Article Text

Statistics from Altmetric.com
Even with postoperative thromboprophylaxis, 1% of patients will develop venous thromboembolism following elective arthroplasty. Of this number, 5% will suffer a fatal pulmonary embolism (PE).1 Where massive PE occurs causing right ventricular hypokinesis and shock, the mortality may be in excess of 30%.2 British Thoracic Society guidelines recommend thrombolysis for massive PE but, following major surgery, the risk of bleeding is significant and many clinicians would hesitate to expose their patient to this. Here we suggest a novel method for minimising the risks of systemic thrombolysis following limb surgery.
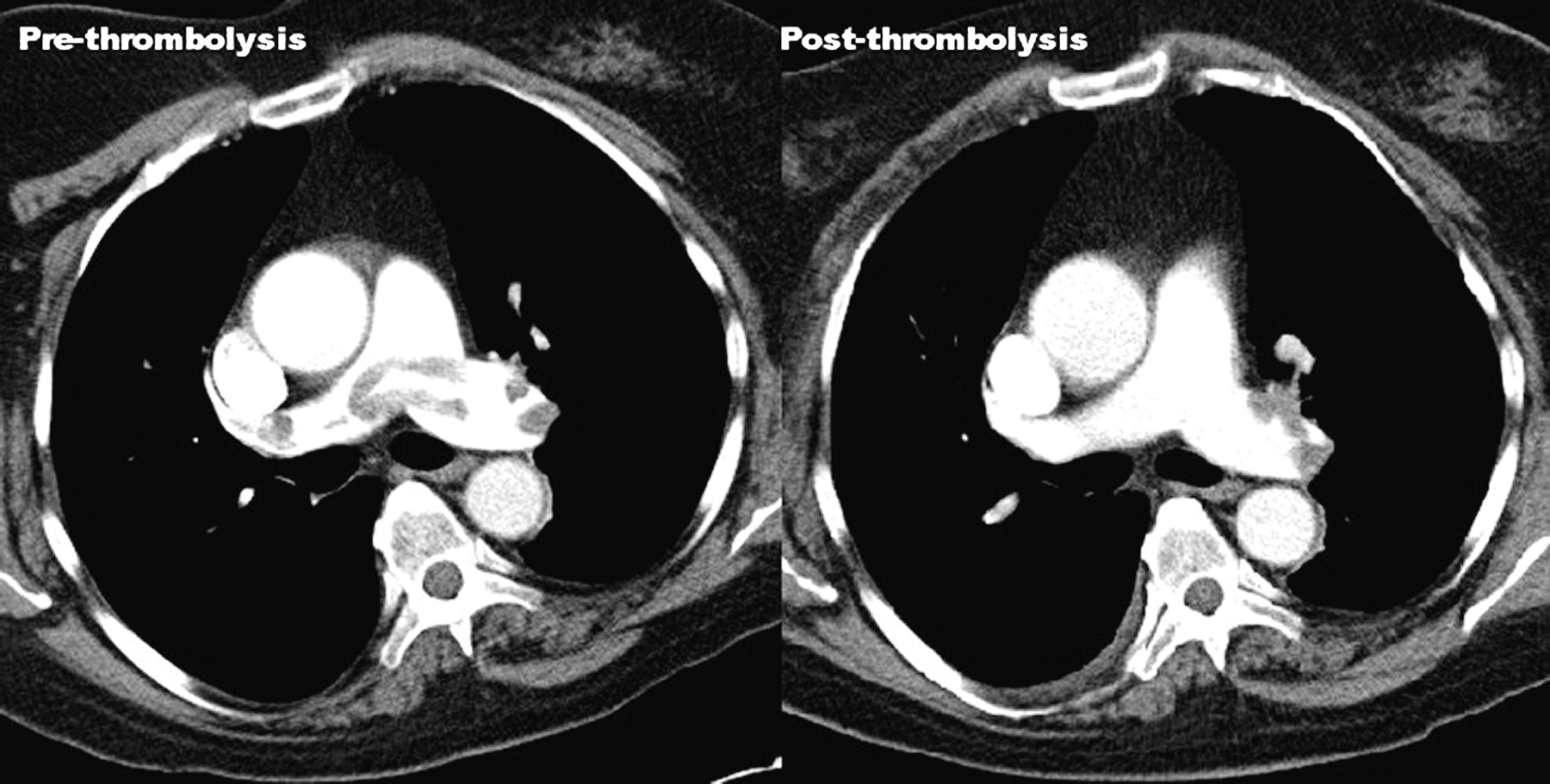
A 75-year-old woman presented with a large saddle pulmonary embolus demonstrated by CT pulmonary angiogram 5 days following knee replacement surgery. She was hypotensive and tachycardic. The echocardiogram showed that her right ventricle was dilated and hypokinetic. The patient was thrombolysed with 50 mg alteplase infused over 15 min, taking steps to preserve the postoperative limb. A tourniquet was applied to the limb to limit the proportion of the systemic thrombolytic agent that would reach the site of the surgery. A Cryocuff was used to cause vasoconstriction and reduce lactic acid formation. The tourniquet was inflated just before the infusion and was left on for 1 h. After thrombolysis the main complication was oozing of blood from the postoperative wound, but this settled with bandage compression. A CT pulmonary angiogram after 3 days showed that the saddle component of the embolus had dispersed (figure 1). She had made a good symptomatic recovery when reviewed in the clinic at 3 months and her echocardiogram showed a normally functioning right heart.

{kind=link}
CT pulmonary angiograms before and after thrombolysis.
The thigh tourniquet is a tool commonly used in orthopaedic surgery. An inflation time of 1 h was sufficient for the thrombolytic agent to be largely eliminated from the circulation. Alteplase was suitable in this situation because of its short plasma half-life of <5 min, although some plasminogen activator activity does persist for up to 4 h.3 Alternative therapies for massive PE include surgical embolectomy and intra-arterial thrombolysis. Both these techniques carry significant risks.4 Furthermore, their use is limited to specialist centres. Successful systemic thrombolysis following surgery has been reported, but this is frequently complicated by severe haemorrhage.5 Using the technique described, it was performed with minimal complications. Given the success in this case, we believe that major limb surgery no longer represents a contraindication to thrombolysis.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; not externally peer reviewed.