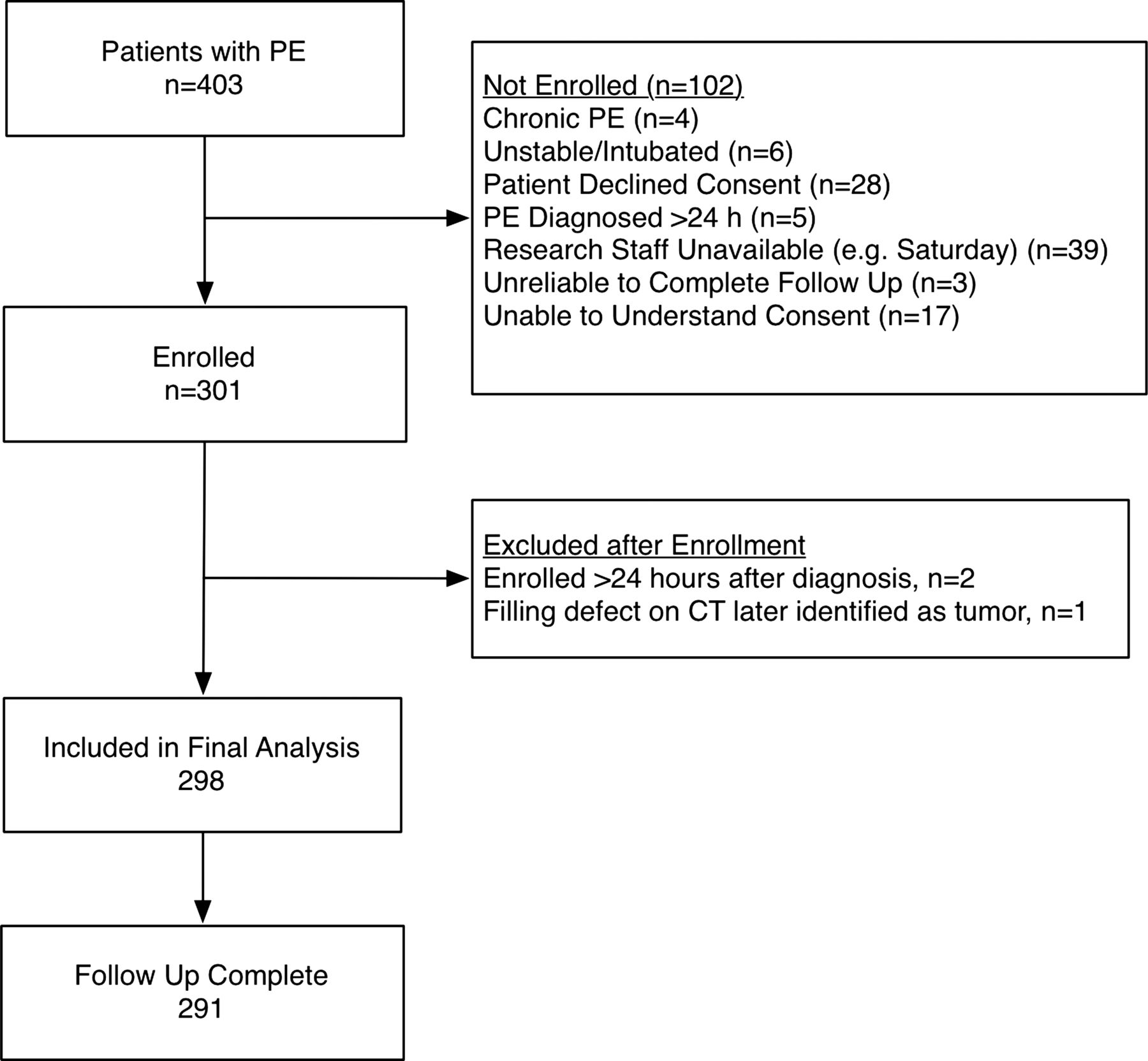
{kind=link}
Eligible and enrolled patients.
Demographics and comorbidities are presented in table 2. Diagnostic testing included CTPA (288/298, 96.6%), V/Q (5/298, 1.7%), lower extremity ultrasound (99/298, 33.2%), CT venography (136/298, 45.6%), echocardiography (66/298, 22.1%), troponin (289/298, 97.0%), NT-proBNP (270/298, 90.6%) and D-dimer (272/298, 91.3%). Most patients (250, 84%) were admitted to hospital floors, with 24 (8%) admitted to intensive care units and 23 (8%) to an ED observation unit. PE was diagnosed prior to admission to an ED observation unit in 21/23 (91%). The median hospital length of stay was 3 days (25–75%, 1–5 days) with 87 (29%) patients in the hospital on day 5. Thirty-day follow-up was successful for 291 (98%) patients. Of the seven patients without follow-up, six had data in our medical record confirming they were alive 30 days after enrolment.
Demographics of analysed patients
With regards to our primary outcome, 101 (34%) patients clinically deteriorated or required a hospital-based intervention within 5 days of PE, whereas 197 (66%) did not (table 3). Several patients were classified as having clinical deteriorated based on more than one criterion. The most common clinical deterioration events were hypoxaemia/need for respiratory support and hypotension.
Adverse clinical events occurring within 5 days of PE diagnosis
Twenty-seven (9%) patients suffered a severe clinical deterioration or required a major intervention within 5 days of PE diagnosis, including positive pressure ventilation/endotracheal intubation (n=18 [6%]); ventricular tachycardia/fibrillation (n=2 [0.7%]), vasopressor therapy (n=1 [0.3%]), thrombolysis/thrombectomy (n=10 [3%]) and death (n=1 [0.3%]).
Seven (2%) patients developed bleeding related to anticoagulation within 5 days of PE diagnosis, including gastrointestinal (n=2, 29%), intracranial (n=1, 14%), other bleeding requiring transfusion (n=1, 14%) and 3 (43%) patients sought care for bleeding after discharge, though the location of this bleeding was not confirmed.
Within 30 days, 12 (4%) patients died, 10 from end-stage malignancy with no evidence that PE hastened death and 2 from end-stage interstitial pulmonary fibrosis.
Factors associated with clinical deterioration
Factors associated with our outcomes on univariate analysis are highlighted in table 4. Among the 101 patients with our primary outcome, echocardiography or lower extremity ultrasound identified two who had normal values for biomarkers, oximetry and vital signs. On multivariable analysis, factors independently associated with our primary outcome were lowest systolic blood pressure in the ED <90 mm Hg (OR=6.9 (95% CI 2.2 to 21.9), p=0.001), lowest oxygen saturation in the ED <95% (OR=3.6 (95% CI 2.0 to 6.2), p<0.001), history of coronary artery disease (OR=3.8 (95% CI 1.5 to 9.6), p=0.004), residual DVT (OR=2.4 (95% CI 1.3 to 4.4), p=0.006) and right heart strain on echocardiogram (OR=3.4 (95% CI 1.7 to 6.9), p<0.001). We also ran our model excluding right heart strain on echocardiogram, and results were similar (data not shown).
Univariate associations with clinical deterioration or need for hospital-based intervention within 5 days of PE diagnosis
Factors associated with severe outcomes were systolic blood pressure <90 mm Hg in the ED (OR=4.2 (95% CI 1.3 to 13.1), p=0.015), elevated NT-proBNP (OR=3.4 (95% CI 1.1 to 10.1), p=0.027) and right heart strain on echocardiogram (OR=5.6 (95% CI 2.2 to 13.9), p<0.001). Removing right heart strain on echocardiogram from the model, systolic blood pressure <90 mm Hg in the ED (OR=4.6 (95% CI 1.5 to 14.0), p=0.008), elevated NT-proBNP (OR=5.7 (95% CI 2.0 to 16.0), p<0.001) and PE in a central location (OR=3.6 (95% CI 1.4 to 9.1), p=0.008) were associated with severe outcomes.
Factors associated with 30-day all-cause mortality were active malignancy (OR 24.2 (95% CI 5.0 to 116.6), p<0.001) and history of congestive heart failure (OR 16.8 (95% CI 2.0 to 139.3), p=0.009). Right heart strain on echocardiogram was not associated with 30-day all-cause mortality.
Including major bleeding events (in hospital or on follow-up) in our primary outcome did not change our results as all patients with bleeding met at least one other outcome criteria (data not shown).
Analysis of CDRs
The sensitivity all CDRs was moderate, with the PESI and sPESI being more sensitive (71% and 80%, respectively) and the Geneva Prognostic Rule being more specific (84%) for our primary outcome (table 5). Areas under the ROC curve (AUC) for the primary outcome were PESI=0.69, sPESI=0.69 and Geneva Prognostic Rule=0.65. By comparison, the model using our predictor variables had an AUC of 0.77 for our primary outcome, and our predictive model had a sensitivity of 86% and a NPV of 88% using a predictive probability of 0.14 as the cut-off. For severe outcomes, the AUC were PESI=0.68, sPESI=0.67 and Geneva Prognostic Rule=0.61. For 30-day all-cause mortality, the AUC were PESI=0.84, sPESI=0.82 and Geneva Prognostic Rule=0.78. By comparison, our model using systolic blood pressure <90 mm Hg in the ED, elevated NT-proBNP and right heart strain on echocardiogram had an AUC of 0.83, and the model had a sensitivity of 93% and a NPV of 99% using a predictive probability of 0.06 as the cut-off.
Test characteristics of clinical decision rules
We performed a secondary analysis, adjusting our definition of low risk to include PESI category I only. Test characteristics for our primary outcome were sensitivity 85% (95% CI 77% to 91%), specificity 37% (95% CI 30% to 44%), PPV 41% (95% CI 34% to 48%) and NPV 83% (95% CI 73% to 90%).
In the subanalysis of patients with a shock index <1 (n=233) in the ED, sensitivity and NPV were lower for all CDRs. Results were similar for severe outcomes (data not shown).
Discussion
The ability to assess patients’ risk of short-term clinical deterioration after PE has gained importance in recent years. Low-risk patients may be eligible for outpatient treatment with heparin or novel oral anticoagulants. 15 ,25 Meta-analyses, systematic reviews and a large clinical trial support the safety of this approach.15 ,26 ,27 Piran et al26 found that selected patients with PE treated as outpatients had low rates of recurrent venous thromboembolism (VTE) (1.47%), fatal PE (0.47%) and major bleeding (0.81%), and Vinson et al28 found that outpatient treatment was associated with low 90-day VTE-related mortality. Conversely, high-risk patients with PE may benefit from intravenous or catheter-directed thrombolysis. Determining whether outpatient treatment or aggressive intervention is appropriate for a patient with PE is now a critical decision in emergency medicine.
In this study, we provide detailed prospective data on the incidence of clinical deterioration and the need for hospital-based interventions related to PE, occurring shortly after diagnosis. Our primary outcome was broad-based and designed to capture the spectrum of events that might justify hospitalisation. Unlike prior studies, we only studied outcomes occurring during a typical inpatient admission. Even with our broad definition, we found that most patients (66%) suffer no clinical deterioration and require no hospital-based intervention within 5 days of PE diagnosis. Our results are consistent with previous work and suggest that many patients with PE may not benefit from inpatient hospitalisation.2 ,15 ,22
We identified several factors associated with clinical deterioration after PE, including abnormal vital signs, the presence of right heart strain on echocardiogram, residual DVT and elevated biomarkers. These factors have face validity and have been shown to be associated with clinical deterioration in previous studies.9 ,10 ,12 ,13 ,29–34 Coronary artery disease, which was also associated with our primary outcome, may make patients less able to withstand increased pulmonary artery pressure. This will require further exploration.
Interestingly, we found that factors associated with 5-day clinical deterioration were generally different than factors associated with 30-day all-cause mortality. This finding was true on univariate and multivariable analysis, and for our primary and severe outcomes. Factors associated with 30-day all-cause mortality included malignancy and a history of congestive heart failure, suggesting that 30-day mortality is often related to pre-existing illness, rather than the acute PE. While we acknowledge that pre-existing illness is important to consider, future studies should emphasise outcomes directly related to the PE.
We found published CDRs to be moderately sensitive for our outcomes, but highly sensitive for 30-day mortality. This may be explained by the fact that the CDRs we examined all include malignancy; the cause of death for 10/12 (83%) patients in our study. The PESI and sPESI also include chronic cardiopulmonary disease, which was the cause of death for the remaining two patients.
Limitations
We used complimentary methods to achieve consecutive enrolment, but when we reviewed radiology records to identify patients diagnosed with PE at night, we could not confirm that an ultrasound was performed in a patient suspected of having PE. We may therefore have missed some patients diagnosed by ultrasound alone. Only five (2%) enrolled patients were diagnosed by ultrasound alone so we suspect few patients were missed. Informed consent was required, so we could not enrol patients with severely altered mental status, significant hemodynamic instability or endotracheal intubation. Although a substantial number (n=65 (21%)) of enrolled patients had a shock index ≥1, our sample may under-represent severe PE.
To standardise the collection of data, we included test results obtained within 24 h of PE diagnosis and defined these as being ‘available to the emergency physician’. We felt limiting our predictive data to results actually obtained in the ED would introduce unacceptable variability unrelated to the safety of outpatient PE treatment. By including data obtained up to 24 h after PE diagnosis, our results may also be applicable to an ED/observation unit stay. However, with the exception of echocardiography, the tests we analysed are rapidly available in most EDs. We therefore believe our results are directly relevant to ED decision making.
We followed patients for clinical deterioration occurring in the hospital and on telephone follow-up, but as some events are more likely to be recognised and reported by patients, we may have missed some clinical deterioration events occurring after discharge. Our 5-day outcomes are different than those for which CDRs were derived, and this likely affected their test characteristics. However, we feel our outcome is directly relevant to the decision to admit or discharge a patient from the ED.
We did not include in our analysis social factors or concurrent illness that might limit the practicality of outpatient treatment, as has been done in other studies.28 ,35 ,36 Finally, while our study suggests that a large proportion of patients might not require hospitalisation, we did not directly assess the safety of outpatient treatment in this study. A management study based on short-term, patient-centred outcomes would be beneficial.
Conclusions
Most (66%) patients suffer no clinical deterioration and require no hospital-based intervention in the first five days after PE. The outpatient treatment of PE is likely safe for a large proportion of patients. Abnormal vital signs, imaging findings and elevated biomarkers are associated with short-term clinical deterioration related to PE. However, existing CDRs are only moderately sensitive for this outcome. Future research focusing on outcomes directly related to PE is needed to facilitate safe outpatient treatment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
International Society of Thrombosis and Hemostasis, Amsterdam, 2013, Society of Academic Emergency Medicine, Denver, CO 2012.
-
Collaborators Parry, Blair A.
-
Contributors CK: conceived the study, obtained funding, collected and analysed data, drafted and edited the manuscript. IO and PH conceived the study, collected data and edited the manuscript. JKT obtained funding, analysed the data and edited the manuscript. PM and FH collected and analysed data, drafted and edited the manuscript. YC analysed data and edited the manuscript.
-
Funding This work was funded by a grant from the Harvard Milton Fund. The funding agency had no role in the design of the study, analysis or writing the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Human Research Committee, Partners HealthCare.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Requests to collaborate and use data published here will be considered. Data referenced, but not shown will be provided upon request.