Article Text

Statistics from Altmetric.com
- Screening
- overdiagnosis
- lung cancer
- alveolar cell cancer
- imaging/CT, MRI
- non-small cell lung cancer
- thoracic surgery
‘Is cure necessary for those in whom it is possible and possible in those in whom it is necessary?’ Willet Whitman.
Introduction
A cancer diagnosis strikes intense fear in us, and for good reason. Cancer is the leading cause of death in people aged less than 85 years,1 and is viewed as a death sentence which few can escape. Lung cancer is particularly ominous, accounting for more than the next three leading causes combined.
However, the National Lung Screening Trial provides hope, demonstrating 20% less lung cancer deaths through CT screening.2 This study also stimulates a focus on overdiagnosis—meaning, any cancer that would not result in death if left untreated. This concept contrasts starkly with the general view of lung cancer as a rapidly fatal disease. This binary, black-and-white view glosses over nuances and hampers a true understanding. Our conceptual framework profoundly affects our understanding of issues, and our thinking must keep pace with advances in an increasingly complex world. This article explores the concept of overdiagnosis and potential implications of CT screening.
Overview of overdiagnosis
Extensive evidence indicates that overdiagnosis occurs in many cancers3; although difficult to quantify, the proportion is substantial. Autopsy studies, and studies involving resections for non-malignant reasons (eg, prostatic hypertrophy), suggest undiagnosed prostate, thyroid, breast or lung cancers exist in 10–70% of middle-aged and older individuals.3–5 In addition, long-term follow-up of randomised screening studies (allowing for ‘catch-up’ cancers that are diagnosed later in the non-screened arms), suggests that 15–50% of breast and lung cancers represent overdiagnosis in mammography and chest radiograph screening studies.3 ,6 ,7 Probably the strongest evidence comes from population-based studies demonstrating that in many cancers the rate of diagnosis has doubled or tripled, yet the death rate remains unchanged (eg, melanoma, thyroid, renal carcinoma).3 The increased rate of diagnosis typically tracks consistently with increased use of methods of detection (ie, skin biopsies or imaging).3 This phenomenon is not only restricted to cancer; while the death rate from pulmonary embolism has been stable, the incidence has increased dramatically since 2000, neatly tracking the rate of use of CT angiography for diagnosis.8 However, overdiagnosis is not an inevitable consequence of screening as there is little evidence of overdiagnosis resulting from screening for cervical and colon cancer.3
The traditional view is that any cancer that is not fatal (if left untreated) is an overdiagnosed cancer (figure 1).9 Thus, an indolent tumour that does not grow significantly, does not cause symptoms, and allows the patient to die of other causes at a ripe old age is an overdiagnosed cancer. The idea of classifying such tumours as overdiagnosed is readily accepted, although there may be hesitation among clinicians who, traditionally, have only encountered life-threatening cancers to accept the premise that such indolent and inconsequential cancers exist.

Traditional view of overdiagnosis. The detection of very indolent tumours in the screened group produces apparent increases in the number of cases of lung cancer (three in the screened group in the figure and one in the control group were diagnosed) and in survival (67% in the screened group vs none in the control group), with no effect on mortality (one death from lung cancer in each group). These results are seen because two patients in the screened group were diagnosed with cancers that were not destined to affect their natural lifespan (overdiagnosed cancers).9
However, problems arise when one considers that overdiagnosis also includes other situations. Tumours grow at varying rates; a tumour would be labelled as overdiagnosed if a decision was made not to treat a slow-growing tumour in a vigorous 70-year-old man who eventually dies of the cancer at the age of 80 years (figure 2). At the other extreme, even an extremely rapidly growing cancer is ‘overdiagnosed’ if the patient dies of some other cause (figure 2), which may be an unexpected event (eg, being struck by a bus), or an expected one from a major co-morbidity (eg, congestive heart failure). Each of these situations have very different implications for the individuals involved, our ability to predict their risk, and how we approach them in clinical patient management.
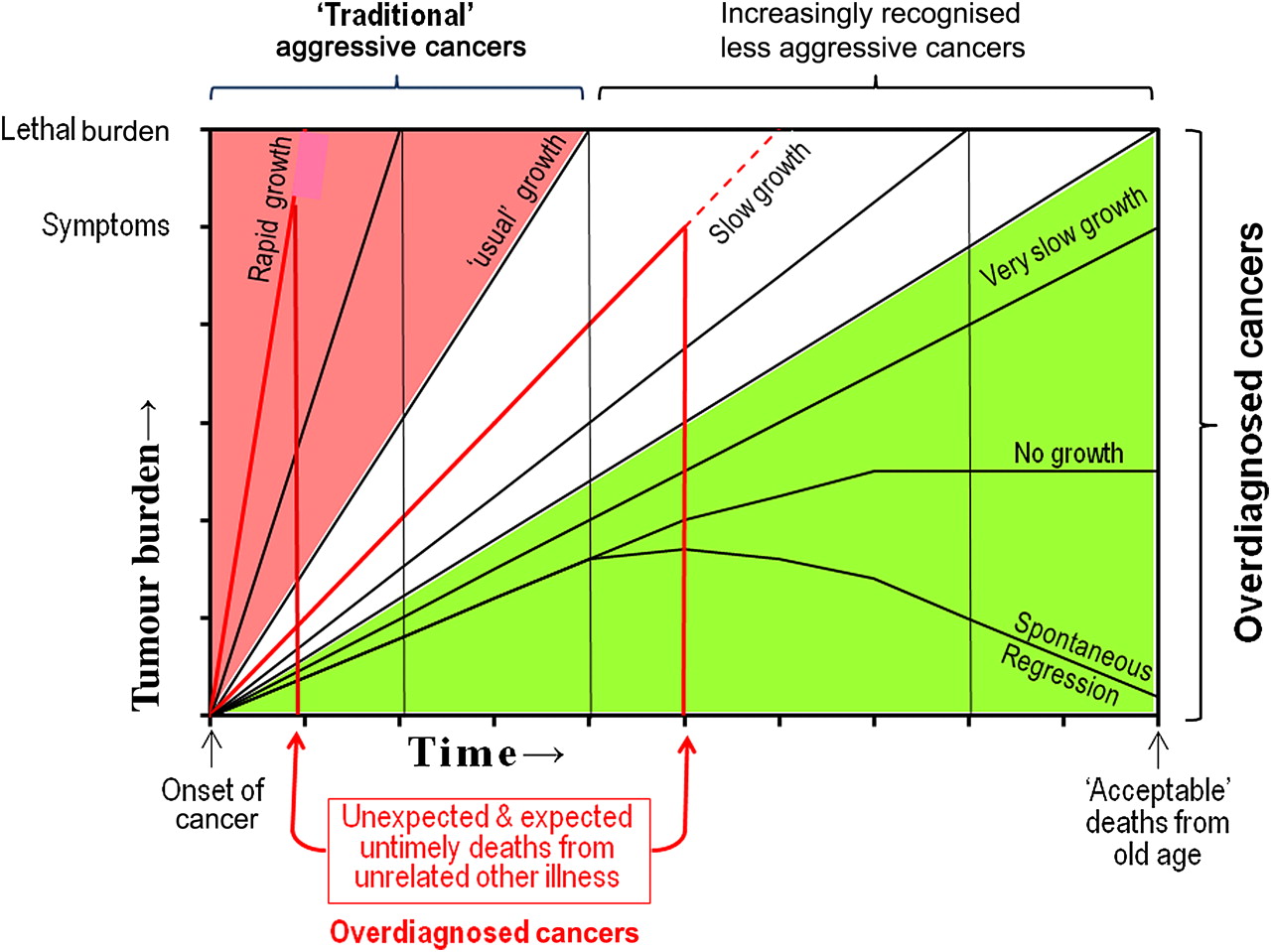
Limitations of a binary view of cancer and overdiagnosis. A cohort of less aggressive cancers is ignored by a binary view of cancer as either traditional (rapidly fatal) or overdiagnosed (allowing the patient to die of ‘natural causes’ even if untreated). Untimely non-cancer deaths (shown in red) are also ‘overdiagnosed’ regardless of aggressiveness of the cancer.
The crux of the problem is that the concept of overdiagnosis hangs on the cause of death, or actually more precisely the time of death. A patient diagnosed with cancer who dies at the point he/she is ‘destined’ to die has an overdiagnosed cancer; a patient who would have died of cancer but whose death is delayed because the cancer was diagnosed and treated is not overdiagnosed. Thus, implicit in the concept is the notion of time when a patient is destined to die, and that this can be altered for those destined to die of cancer. The concept assumes that treatment at preventing or delaying death from cancer is effective; by definition, a patient is classified as overdiagnosed if the treatment is ineffective, or if a decision is made not to treat, even though the patient dies of the cancer. A cancer is considered overdiagnosed even if treatment effectively palliates the symptoms but does not delay death.
The concept of overdiagnosis has value when looking retrospectively at a population that has already died; one can assess how often the diagnosis of cancer altered the time of death (with the assumption that effective treatment is available and has been given). However, the concept of overdiagnosis is not particularly useful for clinicians who are treating individual patients, not a population, and are looking forward with limited ability to determine when a patient is destined to die. Furthermore, combining all non-cancer deaths ignores substantial differences. An untimely death from an unexpected cause is, by definition, unpredictable and cannot influence decision making. An expected untimely death, however, can and should be taken into account when deciding whether to undergo screening (or treatment).
Changing cohorts
It is crucial to keep in mind that cancers exhibit a wide range of growth rates. We tend to think of the average rate, and not in a nuanced fashion of a spectrum of growth rates. Furthermore, we assume (with only limited data) that there is a relationship between growth rate and the propensity to invade locally, or to metastasise.
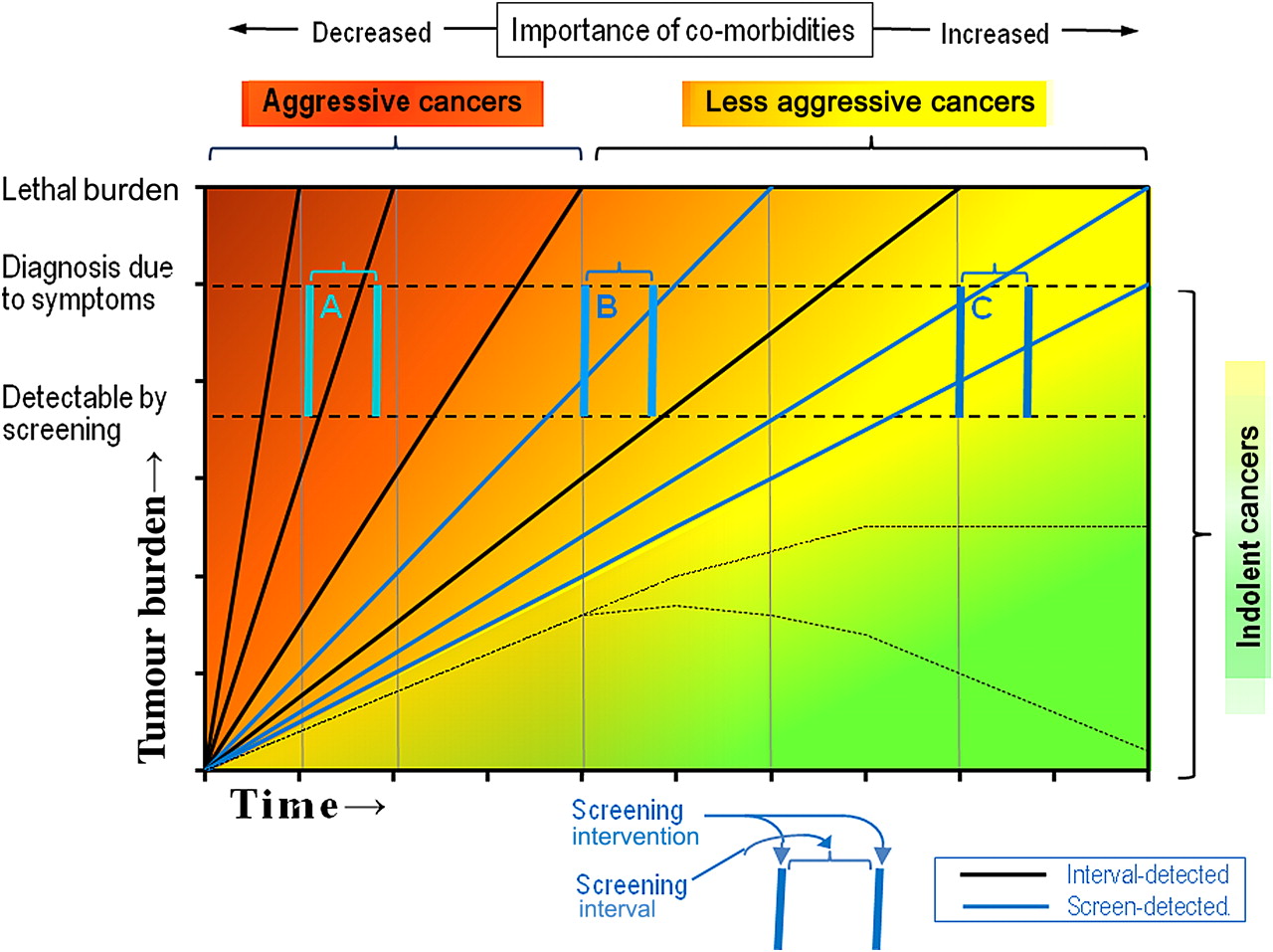
In addition, the spectrum of aggressiveness of detected lung cancer is changing over time.10 A screening intervention will disproportionately include more slow-growing tumours (known by the obscure term ‘length-time bias’, figure 3), because these exist for a longer time as detectable, yet asymptomatic tumours. Indeed, lung cancer screening studies have found more cancers, and a higher mean doubling time (136 days vs 486 days for routine care vs CT screening).10 This phenomenon is occurring generally (not just in screening programs) due the increase in CT imaging (from ∼13 000 000/year in 1990, to ∼60 000 000/year in 2005).11 ‘New’ entities such as adenocarcinoma-in-situ, or minimally invasive adenocarcinoma, are being recognised, with limited understanding of their biologic behaviour and potential for transformation into aggressive cancers.10 ,12
{kind=link}
{kind=link}
{kind=link}
Viewing cancers along a spectrum of aggressiveness. As the spectrum of aggressiveness of cancers decreases, the importance of co-morbid conditions increases. Shown in blue is how a screening intervention alters the cohort to include a greater proportion of slow-growing cancers. The degree to which this occurs is affected by the difference in tumour burden between symptom-detected and screen-detected cancers and the frequency of screening. Rapidly growing cancers (A) grow from an undetectable to a symptomatic state between screens; slow growing (B) and especially very slow growing cancers (C) are detected disproportionately more frequently by the screening test.
Co-morbidities have little impact for aggressive cancers. However, consideration of competing causes of death becomes increasingly important as the lung cancer cohort changes to include more slow-growing tumours, Furthermore, what constitutes appropriate treatment for aggressive versus ‘well-behaved’ cancers is probably different. This is fundamentally an issue of predicting biologic behaviour (which may not necessarily correlate with size at diagnosis, and our assumptions of a logarithmically constant growth rate may not be valid). Finally, as we peer into the future with respect to tumour behaviour and co-morbidities, we must consider that our ability to treat these conditions may change over time.
A proposed framework for discussion
To have a rational discussion we must avoid emotional reactions that inevitably prevent clear thinking. This is particularly important because we have to educate and engage a wider audience in the conversation. CT screening for lung cancer poses a particular challenge because it detects many non-malignant nodules and a greater proportion of slow-growing tumours, and because those with low risk but an elevated fear of the disease are more interested in the screening than those with high-risk lifestyles.13
The term ‘overdiagnosis’ is an oversimplification that does not serve us well to have an insightful discussion. Similarly, the word ‘cancer’ engenders such fear that we must actively work to embed new concepts in our consciousness. Furthermore, we need a framework to structure out thinking as we look forward with newly diagnosed individual patients (instead of looking retrospectively at a former population). We must embrace the concept that cancers have a wide spectrum of behaviour, and we must develop new terms to communicate this.
I propose the terms ‘indolent’, ‘less aggressive’, and ‘aggressive’ as adjectives to describe groups of cancers (figure 3). An ‘IDLE (InDolent Lesion of Epithelial origin) tumour’ is another name that has been suggested for indolent tumours.14 Although our ability to identify in which group a particular tumour falls is rudimentary, introduction of these concepts will help frame the discussion and, potentially, also result in more rational consideration of treatment options. These terms would allow us to ask nuanced questions about tumour behaviour over time, as opposed to the term ‘overdiagnosis’, which hampers this.
We must structure our thinking around relative risks of different outcomes (figure 3). We have always considered major factors and short-term outcomes (eg, the risk of treatment-related toxicity vs the chance of cure, or the impact of severe co-morbidities). However, with an increasing variety of treatment alternatives, a greater mixture of behaviour of lung cancers, and a greater ability to manage both lung cancer and other diseases over a longer period of time, we must develop tools and concepts that allow far more nuanced and complex judgement. We need tools that provide an estimate of a patient's prognosis relative to cancer or a co-morbid disease, a CI around the estimate, and an assessment of the chance that prognosis will be affected by unaccounted factors (eg, a new disease, or being struck by a bus). We must simultaneously learn to estimate the future as well as the degree of uncertainty in our ability to define it. Currently, we lack this capability, and it will be difficult to do, but it is needed to enhance our ability to make clinical judgements for patients.
We must devote more attention to understanding the biologic behaviour of tumours. In reality, a fair body of literature deals with the spectrum of aggressiveness of lung cancers and the effect of screening,10 ,12 ,15–22 although the data is indirect (ie, not from long-term observation without treatment). An impediment to understanding this data is the ingrained concept that lung cancers behave similarly, differing primarily by how early they are detected.23 There is clearly much work remaining to be done. However, we must first examine our assumptions and change our mental constructs in order to be able to forge ahead.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves