Article Text

Abstract
Retrospective prescribing data were obtained from 46 general practice surgeries in NHS Scotland. Patients with asthma who were naïve to previous long-acting β agonist therapy and initiated combination inhaler therapy in 2008–2009 were classified according to the inhaled corticosteroid (ICS) dose in their combination inhaler compared with the highest dose of ICS they received before initiation. Among the 685 patients (541 (79.0%) who had been prescribed an ICS previously), those originally on low-, medium- or high-dose ICS were changed to high-dose combination therapy in 122/250 (48.8%), 94/151 (62.3%) or 85/113 (75.2%) cases in each ICS dose category, respectively. These results suggest that evaluation of appropriate high-dose ICS prescribing in general practice is needed.
- Asthma Epidemiology
- Asthma in primary care
- Asthma Guidelines
Statistics from Altmetric.com
Introduction
Management of chronic asthma in the UK is guided by a stepwise approach recommended by the British Thoracic Society and Scottish Intercollegiate Guideline Network (BTS/SIGN) guideline.1 Combination therapy with an inhaled corticosteroid (ICS) and long-acting β agonist (LABA) is the preferred treatment at step 3 when the use of an ICS alone is insufficient for the control of persistent asthma, which is defined by the presence of symptoms, their effect on the patient's quality of life and the future risk of adverse events such as exacerbation.1 Previously, escalation of ICS dose was advocated to achieve optimal control; however, major international guidelines now agree on the therapeutic benefits of adding LABA therapy to ICS therapy.
The appropriate use of combination therapy has also been questioned. Breton et al2 described the prescribing of combination therapy against the current Canadian asthma guidelines and found that only 40% of patients prescribed combination therapy had received a prescription for an ICS in the preceding year. However, no analyses to our knowledge have described ICS dose transitions on initiation of combination therapy in patients in general practice. The aim of this study was to describe dose changes during the transition from ICS to newly initiated combination inhaler therapy in patients with asthma.
Methods
A retrospective database analysis was conducted in 46 practices (approximately 80% coverage) in the Forth Valley Health Board of National Health Service (NHS) Scotland, which serves nearly 300 000 patients in a representative area. Patients were included if they: (1) had physician-diagnosed asthma; (2) had their first prescription for a combination inhaler (fluticasone/salmeterol or budesonide/formoterol) between 1 January 2008 and 31 December 2009; and (3) were naïve to LABA therapy in the year before initiation of combination inhaler therapy. The date of the first prescription for combination inhaler was considered the index date for each patient.
Doses of the ICS component in both single-agent and combination inhalers were obtained from the prescription posology and standardised to beclometasone dipropionate (BDP) according to the BTS/SIGN guideline.1 For patients aged >12 years, low-dose ICS was defined as ≤400 µg daily, medium-dose ICS as >400 µg daily and ≤800 µg daily and high-dose as ICS >800 µg daily; for patients aged ≤12 years the dose cut-offs were halved.1 Patients were assessed according to highest ICS dose they received in the year before the index date and the first dose of ICS in the combination therapy inhaler they received on the index date. Sensitivity analyses excluding patients with comorbid chronic obstructive pulmonary disease (COPD) and looking specifically at children were also performed. The use of short-acting β agonist (SABA) and oral corticosteroid (OCS) in the year before the index date were quantified as markers of asthma symptoms and exacerbations, respectively.
Results
Six hundred and eighty-five patients started combination inhaler therapy during the study period. The majority of patients were women (403; 58.8%) with a median age of 47 years (IQR 32–62 years); 89 (13.0%) patients were concurrently listed on practice COPD registers. A total of 541 (79.0%) patients had been prescribed an ICS inhaler in the year before the index date. BDP was the most widely prescribed ICS among patients before the index date (294; 54.1%) and fluticasone/salmeterol was the most common combination inhaler therapy choice (497; 72.6%).
The mean standardised dose of ICS before the index date was 677 µg compared with 1043 µg on initiation of combination inhaler therapy, resulting in a mean increase in dose of 354 µg (95% CI 302 to 407; p<0.001). Patients originally on low- or medium-dose ICS had mean dose increases of 550 µg (95% CI 483 to 618) or 275 µg (95% CI 186 to 363), respectively (both p<0.001); patients originally on high-dose ICS had similar doses pre- and post-index (mean difference 21 µg, 95% CI −97 to 139; p=0.723).
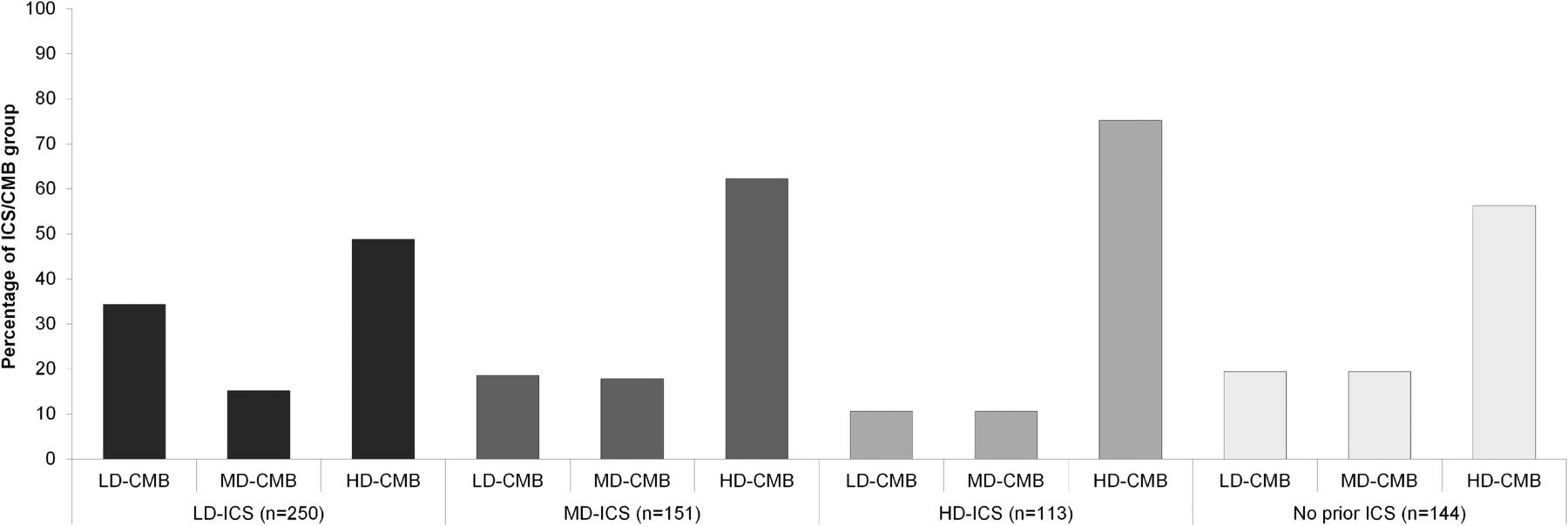
When patients were classified according to ICS dose categories, patients on low-, medium- and high-dose ICS before the index date were changed to high-dose combination inhalers in 122/250 (48.8% of ICS category), 94/151 (62.3%) and 85/113 (75.2%) patients, respectively (figure 1). Patients with no recorded prescribing of ICS pre-index were changed to high-dose combination inhalers in 81/144 cases (56.3%). Fifty-two patients (10.3% of those with pre-index ICS) were changed to a lower dose combination inhaler than their pre-index ICS dose. A small number of patients (27, 3.9% of total) had unclear prescription instructions and were excluded. Excluding the 129 patients with comorbid COPD resulted in no significant changes in the overall classification, with an overall mean dose increase of 463 µg (95% CI 406 to 520) and high-dose combination inhalers remaining the post-index treatment choice in 321/596 patients (53.9%; comparison with the original cohort: p=0.195). Forty-four children were included in the analysis, with the majority (27; 61.4%) changing from low-dose ICS to low-dose combination therapy and only nine (20.5%) receiving high-dose combination therapy.
{kind=link}
Changes in inhaled corticosteroid (ICS) dose at the index date. CMB, combination therapy; HD, high dose; LD, low dose; MD, medium dose.
Overall, 649 (94.7%) and 199 (29.1%) patients had received at least one prescription for SABA or OCS in the previous year, respectively. The number of SABA inhalers prescribed was similar (albeit variable) regardless of baseline ICS dose, with a median of six inhalers/year (IQR 2–12; p=0.145 for comparison among ICS categories). The number of OCS courses was also similar with a median of two prescriptions/year (IQR 1–3; p=0.306).
Discussion
This analysis demonstrates significant use of high-dose combination therapy among patients with asthma treated in GP surgeries. Widespread use of high-dose ICS in the UK has been noted previously. Thomas et al3 found that, within a prescribing analysis of over 22 000 adults/adolescents with asthma, 27% of patients received high-dose ICS and 83.6% of them had no record of a trial of add-on therapy with a LABA or other controller therapy. The present analysis found that over three-quarters of patients received ICS therapy before starting treatment with a combination inhaler, suggestive of better concordance with guideline recommendations. However, on addition of a LABA to the treatment regimen, there was a widespread pattern of simultaneous ICS dose escalation with patients advancing directly to high-dose combination therapy, largely irrespective of their baseline ICS dose. This suggests not only questionable use of high-dose ICS but also failure to follow guideline recommendations.
The dose-response relationship of ICS has been the subject of much research, although high-quality evidence indicates that the therapeutic benefits of ICS are seen at doses of 200–1000 μg BDP equivalent daily.4 ,5 Above this threshold, adverse effects of ICS such as hypothalamic-pituitary-adrenal axis suppression, osteoporosis and skin bruising are more common. Accordingly, the wide utilisation of high-dose ICS is likely to produce a poor return on investment, with an increased risk of local and systemic adverse effects traded for little gain in asthma control. Although as a database analysis we were unable to determine the clinical reasoning underlying ICS dose changes, the patterns noted in this study should prompt further investigation into the appropriateness of high-dose ICS prescribing in UK general practice.
Fluticasone/salmeterol was the most commonly used high-dose combination therapy in this analysis, but the reasons behind this are unclear. Fluticasone may be preferentially chosen for treatment due to its potency and ease of dosing regimen to achieve higher doses. A post hoc analysis found that, of the 394 patients prescribed high-dose combination therapy, 149 (37.8%) were prescribed doses ≥1600 μg daily (very high-dose ICS), and all but five of these patients received fluticasone/salmeterol. However, we also acknowledge that this prescribing may be inadvertent, and that a lack of awareness of potency differences between different ICS preparations may lead to the product being prescribed at twice the intended dose of budesonide/formoterol. Another contributing factor may be the licensing of high-dose combination therapy for the treatment of COPD. The analysis included patients with comorbid COPD as this group of patients is often excluded from randomised controlled trials despite constituting 5–20% of the asthma population. While it would be plausible that the inclusion of this patient group would inflate the use of high-dose combination therapy, the results of our sensitivity analysis showed no differences from the full cohort. However, clinicians may feel more comfortable prescribing larger doses of ICS for asthma than previously due to widespread use of high-dose ICS in COPD, and may alter their prescribing practices for patients with asthma.
There was no discernible pattern of SABA/OCS prescribing among ICS dose categories, suggesting that patient symptoms and/or exacerbations were not primary motivators for dose increases during the initiation of combination inhaler therapy in this analysis. While symptoms and/or exacerbations may push a clinician to escalate treatment rapidly, changing a patient from no ICS therapy to high-dose combination therapy remains a concern and there is little evidence to support this approach. Our analysis did uncover some ICS dose step-down, albeit with the concurrent addition of a LABA (medium-dose ICS changed to low-dose combination inhaler). Although this was only seen in a small number of patients, it may provide some reassurance to the use of increasing doses of ICS and combination therapy.
High-dose combination inhalers were prescribed frequently in this UK cohort with asthma, even without a history of ICS treatment. Evaluation of the appropriateness of high-dose prescribing in general practice is needed, and educational efforts should focus on the dose-response relationship of ICS and the risk of adverse effects when using high-dose ICS.
Acknowledgments
The authors thank the NHS Forth Valley Airways Managed Clinical Network for provision of the data.
Footnotes
-
Contributors ACB, FW and JRC were responsible for the concept of the study, BFJ for the analytical methods and JRC for handling of the data and execution of the analysis. All authors interpreted the data, wrote the manuscript, had access to the data and made the decision to submit for publication. ACB is the guarantor.
-
Funding US-UK Fulbright Commission and the University of Strathclyde. The NHS Forth Valley Airways Managed Clinical Network provided the database used in this analysis.
-
Competing interests JRC has received support in the form of a PhD studentship from the US-UK Fulbright Commission and the University of Strathclyde. FW and ACB have received meeting support from Novartis and GlaxoSmithKline, respectively. ACB is a member of the steering committee for the BTS/SIGN asthma guideline.
-
Ethics approval Departmental ethics was consulted regarding use of the database and it was determined that no formal review was required.
-
Provenance and peer review Not commissioned; externally peer reviewed.