Article Text

Abstract
Interleukin 17 (IL-17) is a key proinflammatory cytokine in the T helper 17 pathway. While it is important in the clearance of certain pathogens, IL-17 has been shown to contribute to the pathogenesis of such inflammatory diseases as rheumatoid arthritis and psoriasis. In the lung, it has been postulated to be involved in the neutrophilic inflammation and airway remodelling of chronic respiratory conditions but the situation is increasingly complex. This review summarises the evidence for its role in several chronic inflammatory lung diseases: asthma, obliterative bronchiolitis, chronic obstructive pulmonary disease, sarcoidosis and cystic fibrosis.
- Cytokine Biology
- Asthma
- Cystic Fibrosis
- Respiratory Infection
Statistics from Altmetric.com
Introduction
Interleukin 17 (IL-17) is one of the few cytokines a chest physician should have knowledge of, not least because of its importance in the history of immunology. T helper (Th) lymphocytes used to be divided into Th1 cells (involved in cell-mediated immunity) and Th2 cells (antibody-mediated immunity). This Th1/Th2 dichotomy provided the initial framework for understanding immune regulation. The discovery of a population of IL-17-secreting Th cells, which were neither Th1 nor Th2, led to a major revision of the Th1/Th2 hypothesis. Named Th17 cells, they have their unique cytokine profile (IL-17, IL-21, IL-22), transcription factors (retinoic orphan receptor γt) and differentiation factors (IL-6, IL-21, IL-23, IL-1β and transforming growth factor β (TGFβ)).1 The primary function of Th17 cells appears to be the clearance of pathogens inadequately addressed by Th1 and Th2 cells. In mice, IL-17 is important in clearing organisms such as Klebsiella pneumoniae and Mycoplasma pneumoniae. Th17 cell differentiation is impaired in patients with hyper-IgE syndrome, the likely mechanism underlying their increased susceptibility to infections with Staphylococcus aureus. However, there are situations when their role as mediators of inflammation results in pathology.
IL-17 acts on a wide range of cells, including those from haemopoietic, endothelial, epithelial and mesenchymal lineages. It is involved in granulopoiesis; can induce the expression of numerous proinflammatory cytokines such as tumour necrosis factor α, IL-1β, granulocyte macrophage colony-stimulating factor, granulocyte colony-stimulating factor and IL-8; is a key cytokine for the recruitment and activation of neutrophils; and has been shown to regulate neutrophil migration in the lung. It may play a role in airway remodelling as it can enhance the production of the profibrotic cytokines IL-6 and IL-11 from fibroblasts isolated from human bronchial biopsies. In addition, intranasal administration of IL-17 in mice resulted in an increase in the concentration of matrix metalloproteinase 9 (MMP-9), a proteolytic enzyme that can degrade structural compounds including extracellular matrix. It has therefore been postulated that IL-17 could be involved in the pathogenesis of chronic respiratory conditions when there is neutrophilic inflammation and airway remodelling. A brief overview of some key findings is given below.
Asthma
While asthma has principally been considered a Th2 disease, IL-17 may contribute to its pathogenesis. Certainly, the number of IL-17+ cells in endobronchial biopsies of patients with asthma is increased in a disease severity dependent manner.2
In mouse models, the evidence is quite contradictory, likely due to the use of different mouse strains and allergen sensitisation protocols. Th17 cells can upregulate Th2 cell-mediated eosinophilic airway inflammation. IL-17 can enhance airway smooth muscle contraction and proliferation, and epithelial permeability of the airways to allergen.3 Th17-deficient mice have been shown to be protected from airway hyperesponsiveness in response to house dust mite and ovalbumin sensitisation/challenge and also display less airway remodelling after chronic allergen challenge.
However, it is now known that IL-17 can be secreted by other cells besides Th17 cells. IL-17-producing γδT cells have been shown to mediate the resolution of allergic airway inflammation and airway hyperreactivity in a murine model of ovalbumin-induced allergic inflammation while adoptive transfer of Th17 cells had no such effect.4 In Thorax, IL-17 has been shown to inhibit respiratory syncytial virus induced airway hyperresponsiveness during ovalbumin-induced allergic inflammation.5 These data suggest that IL-17 may play different roles in the airway, depending on the cellular source and context.
Obliterative bronchiolitis
Lung transplant recipients who develop bronchiolitis obliterans (OB) have increased IL-17 and Th17 differentiating cytokines (IL-1β, IL-6 and IL-23) in bronchoalveolar lavage fluid (BALF) compared with controls and patients with acute rejection.6 In a murine model of orthotopic lung transplantation, IL-17 levels were higher in mice that developed OB compared with those that did not. Neutralisation of IL-17 in these mice prevented the development of OB.
Sarcoidosis and COPD
In patients with sarcoidosis, Th17 cells localise inside and around the lung granulomas with more Th17 cells in the BALF of patients with marked alveolitis compared with controls.7
In patients with chronic obstructive pulmonary disease (COPD), IL-17 expression is upregulated in the bronchial submucosa. Th17 cells are present and CD8 IL-17-secreting cytotoxic T cells have also been identified. IL-17+ neutrophils are also present in induced sputum from patients with COPD.
Cystic fibrosis
IL-17 and IL-23 are elevated in the sputum of adult patients with cystic fibrosis (CF) during respiratory exacerbations, and decreased after antibiotic treatment. Clinically stable adult patients with CF were also found to have higher levels of IL-17 protein and IL-23 mRNA levels in their sputum compared with healthy controls. In children with CF, Th17 lymphocytes are present in the submucosa of endobronchial biopsies from early in the course of the disease and could be among the earliest drivers of the inflammatory response.8 IL-17+ neutrophils and γδT cells have also been identified. There was a significant correlation between BALF IL-17 levels and neutrophil counts and the presence of IL-17+ neutrophils may be indicative of a positive feedback loop, that is, initial production of IL-17 by γδT/Th17 cells attracts neutrophils, which then produce more IL-17, resulting in further neutrophil recruitment. Intriguingly, children with CF with raised levels of IL-17 in their BALF were more likely to become culture positive for Pseudomonas aeruginosa in the subsequent 2 years.9
In a murine model of chronic P aeruginosa lung infection, early IL-23-induced secretion of IL-17 by γδT cells was seen, followed by a later Th17 response. IL-23p19−/− mice had less induction of IL-17, MMP-9, decreased BALF neutrophils, and less airway inflammation, although no difference in bacterial colony-forming units or survival rates compared with controls,10 suggesting IL-23 may be a potential therapeutic target to reduce airway inflammation in CF.
Conclusion
Mechanistic studies are needed. A current postulated model of the role of IL-17 in the pathogenesis of chronic inflammatory lung conditions is shown in figure 1. New therapies targeting IL-17/Th17 pathways have been proposed as attractive avenues of investigation. Antibodies to the p40 subunit of IL-23 have shown promise in the treatment of psoriasis. Similarly, simvastatin which inhibits IL-17 has been shown in animal studies to prevent OB. However, it is important to remember that presence in disease does not necessarily imply causation. The role of Th17 and other IL-17+ cells still needs clarification: are they beneficial or pathogenic and under what circumstances? Different IL-17+ cells may have differing functions: Th17 cells seem to be proinflammatory, yet IL-17+ γδ T cells may be the opposite. Indeed, not all Th17 cells are equal: murine Th17 cells induced by TGFβ3 were pathogenic, whereas those induced by TGFβ1 were not. Furthermore, the plasticity of Th populations is now recognised: a reporter mouse strain has shown that Th17 cells can take on a Th1 phenotype. Overall, a network of cross regulation between Th cell subsets exists, dictated by the particular local cytokine milieu, which in turn is influenced by pathogens and the local environment. Blanket suppression of all IL-17 may have unintended consequences, particularly in the lung which is constantly being challenged with antigens and pathogens. The discovery of IL-17 has opened up new areas of potential therapy, but given the complexity of immunological interactions, the excitement that these are generating should perhaps be tempered to ‘cautious optimism’.
{kind=link}
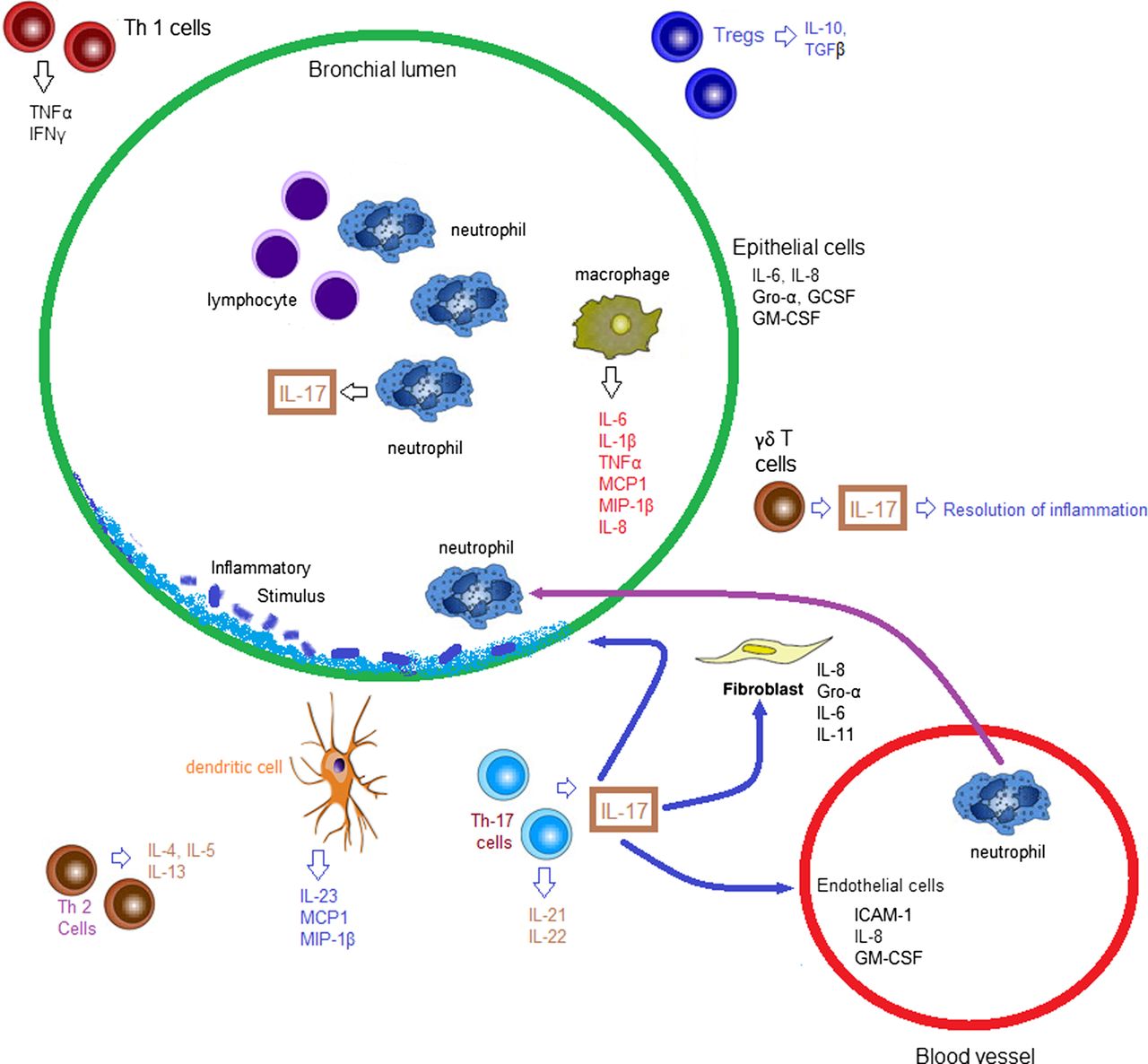
Postulated model of the role of interleukin 17 (IL-17) in the pathogenesis of chronic inflammatory lung conditions. While in acute infection, IL-17 from γδT cells and T helper 17 (Th17) cells can result in clearance of the pathogen and resolution of infection, persisting activation of inflammatory pathways can promote chronic IL-17 production. As IL-17 is a key cytokine for the recruitment and activation of neutrophils and neutrophils themselves can secrete IL-17, a vicious cycle of over-exuberant inflammation can occur with resulting inflammation-mediated damage. This cycle would be augmented by other cytokines such as IL-8. Airway remodelling can occur secondary to the inflammation, but IL-17 itself can also induce profibrotic cytokines and matrix metalloproteinase 9 (MMP-9) expression, which may also play a role in airway remodelling. GCSF, granulocyte colony-stimulating factor; GM-CSF, granulocyte macrophage colony-stimulating factor; Gro-α, growth-regulated oncogene α; ICAM-1, intercellular adhesion molecule 1; IFNγ, interferon γ; MCP1, monocyte chemoattractant protein 1; MIP-1β, macrophage inflammatory protein 1β; TGFβ, transforming growth factor receptor β; TNFα, tumour necrosis factor α; Treg, T-regulatory cell.
References
Footnotes
-
Contributors Both authors contributed to the manuscript.
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.