Article Text

Abstract
Background COPD is an inflammatory disease usually associated with cigarette smoking (CS) with an increasing global prevalence and no effective medication. Extracellular ATP is increased in the COPD affected lung and may play a key role in driving CS-induced airway inflammation, but the mechanism involved in ATP release has eluded researchers. Recently, the transient receptor potential (TRP) and pannexin-1 channels have been suggested to play a role in other experimental paradigms. Thus, the aim of this work is to investigate if these channels are involved in CS-induced ATP release in the lung.
Methods Primary human cells were exposed to CS and extracellular ATP levels measured. Mice were exposed to mainstream CS and airway inflammation assessed. TRPV1/4 mRNA expression was assessed in human lung parenchyma.
Results CS exposure caused a dose-related increase in ATP from primary airway bronchial epithelial cells. This was attenuated by blockers of TRPV1, TRPV4 and pannexin-1 channels. Parallel data was obtained using murine acute CS-driven model systems. Finally, TRPV1/4 mRNA expression was increased in lung tissue samples from patients with COPD.
Conclusions Extracellular ATP is increased in the COPD affected lung and may play a key role in driving disease pathophysiology. These experiments uncover a novel mechanism which may be responsible for CS-induced ATP release. These findings highlight novel targets that could lead to the development of medicine to treat this devastating disease.
- COPD Pathology
- COPD Pharmacology
Statistics from Altmetric.com
Key messages
What is the key question?
COPD is an airway disease with an increasing global prevalence but no effective medication. Understanding the disease pathogenesis would be a major step towards developing new therapies.
What is the bottom line?
This study reveals for the first time the mechanism that leads to the increased ATP levels and the associated steroid-resistant inflammation observed in the airways of patients with COPD.
Why read on?
These data highlight novel targets which can be exploited for the development of effective therapeutics for the treatment of COPD.
Introduction
COPD is an inflammatory airway disease usually associated with cigarette smoking (CS) with an increasing global prevalence and no effective medication.1–3 The Global Initiative for Chronic Obstructive Lung Disease guidelines state that COPD is characterised by airflow limitation that is not fully reversible and is attributed to small airways disease and parenchymal destruction. It is a steroid-resistant, inflammatory disease characterised by the infiltration of leucocytes including neutrophils, macrophages and CD8+ T-cells.4 ,5 Increased concentrations of many proinflammatory mediators are also observed including the caspase-1 related cytokines, IL-1β and IL-18, the levels of which are found to correlate with disease severity.6 ,7 Caspase-1 activation is thought to be regulated by the NLRP3 inflammasome, and one of the key activation mechanisms is through extracellular ATP (eATP)-dependent stimulation of the P2X7 receptor.8–10 Interestingly, increased levels of eATP have been reported in vitro and in vivo models of cigarette smoke-induced inflammation and in the lungs of patients with COPD.11–14 The relevance of this pathway to the pathogenesis of COPD is supported by findings that P2X7 receptor and caspase-1 activation are central to the development of CS-induced airway inflammation in murine models.15–17
eATP is thought to be stored in the cytosol, but the mechanism by which it is released can depend on the cell/tissue type, the environment and the stimulus.18–21 Recent evidence has suggested a role for the pannexin-1 channel/pore in the mechanism of ATP release.22–27 Furthermore, transient receptor potential (TRP) channels have been suggested to play a pivotal role in the release of eATP and are associated with opening the pannexin-1 channel.18 ,27 ,28 Of the TRP family, TRPV4 has been shown to be present in the airway and involved in the release of hypotonicity-induced eATP.27 ,29 ,30 Endogenous TRPV1 activators (e.g. lipoxygenase products and mediators of the Protein Kinase-A, Protein Kinase-C and Phospholipase- C pathways) are known to be increased in the COPD affected lung. Furthermore, low pH conditions often manifest in the lungs of patients with COPD as measured in exhaled breath condensate and this is also a trigger for TRPV1 activation.31 TRPA1, has also been implicated in COPD-associated disease pathologies. Indeed, Trpa1−/− mice were found to be protected against CS-mediated plasma protein extravasation and had reduced levels of the murine neutrophil chemoattractant keratinocyte chemoattractant (KC).32 Furthermore, TRPA1 is known to be activated by some of the key inflammatory components of CS, including acrolein and crotonaldehyde.33
Therefore, in view of the evidence presented above, we hypothesised that CS exposure induces ATP release via activation of specific TRP channels and the subsequent opening of the pannexin-1 pore. To test this hypothesis, we confirmed that CS exposure increased ATP levels in lavage in a murine model and that these levels were unchanged in P2X7 receptor-deficient mice that were protected from the CS-induced neutrophilia. This suggested that in our system the P2X7 receptor was not involved in the eATP release and that the signal was not from the recruited neutrophils but probably from cells present in the airway i.e. alveolar macrophages (AM) and human bronchial epithelial cells (HBEC). To study the mechanism responsible for the CS-induced release of ATP, we used primary human cell-based assays (AMs and HBECs) and pharmacological tools to investigate the role of TRPV1, TRPV4 and TRPA1 and pannexin-1. This was paralleled in our murine model using Trpv1, Trpv4, Trpa1 and pannexin-1 gene knockout (KO) mice. Finally, we measured the expression of the TRP channels in disease-relevant lung tissue harvested from patients with COPD to provide convincing data implicating these ion channels in the pathophysiology of COPD and highlighting them as novel targets for therapeutic intervention.
Materials and methods
Cell-based model system
CS bubbled medium (CSM) was prepared as described previously34 and added to HBECs (Lonza, UK) or human AMs harvested as previously described.34 Cell viability was assessed using MTT. ATP levels were assessed using an ATPlite assay (Perkin Elmer, Cambridge, UK). Osmolarity and pH was assessed using an Osmomat 030 osmometer (Gonotec, Germany) and pHep4pH meter (Hanna Instruments, UK), respectively. In some experiments, cells were pretreated with TRPV1, TRPV4 or TRPA1 antagonists (JNJ-17203212 (Sigma, UK), HC 067047 (Peakdale Molecular, UK) and HC 030031 (Chembridge, USA)), respectively, or agonists capsaicin (Sigma, UK), GSK 1016790a (Sigma, UK) and acrolein (Sigma, UK), respectively. In separate experiments cells were pretreated with specific pannexin antagonists carbenoxolone and probenecid or the connexin inhibitor flufenamic acid (all from Sigma, UK). Concentrations used were based on previous studies.24 ,27 ,35
Measurement of mRNA expression
Quantitative RT-PCR was used to measure mRNA from human lung samples and cell populations using TaqMan reagents and protocols (Applied Biosystems) as previously described.36 Human donor and recipient lung tissue samples, surplus to clinical requirements, were obtained from a transplant programme supported by the NIHR Respiratory Disease Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London. Informed written consent and ethical approval was obtained (Ethic Number: REC 09/H0708/72, active from Dec 2009). See table 1 for demographic details.
Details on the donor/recipient
In vivo studies
All in vivo protocols were approved by a local ethical review process and strictly adhered to the Animals (Scientific Procedures) Act 1986 UK Home Office guidelines (Project Licence number: 70/7212, active from May 2012). Male wild-type C57BL/6 were bred inhouse alongside the genetic lines. Mice were either kind gifts or purchased from Jackson labs, USA, (P2X7—Professor Jean Kanellopoulos (Université Paris-Sud, France), Trpv1 and Trpa1—Jackson labs; Trpv4—Riken Bioresource Centre, (Japan)37 ,38 and Pannexin-1—Dr Vishva Dixit, (Genentech, USA)).
CS or lipopolysaccharide (LPS) exposure protocols have been described previously.15 Briefly, mice were exposed to CS (1 h, twice a day for 3 days—acute model) or LPS (aerosol of 1 mg/mL for 30 min) and the lungs lavaged 24 h or 6 h later, respectively. Bronchoalveolar lavage fluid (BALF) interleukin (IL)-1β (ELISA, assay range reported as 15.6–1000 pg/mL; to measure lower levels it is important to freshly prepare the assay plates) neutrophil and ATP levels (no increase detected in the LPS model) were assessed as previously described.15 A parallel subchronic model was also performed where the wild-type or KO mice were exposed to CS for 14 days.
Data analysis
Data are expressed as mean±SEM of n observations. Statistical significance was determined using either single or multiple comparisons (specific tests used are described in the figure legends), using GraphPad Prism 5 software. A p value <0.05 was taken as significant and all treatments were compared with the appropriate control group.
Online supplementary material
The online supplementary material section contains the data from characterising the impact of smoke on cell/medium in vitro, profiling the TRPV1, TRPV4 and pannexin-1 KO mice in the LPS-driven model of airway inflammation. Additionally, it contains the data from profiling the TRPA1 KO mice in the smoke and LPS model systems.
Results
P2X7 receptor and neutrophils are not involved in acute CS mediated ATP release in vivo
Wild-type and P2X7−/− mice were concurrently exposed to CS twice a day for three consecutive days. There was a significant increase in ATP, IL-1β and neutrophils in the BALF in CS-challenged wild-type mice 24 h after the last exposure (figure 1). P2X7−/− mice exhibited significantly reduced levels of IL-1β and neutrophilia compared with the wild-type consistent with previously published data15 ,16 (figures 1B, C). There was, however, no reduction in the levels of BALF ATP in CS-exposed P2X7−/− mice compared with the wild-type controls. This indicates that the ATP release is independent of the P2X7 receptor and that it is not released from the recruited neutrophils. This also suggests that CS-induced ATP is upstream of the P2X7-inflammasome-IL-1β/IL-18 axis and is released from structural and/or resident cells in the airway, possibly AMs and bronchiolar epithelial cells.
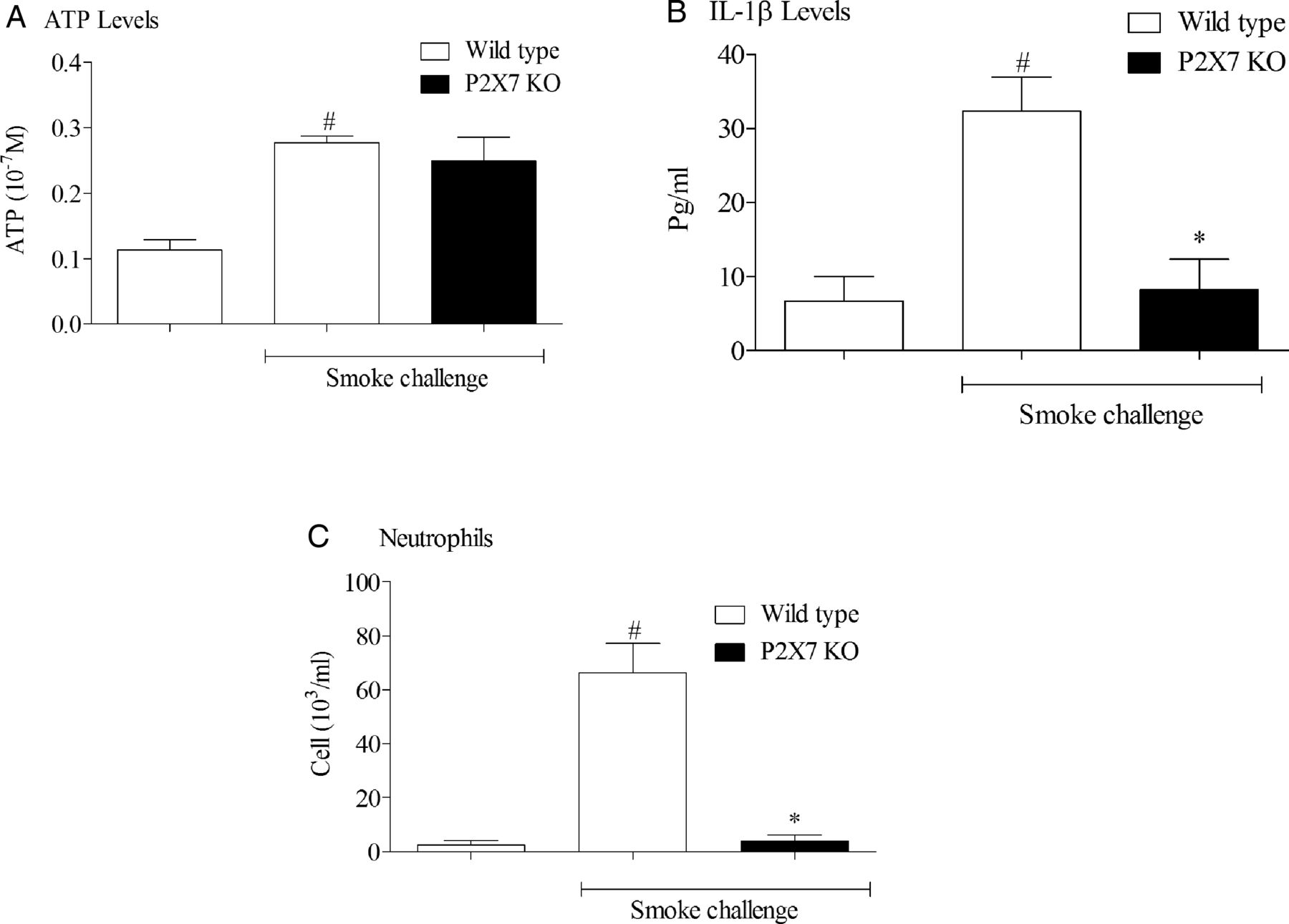
The role of P2X7 in cigarette smoking (CS)-induced murine airway inflammation. P2X7−/− mice were exposed to CS or room air (control) twice daily for 3 consecutive days alongside wild-type controls. Bronchoalveolar lavage fluid was collected 24 h after the last exposure for measurement of neutrophil (C), interleukin (IL)-1β (B) and ATP (A) levels. Data are represented as mean±SEM for n=8 animals in each group. Statistical significance was determined using Mann–Whitney U test. #p<0.05, denoting a significant difference between the smoke-exposed and air-exposed wild-type groups; *p<0.05, denoting a significant difference between the smoke-exposed knock-outs (KO) and wild-types.
Development and characterisation of CS-induced ATP release in vitro
To begin to investigate the mechanism responsible for CS-induced ATP release we used cell-based assays. We selected airway-relevant primary cells (HBECs and AMs) and exposed them to CSM. CSM caused a dose-related release of ATP over time in both cell types (figure 2A, C). CSM (2.5%) was chosen for further analysis. CSM did not cause any cell death or alter the pH or osmolarity of the culture medium (see online supplementary figure S1). Analysis of the mRNA levels of the TRP channels under investigation in the two cell types showed that both cell types expressed significant levels of TRPV1 and TRPV4 mRNA but the levels of TRPA1 were below the detection limit of the assay in AMs and detected only at very low levels in HBECs (figure 2D).

Characterisation of ATP release from HBECs and AMs in vitro. For concentration-response experiments (A and C), HBECs and AMs were stimulated with increasing concentrations (0.312%–10%) of CSM or vehicle (normal medium). Cells were incubated for 3 h before removal of supernatant and measurement of ATP levels. For time-course experiments (B and C), cells were stimulated with CSM (2.5/5%) or vehicle. Supernatants were removed from selected cell populations at various time-points (1, 3, 6, 24 h) after stimulation for measurement of ATP. For both, concentration-response and time-course experiments, data are represented as mean±SEM for n=3–5 donors. (D) TRPA1, V1 and V4 mRNA expression was measured in HBECs and AMs using TaqMan reagents and protocols. Data are expressed as mean±SEM expression levels relative to internal control (18S). TRP, transient receptor potential; HBEC, human bronchial epithelial cells; AM, alveolar macrophages; CSM, cigarette smoking bubbled medium.
Role of TRPV1, TRPV4 and pannexin channels in CSM-mediated ATP release in vitro
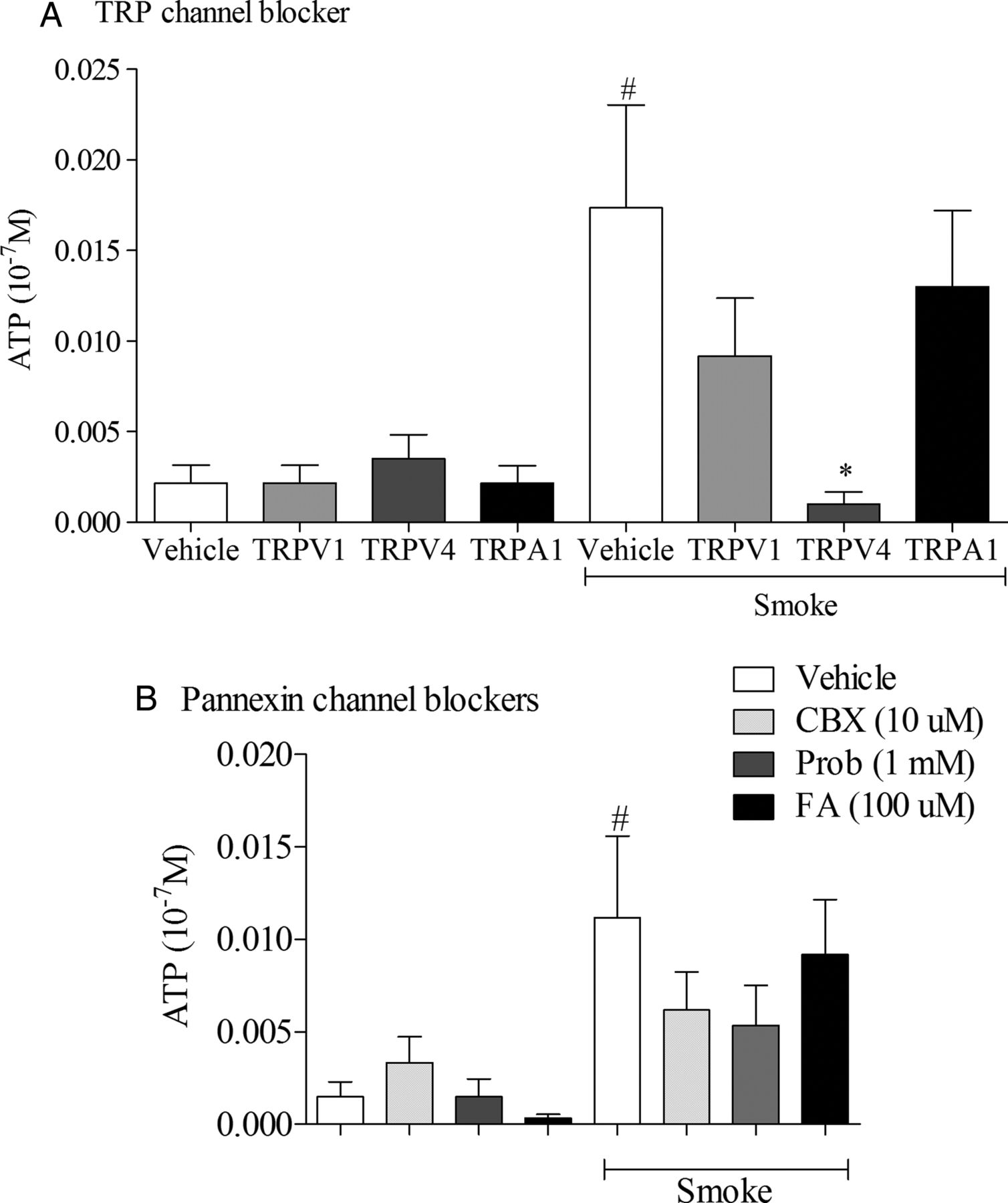
CSM-induced ATP release from HBECs was inhibited by a TRPV4 antagonist and, to a lesser extent, by a TRPV1 antagonist (figure 3). In parallel, the pannexin channel blockers (carbenoxolone and probenecid), but not the connexin channel blocker (flufenamic acid) modulated the ATP levels (figure 3). To complement the antagonist data, we examined whether specific TRP channel agonists were able to stimulate ATP release directly in HBECs. A dose-dependent ATP release was observed using the TRPV1 agonist capsaicin (figure 4A) and the TRPV4 agonist HC-067047 (figure 4B), but there was no effect with the TRPA1 agonist acrolein (figure 4C). In summary, pharmacological data advocate a role for TRPV1 and TRPV4, but not TRPA1 in CSM-stimulated ATP release from HBECs via pannexin channels.

The effect of transient receptor potential (TRP) channel and pannexin channel antagonists on cigarette smoking bubbled medium (CSM) induced ATP release in vitro. (A) Human bronchial epithelial cells (HBECs) were preincubated with either TRP channel antagonist: HC-030031 (TRPA1, 100 µM), JNJ-17203212 (TRPV1, 10 µM), HC-067047 (TRPV4, 10 µM); or vehicle (dimethyl sulfoxide (DMSO), 0.1% v/v). (B) HBECs were preincubated with either a pannexin or connexin antagonist or vehicle (DMSO, 0.1% v/v). After preincubation with the respective antagonist or vehicle for 1 h, cells were treated with 2.5% CSM or control medium and incubated for 3 h before removal of supernatants for measurement of ATP levels. Data are represented as mean±SEM for n=3 donors. #p<0.05, denoting a significant difference between the CSM-treated and control-treated vehicle groups (using Mann–Whitney U test); *p<0.05, denoting a significant difference between the respective CSM/antagonist group and the CSM/vehicle group (using one-way analysis of variance followed by Dunn's Multiple Comparison Test).

The effect of transient receptor potential (TRP) channel agonists on ATP release in vitro. Human bronchial epithelial cells (HBECs) were stimulated with increasing concentrations of agonist or vehicle. (A) TRPV1 agonist, capsaicin; (B) TRPV4 agonist, GSK 1016790A; (C) TRPA1 agonist, acrolein. Supernatants were collected 3 h after stimulation for assessment of ATP release. Data are expressed as mean±SEM for n=3 donors; *p<0.05, denoting a significant difference between the vehicle and agonist stimulation (using one-way analysis of variance followed by Dunn’s Multiple Comparison Test).
Role of P2X7 in ATP and LPS-induced IL-1β release in vitro
The above data, in combination with the published literature,15 ,16 suggests that inhaling smoke leads to the release of eATP via the activation of TRPV1/4 receptors and opening of pannexin-1 channels. ATP then acts on P2X7 receptors to trigger the release of the inflammasome products IL-1β/IL-18. Indeed, Lucattelli et al,16 using irradiated mice, suggest that this response was dependent on P2X7 receptor activation on haemopoietic cells, and not structural cells. From this, we proposed that ATP could cause the release of IL-1β from our cell-based system. Thus, we profiled the effect of ATP, and a second known IL-1β release trigger (LPS—an innate stimulus), on IL-1β levels in culture HBECs and AMs. Time points and assay conditions were chosen from previous studies.15 ,34 Neither ATP nor LPS triggered the release of IL-1β from HBECs but they did cause a concentration-induced release from AMs (figure 5). Consistent with these observations, we found significant expression levels of caspase 1 and P2X7 in AMs, but very low levels in HBECs (163±42 and 208±95 vs 0.04±0.02 and 3.7±0.7 2deltaCTx106, respectively). Finally, we found that blockade of the P2X7 receptor resulted in a concentration-related decrease in ATP-induced IL-1β release but had no effect on the normal, defensive, innate response. Together, these data support the hypothesis that ATP can induce IL-1β from haemopoietic cells (AMs) via the P2X7 receptor.

Characterisation of ATP-induced interleukin (IL)-1β release in vitro. A: Human bronchial epithelial cells (HBECs), cultured in medium with or without 3% fetal calf serum (FCS), were stimulated with ATP (0.3 mM) or vehicle (phosphate buffered saline (PBS) 0.1% v/v). Supernatants were collected 24 h after stimulation for IL-1β measurement by ELISA. B: HBECs, cultured in medium with or without 3% FCS, were stimulated with lipopolysaccharide (LPS) (0.1 µg/mL) or vehicle (PBS, 0.1% v/v). Supernatants were collected 24 h after stimulation for IL-1β measurement by ELISA. Data for (A) and (B) are represented as mean±SEM for n=3 donors. (C) and (D): alveolar macrophages (AM) were stimulated with (C) increasing concentrations of ATP from 10 to 1000 μM or (D) increasing concentrations of LPS from 0.01 to 10 μg/mL. Supernatants were collected 24 h after stimulation for IL-1β measurement by ELISA. (E) and (F) AMs were preincubated with increasing concentrations of P2X7 antagonist (AZ-11645373) or vehicle (dimethyl sulfoxide, 0.1%, v/v) for 1 h before stimulation with (E) either 1 mM ATP or vehicle; or (D) either 0.1 μg/mL LPS or vehicle. Cells were subsequently incubated for a further 24 h before collection of supernatants and measurement of IL-1β. Data for (C), (D), (E) and (F) are represented as mean±SEM for n=3 donors. (E) #p<0.05, denoting a significant difference between the ATP/vehicle treated and vehicle/vehicle-treated groups (using Mann–Whitney U test); *p<0.05, denoting a significant difference between the ATP/vehicle-treated group and the respective ATP/antagonist-treated group (using one-way analysis of variance followed by Dunn’s Multiple Comparison Test). (F): #p<0.05, denoting a significant difference between the LPS/vehicle treated and vehicle/vehicle-treated groups (using Mann–Whitney U test).
Role of TRPV1, TRPV4 and pannexin-1 channels in CS-mediated ATP release and the inflammatory response in a murine model
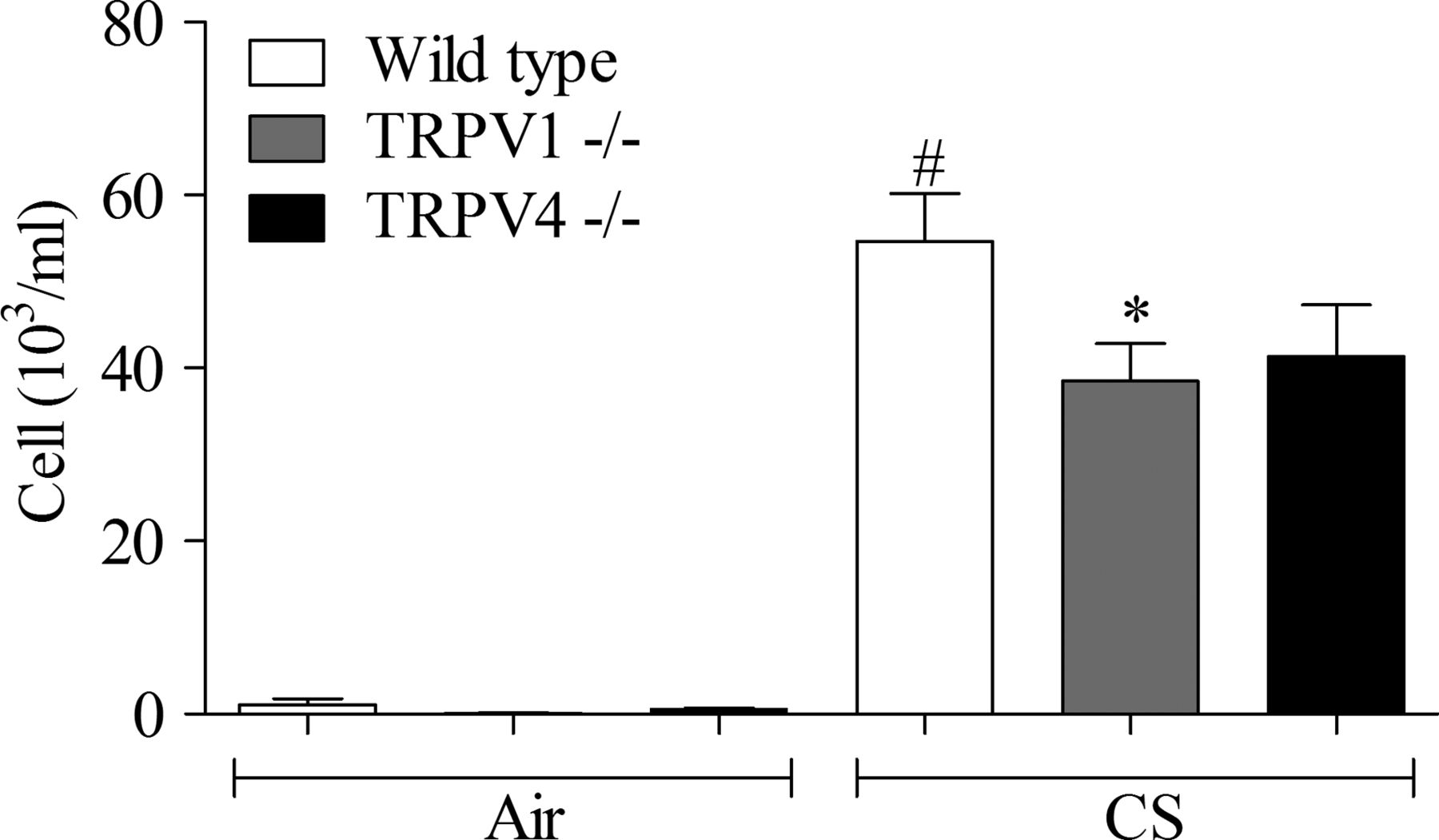
Trpv1−/− and Trpv4−/− mice were found to exhibit reduced levels of ATP, IL-1β and neutrophilia, in the BALF, after acute CS exposure (figures 6 and 7). Similarly, pannexin-1−/− mice exhibited significantly reduced levels of BALF ATP and neutrophilia compared with wild-type mice after acute CS exposure, and no increase in IL-1β levels (figure 8). In this study, we observed an increase in BALF IL-1α levels that were abolished in the pannexin-1 KOs (air/WT=16.5±7.2, air/KO=18.4±4.5, smoke/WT=36.7±4.5, smoke/KO=17.6±4.0). Interestingly, Trpv1, Trpv4 or pannexin-1 knockouts were not compromised in their ability to mount an inflammatory response to an innate stimulus suggesting that they would not be immune compromised (see online supplementary figures S2, S3 and S4). TRPA1 deficient mice did not have an altered response profile, compared with wild-type controls, after either CS or LPS challenge (see online supplementary figure S5). In the subchronic model, the numbers of neutrophils in the Trpv1−/− and Trpv4−/− mice were found to be lower than the wild-type controls (figure 9).

The role of TRPV4 in acute CS-induced murine airway inflammation. Trpv4−/− mice were exposed to CS or room air (control) twice daily for 3 consecutive days alongside wild-type controls. BALF was collected 24 h after the last exposure for measurement of neutrophil (C), IL-1β (B) and ATP (A) levels. Data are represented as mean±SEM for n=8 animals in each group. Statistical significance was determined using Mann–Whitney U test. #p<0.05, denoting a significant difference between the smoke-exposed and air-exposed wild-type groups; *p<0.05, denoting a significant difference between the smoke-exposed knock-outs and wild-types. TRP, transient receptor potential; CS, cigarette smoking; BALF, bronchoalveolar lavage fluid; IL-1β, interleukin-1β.

The role of TRPV1 in acute CS-induced murine airway inflammation. Trpv1−/− mice were exposed to CS or room air (control) twice daily for 3 consecutive days alongside wild-type controls. BALF was collected 24 h after the last exposure for measurement of neutrophil (C), IL-1β (B) and ATP (A) levels. Data are represented as mean±SEM for n=8 animals in each group. Statistical significance was determined using Mann–Whitney U test. #p<0.05, denoting a significant difference between the smoke-exposed and air-exposed wild-type groups; *p<0.05, denoting a significant difference between the smoke-exposed knock-outs and wild-types. TRP, transient receptor potential; CS, cigarette smoking; BALF, bronchoalveolar lavage fluid; IL-1β, interleukin-1β.
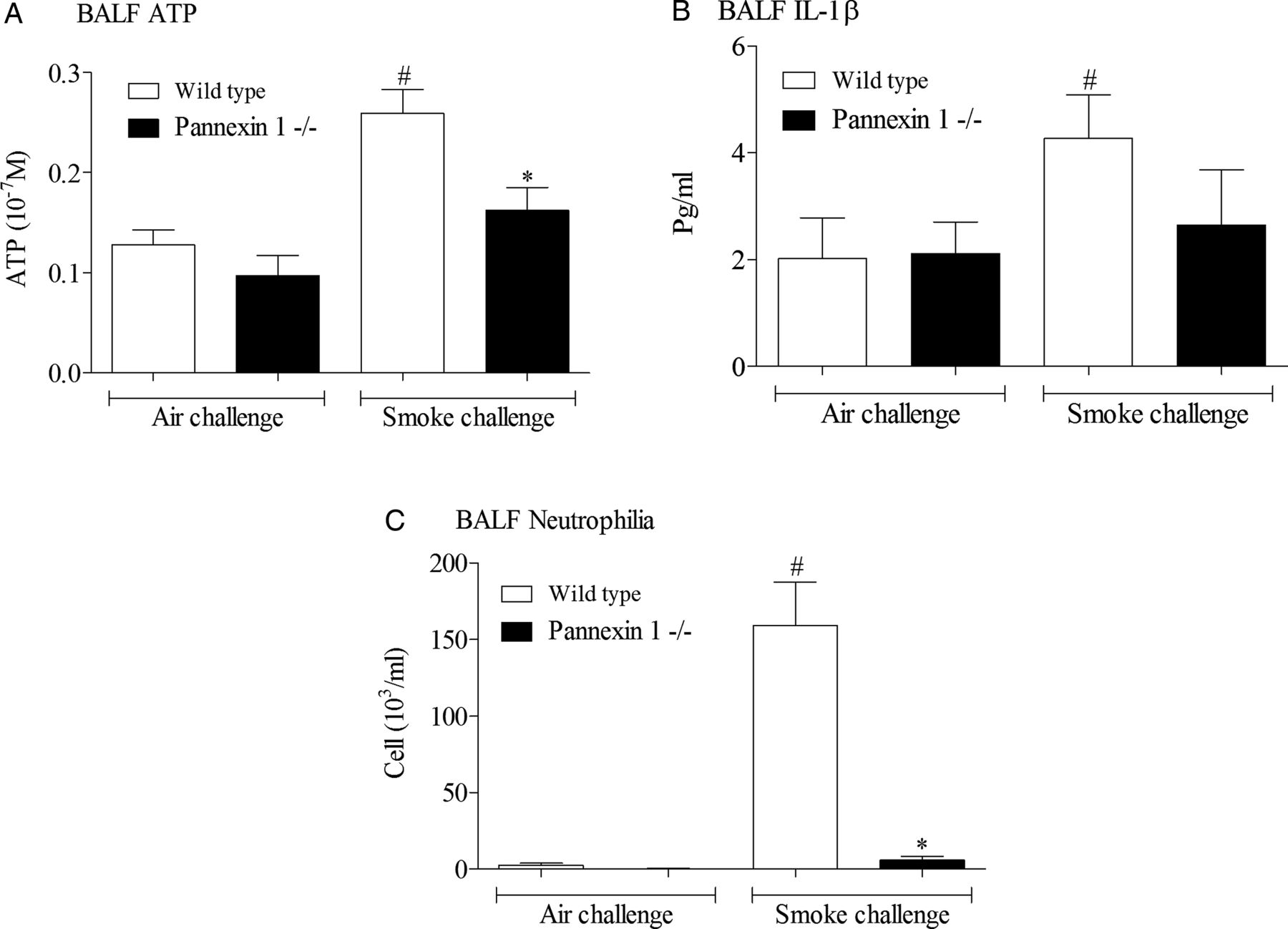
The role of pannexin-1 in acute cigarette smoking (CS)-induced murine airway inflammation. Pannexin-1−/− mice were exposed to CS or room air (control) twice daily for 3 consecutive days alongside wild-type controls. Bronchoalveolar lavage fluid (BALF) was collected 24 h after the last exposure for measurement of neutrophil (C), interleukin (IL)-1β (B) and ATP (A) levels. Data are represented as mean±SEM for n=8 animals in each group. Statistical significance was determined using Mann–Whitney U test. #p<0.05, denoting a significant difference between the smoke-exposed and air-exposed wild-type groups; *p<0.05, denoting a significant difference between the smoke-exposed knock-outs and wild-types.
The role of TRPV1 and V4 in subchronic cigarette smoking (CS)-induced murine airway inflammation. Trpv1−/− and Trpv4−/− mice were exposed to CS or room air (control) twice daily for 14 consecutive days alongside wild-type controls. Bronchoalveolar lavage fluid was collected 24 h after the last exposure for measurement of neutrophils. Data are represented as mean±SEM for n=8 animals in each group. Statistical significance was determined using analysis of variance with a Bonferroni post-test; #p<0.05, denoting a significant difference between the smoke-exposed and air-exposed wild-type groups; *p<0.05, denoting a significant difference between the smoke-exposed knock-outs and wild-types.
Taken together, these data suggest that CS mediates inflammation in these murine in vivo models by activation of TRPV1 and TRPV4 (but not TRPA1), leading to ATP release via pannexin channels.
Expression of TRPV1 and TRPV4 in patients with COPD
To assess the translational merits of this murine in vivo data, we examined the expression levels of selected TRP channels in human lung parenchyma from healthy non-smokers, healthy smokers and patients with COPD (see table 1 for demographic details). TRPV1 and TRPV4 expression levels were significantly increased in patients with COPD compared with healthy non-smokers, but there was no difference between healthy smokers and healthy non-smokers (figure 10A, D). There was no difference in TRPV2 expression between any of the groups (figure 10B). TRPV3 expression was below the detection limits of the assay in all three groups (figure 10C). TRPA1 levels were below the assay's reliable detection limit.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transient receptor potential (TRP) channel expression in human lung parenchyma. Human lung parenchymal samples were collected from healthy non-smokers, healthy smokers and patients with COPD. RNA was extracted and reverse transcribed to cDNA before measurement of TRPV1 (A), TRPV2 (B), TRPV3 (C) and TRPV4 (D) mRNA expression levels using TaqMan reagents and protocols. Data are expressed as mean±SEM expression levels relative to internal control (18S); #p<0.05, denotes a significant difference between healthy smokers and patients with COPD, determined by one-way analysis of variance followed by Dunn's multiple comparisons posthoc test.
While this data is encouraging, it is necessary to confirm these finding in samples harvested from a larger, well characterised patient group. Furthermore, the parenchyma was not sampled from specific anatomical positions for a truly accurate comparison.
Discussion
Chronic exposure to CS is a key causative factor in the development of COPD.39 It is thought to result in a dysregulated inflammatory response in the airways characterised by high levels of leucocyte infiltration and inflammatory mediator release which drive disease progression and lung function decline. Elucidation of the pathways which mediate CS-induced inflammation is likely to uncover novel targets for the development of effective therapies. Patients with COPD exhibit increased levels of eATP, IL-1β and IL-18 in the BALF, as well as increased expression of P2X7 and caspase-1 in leucocytes and lung tissue, and importantly, these markers are found to correlate with disease severity.6 ,7 ,12 ,15 Murine in vivo models of CS-induced airway inflammation have also been shown to be dependent on the P2X7-dependent activation of caspase-1 to mediate the maturation of cytokines IL-1β and IL-18, indicating that these models have disease relevance. Pharmacological and/or genetic manipulation of ATP and these proteins have been shown to attenuate CS-induced neutrophilia in both acute and more chronic murine models, suggesting that modulation of this pathway could potentially reduce the steroid-resistant inflammation which drives the progression of COPD.15 ,16 ,40 Despite this wealth of data indicating a role for ATP, the mechanism by which it is released after exposure to cigarette smoke has so far eluded researchers and, if identified, could reveal novel targets for the development of truly effective therapies.
The data presented herein strongly advocate a crucial role for TRPV1 and TRPV4 channels in the pannexin-1-mediated release of ATP in response to acute CS exposure. This was demonstrated in human primary cells using TRPV1, TRPV4 and pannexin-1-specific antagonists to block CSE-induced ATP release, as well as TRPV1 and TRPV4 agonists to directly elicit ATP release. The importance of this TRP channel pannexin-1 axis was recapitulated in vivo using colonies of Trpv1−/−, Trpv4−/−, and pannexin-1−/− genetically deficient mice. Importantly, these mice exhibited reduced ATP levels after acute CS exposure, and they also exhibited attenuated IL-1β and neutrophil levels in BALF compared with wild-type, demonstrating that this pathway is integral to acute CS-induced inflammatory response, which is thought to drive the progression of COPD. These findings provide a novel insight into the role of these channels in the generation of acute CS-induced airway inflammation. By comparison, genetic ablation of the P2X7 receptor was found to protect CS-exposed mice against increased BALF IL-1β and neutrophilia, but did not alter ATP release. These observations indicate that ATP is released upstream of P2X7 receptor activation in this model and help to unravel the relationship between pannexin-1 and the inflammasome. These data support the hypothesis that in this system, pannexin-1 stimulation results in inflammasome activation indirectly, via the release of eATP resulting in subsequent P2X7 activation.21 While these data in the acute and subchronic models are very exciting, further work in chronic models is required to fully elucidate the role of this axis in the pathogenesis of clinical COPD.
Evidence suggests that this inflammatory pathway is important in COPD, as translational data has shown increased levels of P2X7 expression and caspase-1 activation in CS-exposed wild-type mice and in patients with COPD.12 ,15 Furthermore, the preliminary demonstration that TRPV1 and TRPV4 gene expression are also upregulated in lung tissue from patients with COPD suggests that these channels may be important for the CS-mediated release of eATP in this disease. It could also provide some preliminary insight into COPD susceptibility and indicate why only a certain percentage of smokers develop COPD (i.e. increased channel expression means higher levels of ATP). Indeed, TRPV4 single nucleotide polymorphisms have been associated with COPD susceptibility in two separate studies.41 ,42
An interesting feature of this inflammatory pathway is the fact that release of eATP to activate the P2X7-inflammasome-caspase-1 axis facilitates the production of IL-1β and IL-18 without the need for transcriptional upregulation of the genes which encode these proinflammatory cytokines. Rather, there are substantial levels of the proforms of these cytokines constitutively present in the cytosol, for which caspase-1 facilitates the maturation to active, proinflammatory mediators. Indeed, previous investigation of murine models has demonstrated that IL-1β mRNA levels are not affected by CS exposure, despite significantly higher levels of IL-1β protein.15 This may, in part, explain the insensitivity of patients with COPD to glucocorticoids, as they are generally thought to exert their anti-inflammatory effects by modulation of inflammatory cytokines at the transcriptional level. Pharmacological intervention at the TRPV1/4-pannexin-1 axis may, therefore, prove to be an effective anti-inflammatory therapeutic strategy where glucocorticoids have failed. Furthermore, TRPV1, TRPV4 and pannexin-1 gene-deleted mice mounted a normal innate immune response to inhaled bacterial mimetic, LPS, suggesting that therapies that target this axis would not immune-compromise patients. To confirm this suggestion, further work is required with live bacteria and respiratory viruses. Somewhat surprisingly, TRPA1 did not play a role in CS-induced inflammation in either the in vivo or in vitro models even though it can be directly activated by acrolein, one of the key components of CS. One explanation could be that the cell types we studied did not express TRPA1.
A question remains regarding the mechanism by which CS activates TRPV1 and TRPV4 in these models. We initially hypothesised that TRPV1 and TRPV4 may be activated by low pH, but analysis of the CSM would suggest otherwise. Furthermore, changes in osmolarity, a known trigger of TRPV4 activation,27 seems an unlikely scenario in this model system. Therefore, it would seem that either constituents in CSM directly trigger the channels or they result in the production of a channel modulator. Indeed, we are currently exploring ways of identifying likely candidates from the 4000+ chemicals reported to be present in CS. It is also currently not clear how activation of TRP channels triggers the opening of the pannexin-1 pore. The most likely mechanism would simply be that increases in intracellular Ca2+ and membrane depolarisation are sufficient or that a second messenger signal is required.18 However, the fact that the pannexin-1 pore is central to the response does mirror observations made by others in different biological systems.22–24 ,26 ,27 The time course of ATP release in vitro is intriguing, it would appear that the release is a not a rapid process (taking a few hours to reach a plateau), suggesting that either the process is slow or that perhaps the CS induction of the possible TRP channel activators takes time. Furthermore, the data would suggest that the cells stop releasing ATP after a time or that enzymes which cleave it are induced.
Finally, it is unclear why ATP is still detectable, especially in vivo, as one would assume that under normal circumstances ATP would be cleaved rapidly. Indeed, preliminary studies with exogenous ATP added to BALF from smoke-exposed mice showed that it is undetectable with the specific ATP assay used. This suggests that the ecto-ATPases that breakdown ATP are functional in the CS-exposed mouse lung and perhaps the ATP measured in the BALF by our group and others is somehow protected from enzymatic activity, and this observation warrants further investigation.
In summary, this data represents a significant breakthrough in understanding the mechanism by which CS exposure leads to the release of ATP. Furthermore, preliminary expression data in clinical samples appears to validate the preclinical findings. We, therefore, propose that pharmacological modulation of the TRPV1/4-pannexin-1 axis may provide clinical benefit to patients with COPD by attenuating the dysregulated, steroid-resistant inflammation which is associated with the decline in lung-function seen in patients with COPD.
Acknowledgments
P2×7−/− mice were kindly supplied by Professor Jean Kanellopoulos, Université Paris-Sud, France, Trpv4−/− mice were kindly supplied by Riken Bioresource Centre, and Dr Vishva Dixit from Genentech generously provided the pannexin 1 -/- mice.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors Conception and design: MB, MGB, MAB. Data generation, analysis and interpretation: MB, SE, BD, LY-B, EDD, SAM. Drafting the manuscript for important intellectual content: MB, MGB, MAB. All authors reviewed the manuscript and approved the final draft
Competing interests MB was supported by an NHLI COPD PhD studentship, SE was supported by a postdoctoral award from Roche Pharmaceuticals, Nutley, USA. LY-B was funded by a Capacity Building Award in Integrative Mammalian Biology funded by the BBSRC, BPS, HEFCE, KTN & MRC. EDD was funded by a Wellcome Trust project grant (089301/Z/09/Z) and Boehringer-Ingelheim. SAM and MAB were funded by project grants from the MRC, UK (G0800195 and G0800196, respectively). The human tissue experiments in this study were undertaken with the support of the NIHR Respiratory Disease Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London.
Provenance and peer review Not commissioned; externally peer reviewed.