Article Text

Abstract
Obstructive sleep apnoea syndrome (OSAS) is a highly prevalent disease and is recognised as a major public health burden. Large-scale epidemiological studies have demonstrated an independent relationship between OSAS and various cardiovascular disorders. The pathogenesis of cardiovascular complications in OSAS is not completely understood but a multifactorial aetiology is likely. Inflammatory processes have emerged as critical in the pathogenesis of atherosclerosis at all stages of atheroma formation. Increased levels of various circulating markers of inflammation including tumour necrosis factor α (TNFα), interleukin 6 (IL6), IL-8 and C-reactive protein (CRP) have been reported as associated with future cardiovascular risk. There is increasing evidence of elevated inflammatory markers in OSAS with a significant fall after effective treatment with continuous positive airway pressure. This evidence is particularly strong for TNFα, whereas studies on IL6 and CRP have yielded conflicting results possibly due to the confounding effects of obesity. Cell culture and animal studies have significantly contributed to our understanding of the underlying mechanisms of the association between OSAS and inflammation. Intermittent hypoxia, the hallmark of OSAS, results in activation of pro-inflammatory transcription factors such as nuclear factor kappa B (NF-κB) and activator protein (AP)-1. These promote activation of various inflammatory cells, particularly lymphocytes and monocytes, with the downstream consequence of expression of pro-inflammatory mediators that may lead to endothelial dysfunction. This review provides a critical analysis of the current evidence for an association between OSAS, inflammation and cardiovascular disease, discusses basic mechanisms that may be responsible for this association and proposes future research possibilities.
Statistics from Altmetric.com
Obstructive sleep apnoea syndrome (OSAS) is characterised by instability of the upper airway during sleep resulting in markedly reduced (hypopnoea) or absent (apnoea) airflow at the nose/mouth. These episodes are usually accompanied by loud snoring and oxyhaemoglobin desaturation, and are typically terminated by brief arousals which result in marked sleep fragmentation and diminished amounts of slow wave and rapid eye movement (REM) sleep.1 Patients with OSAS are usually unaware of this sleep disruption, but the changes in sleep architecture contribute significantly to the prominent symptom of chronic daytime sleepiness found in these patients. The prevalence of OSAS among the adult population is high, being 4% in men and 2% of women in the Wisconsin Sleep Cohort Study.2 Given the rapidly rising incidence of obesity, which is the most important risk factor of OSAS, the prevalence is now likely to be significantly higher.3
The current management of moderate to severe OSAS is largely dependent on nasal continuous positive airway pressure (CPAP), which acts to splint the upper airway open during sleep and thus counteracts the negative suction pressure during inspiration that promotes upper airway collapse in these patients.4 5 Nasal CPAP completely controls the condition and has a dramatic effect on the patient’s awake performance because of the normalised sleep pattern.
OSAS is associated with significant morbidity and mortality. The excessive daytime sleepiness leads to impairments in quality of life, cognitive performance and social functioning.6 Furthermore, the disorder is associated with a 3–7-fold increase in the rate of road traffic accidents.7 The major health burden in patients with OSAS, however, is the strong risk of cardiovascular diseases such as systemic arterial hypertension, coronary artery disease, heart failure and stroke.8 The association between OSAS and cardiovascular diseases has been suggested for many years and, more recently, is corroborated by large-scale epidemiological and prospective studies. The underlying mechanisms mediating this association are incompletely understood. Current evidence suggests that inflammatory processes leading to endothelial dysfunction play a pivotal role in the pathogenesis.
Following a brief summary of the current epidemiological and clinical evidence of OSAS-associated cardiovascular involvement and an overview of inflammatory processes in the atherosclerotic process, this article provides a critical review of the current evidence of an association between OSAS and systemic inflammation, describes basic mechanisms that may be responsible for this association and outlines future research perspectives.
OSAS AND CARDIOVASCULAR DISEASES
An association between OSAS and the development of cardiovascular diseases has been suggested for several years. However, confounding variables such as obesity, hypertension, smoking, alcohol intake, age and level of exercise have made this independent relationship difficult to prove. Furthermore, many of the earlier studies on OSAS and cardiovascular diseases used samples from clinical populations which are usually not representative of the condition in the general population, and cannot be used to estimate the public health impact of the disease.3 However, the evidence of an association is growing, particularly with systemic arterial hypertension. Both the Sleep Heart Health Study which included over 6000 subjects and the Wisconsin Sleep prospective cohort study involving 1069 subjects have yielded convincing evidence of a modest but definite association, independent of possible confounding factors such as age, sex and obesity.9 10 The prevalence of OSAS is particularly high in patients with drug-resistant hypertension; a recent study found occult OSAS in up to 83% of patients who had uncontrolled hypertension despite taking three or more antihypertensive agents at optimum doses.11
Data linking OSAS to other cardiovascular diseases are not as clear-cut but, nonetheless, supportive. The strongest evidence is provided by data from the Sleep Heart Health Study cohort which reports an independent association between OSAS and congestive cardiac failure, cerebrovascular disease and coronary artery disease.12 In support, Peker et al followed patients with known coronary artery disease for 5 years and observed a significantly higher mortality in patients with an apnoea/hypopnoea index (AHI) of ⩾10/h in comparison with matched controls.13
A key question relates to the effect of CPAP therapy for OSAS on cardiovascular outcomes. Clearly, the ultimate answer to this question is still outstanding due to the lack of a long-term randomised trial. However, the withholding of effective CPAP therapy from patients with severe OSAS over a long period of time is unethical because of the recognised benefit of CPAP to daytime sleepiness and related symptoms in addition to the reduction in the risk of driving accidents. Three long-term cardiovascular outcome studies have compared patients on effective CPAP therapy with untreated or incompletely treated patients over 7–10 years and consistently found a significantly increased mortality and morbidity in the untreated group.14–16 However, patients intolerant of CPAP or unwilling to use the device do not represent a desirable control group as they may not be compliant with other medications. Randomised controlled studies looking at the effect of CPAP therapy on 24 h blood pressure in general have yielded modest but significant reductions in blood pressure, both during the night and day,17 18 and the beneficial effects were greatest in patients with pre-existing hypertension. Furthermore, there is now good evidence suggesting a beneficial effect of CPAP on left ventricular function. Two recent randomised trials have shown significant improvements in left ventricular ejection fraction following CPAP therapy for 1–3 months in patients with systolic congestive cardiac failure and OSAS.19 20
In summary, there is growing evidence of a causal link between OSAS and the development of cardiovascular diseases, and CPAP therapy potentially decreases cardiovascular morbidity and mortality. Given the high and steadily rising prevalence of OSAS, the clarification of its exact role as a cardiovascular risk factor is a major priority. Identification of the detailed mechanisms underlying cardiovascular disease in patients with OSAS will help to support the current epidemiological evidence.
These mechanisms are, so far, still poorly understood. The pathogenesis is likely to be a multifactorial process involving a diverse range of mechanisms including sympathetic excitation, endothelial dysfunction and metabolic dysregulation (fig 1).8 Current evidence suggests that inflammatory processes leading to endothelial dysfunction play a pivotal role in the pathogenesis. Endothelial dysfunction substantially contributes to the development of various cardiovascular disease processes, particularly atherosclerosis but also hypertension and congestive cardiac failure.
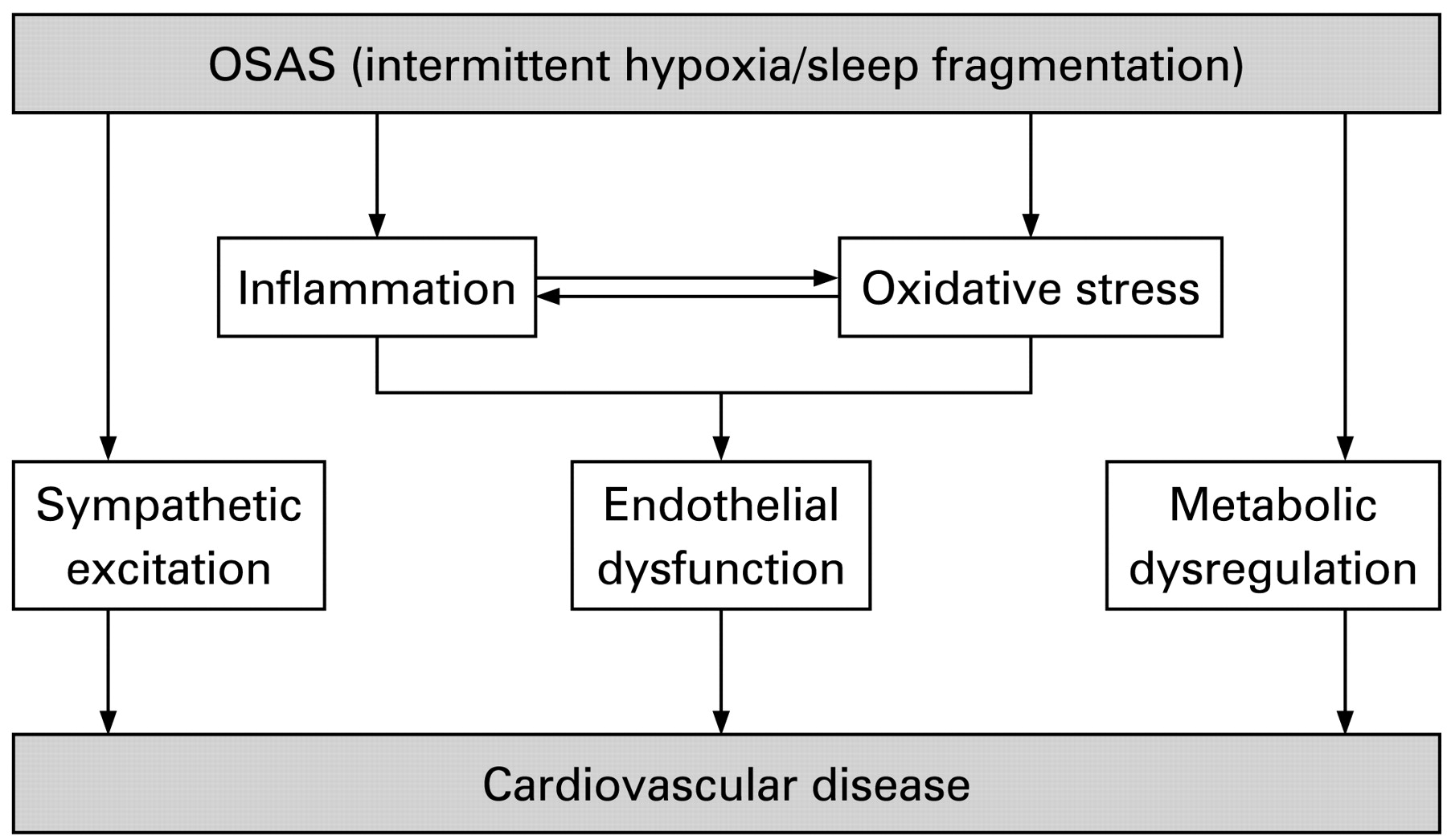
Mechanisms associated with obstructive sleep apnoea syndrome (OSAS) contributing to cardiovascular diseases.
INFLAMMATION AND ATHEROSCLEROSIS
Over the last several years we have seen major developments in our understanding of the pathogenesis of atherosclerosis. Inflammatory mechanisms have emerged as playing a pivotal role in all stages of atherosclerotic plaque formation, from initiation of the fatty streak to the culmination in plaque rupture presenting as acute coronary syndrome.21 22 Systemic inflammation occurs in the vasculature as a response to injury, lipid peroxidation and perhaps infection.23 24 Resident or circulating leucocytes mediate the adherence of monocytes to the endothelium which in turn release a number of inflammatory mediators including cytokines such as tumour necrosis factor α (TNFα) or interleukin (IL)-1, chemokines such as IL-8 or monocyte chemoattractant protein-1 (MCP-1) and adhesion molecules such as intercellular adhesion molecule 1 (ICAM-1) or selectins. Expression of adhesion molecules and chemokines facilitates the recruitment of macrophages, differentiated from monocytes, laden with oxidised lipid (foam cells). The accumulation of foam cells leads to the formation of a lipid pool, and collagen produced by smooth cells contributes to the strength of the fibrous cap. In particular, smooth cells also release IL6 which is the main hepatic stimulus for the acute phase reactant, C-reactive protein (CRP), which causes expression of adhesion molecules and mediates MCP-1 induction.25
EVIDENCE OF INFLAMMATION IN OSAS
Circulating inflammatory markers in OSAS
The importance of inflammatory processes in the pathogenesis of cardiovascular diseases in OSAS is strongly supported by numerous studies demonstrating raised levels of circulating pro-inflammatory cytokines, chemokines and adhesion molecules in patients with OSAS in comparison with matched controls, and a significant fall with effective CPAP therapy. In particular, the potent pro-inflammatory cytokine TNFα has been evaluated by several case-control studies that have consistently shown raised levels in patients with OSAS compared with controls, independent of obesity, and a significant fall with effective CPAP therapy; both T cells and monocytes have been suggested as potential sources.26–30 Recently, a large prospective study in men without cardiovascular diseases identified a strong association between OSAS severity and TNFα levels, independent of possible confounders such as body mass index (BMI), age or sleepiness.29 Levels of the chemokine IL-8, which plays a key role in the process of adhesion of neutrophils and monocytes to the vascular endothelium,31 32 have also been shown to be raised in OSAS.29 33 Earlier studies have suggested increased IL6 levels in patients with OSAS,26 34 35 but some of these reports may have been limited by smaller numbers, lack of adequately matched normal control populations, particularly in terms of BMI, and the inclusion of patients with established cardiovascular or metabolic diseases. Recent studies did not detect an association between OSAS and IL6.29 36 However, in a large cross-sectional analysis of the Cleveland Family Study there was an independent association between OSAS severity parameters and soluble IL6 receptor,36 which appears to be associated with the processes of inflammation and myocardial injury during the acute phase of acute myocardial infarction.37
A limited number of studies have also examined the levels of various cellular adhesion molecules such as intercellular adhesion molecule 1 (ICAM-1), vascular adhesion molecule 1 (VCAM-1) and the family of selectins. The results consistently suggest an association between OSAS severity and circulating levels of cellular adhesion molecules, with one report also showing a significant fall after 1 month of effective CPAP therapy.38–42
Another potential link between OSAS and inflammation is the acute phase reactant C-reactive protein (CRP). In the high to normal range, when measured with a high-sensitivity assay, CRP levels are widely recognised as potent predictors of future cardiovascular events in apparently healthy subjects43 44 as well as in subjects with known cardiovascular disease.45 46 However, recent large-scale studies suggest that the elevated levels may, in fact, be attributable to the presence of abnormal conventional cardiovascular risk factors, particularly obesity.47–49 The strong relationship between CRP levels and obesity has also influenced various studies investigating CRP levels in adults with OSAS, and therefore the role of CRP in OSAS is still under debate. This is reflected, for instance, in different conclusions obtained from two large cross-sectional studies in patients with OSAS. A study on 316 Japanese men detected a significant association between CRP and sleep-disordered breathing; however, the use of overnight oximetry as a screening tool for OSAS was a significant limitation.50 On the other hand, the Wisconsin Sleep Cohort Study involving 907 adults failed to detect an independent association between CRP and OSAS after adjustment for BMI.51 This discrepancy has also been evident in numerous case-control studies where some reports have identified increased levels of CRP in patients with OSAS34 52–54 and others did not.55–57 Furthermore, the impact of CPAP therapy on CRP levels is still unclear.34 57–59 In a recent randomised trial comparing therapeutic and subtherapeutic CPAP, effective OSAS treatment had no significant effect on levels of CRP or IL6.60
It is noteworthy that the role of increased inflammatory markers in the prediction of cardiovascular morbidity in OSAS is still unclear and long-term prospective studies on this subject are lacking. Furthermore, vascular inflammation leading to endothelial dysfunction may potentially occur and persist in the absence of a systemic inflammatory response. A recent study provides evidence of increased expression of the inflammatory markers inducible nitric oxide synthase (iNOS) and cyclooxygenase-2 (COX-2) in harvested venous endothelial cells of patients with OSAS compared with matched controls, together with evidence of altered endothelial repair capacity that was reversed by CPAP therapy.61 However, whether these alterations are associated with a detectable systemic inflammation is unknown.
Inflammatory cells and interactions with the endothelium in OSAS
Accumulation of leucocytes and their adhesion to the endothelium play a central role in the formation of atherosclerotic plaques. Activation of monocytes and T lymphocytes is among the crucial steps leading to the release of inflammatory mediators and adhesion molecules.
Activation of inflammatory cells and their interaction with endothelial cells have been demonstrated in OSAS. In a rat model, recurrent obstructive apnoeas led to a significant increase in various leucocyte-endothelial cell interactions such as leucocyte rolling and firm adhesion of leucocytes in comparison with a sham group.62 Monocytes of patients with OSAS adhere more firmly to endothelial cells than those of control subjects, a process that is decreased by the application of CPAP therapy.63 In the same study, OSAS was associated with the upregulation of the adhesion molecules CD15 and CD11c in monocytes. Furthermore, in a cell culture model of repetitive hypoxia and reoxygenation, lipid uptake into macrophages and the expression of various adhesion molecules were significantly increased in comparison with control cells.64 Further evidence is provided in the report by Minoguchi et al who demonstrated significantly higher spontaneous TNFα production by monocytes in patients with OSAS than in matched controls.30
T lymphocytes are also involved in the pathogenesis of atherosclerosis. In a series of experiments, Dyugovskaya et al showed that various subpopulations of cytotoxic T cells of patients with OSAS acquire an activated phenotype with the downstream consequence of increased cytotoxicity against endothelial cells.27 65 66 Furthermore, this activation process is associated with an increased intracellular content of the pro-inflammatory mediators TNFα and IL-8 and a decrease of the anti-inflammatory cytokine IL-10.27
A recent in vitro study addressed the involvement of neutrophils in the cardiovascular pathogenesis of OSAS.67 The results demonstrate impaired neutrophil apoptosis and increased adhesion molecule expression by these cells in OSAS, thus suggesting a further potential pathway in the atherosclerotic process.
MECHANISMS OF INFLAMMATORY PROCESSES IN OSAS
The basic mechanisms underlying the inflammatory process in OSAS remain unclear. In addition to sleep fragmentation and sleep deprivation, the unique form of hypoxia in OSAS—with repetitive short cycles of desaturation followed by rapid reoxygenation, termed intermittent hypoxia (IH)—is likely to play a significant role in the initiation of the inflammatory process. Various effects of IH on the cardiovascular system have been demonstrated using animal models. Rat and dog models of IH have consistently reported an increase in arterial blood pressure which is sustained even after cessation of the stimulus.68 69 Furthermore, enhanced sympathetic activity and decreased baroreflex sensitivity have been proposed to lead to the blood pressure increase in these models.70–72
There are various animal models supporting the development of atherosclerosis in response to IH.73 74 In mice on a high-cholesterol diet, IH led to the development of atherosclerotic lesions which was not observed in control animals that were not exposed to IH.73 Furthermore, cardiovascular remodelling with altered adhesion molecule expression has been observed in mice exposed to 14 days of IH. Interestingly, the right heart was not affected in this model whereas both the left ventricle and aorta demonstrated these changes.74
We recently showed in a cell culture model of IH a preferential activation of inflammatory pathways mediated by the transcription factor nuclear factor kappa B (NF-κB) over adaptive hypoxia-inducible factor 1 (HIF-1)-dependent pathways, which contrasts with sustained hypoxia where activation of adaptive and protective pathways predominate.28 NF-κB is a key player in inflammatory and innate immune responses and a master regulator of inflammatory gene expression, and genes such as TNFα or IL-8 that are important to the atherosclerotic process and which have also been found upregulated in OSAS are under the control of this transcription factor. The central role of NF-κB in inflammatory processes in OSAS was furthermore suggested by increased activation in cardiovascular tissues in a mouse model of IH and also in cultured monocytes of patients with OSAS.75 76 The p38 mitogen-activated protein kinase (MAPK) plays a major role in the process of IH-induced NF-κB activation, and pharmacological as well as targeted siRNA inhibition of p38 leads to a significant reduction in NF-κB activity.77 p38 MAPK is a key player in inflammatory processes and is necessary for inflammatory cytokine production and signalling.78 Furthermore, p38 is activated in response to environmental stresses and is critically involved in the pathophysiology of a variety of cardiovascular diseases.79–84 Activation of p38 MAPK was also demonstrated in a rat model of IH which was associated with delayed cardioprotection against prolonged ischaemia.85
Although our cell culture model demonstrates preferential activation of inflammatory over adaptive pathways by IH,28 more prolonged exposure to IH may activate HIF-1, and this finding has been reported in another cell culture model86 and in a mouse model of IH.87 In particular, Yuan and co-workers reported increased HIF-1 transcriptional activity in response to 60 and 120 cycles of IH but not with fewer cycles.86
IH also activates other inflammatory transcription factors. Among them is the activator protein complex-1 (AP-1), formed by the proteins c-Fos and c-Jun. AP-1 drives transcriptional activation of a variety of genes including tyrosine hydroxylase which encodes the key enzyme in catecholamine synthesis.88 c-Fos upregulation by IH has been demonstrated in an animal as well as in a cell culture model.86 89 In a rat model, activation of inflammatory pathways by IH was associated with an impairment of neurocognitive function, a process which was reversed once the stimulus was removed.90
Yet to be determined remain(s) the initial sensing and signalling event(s) which occur(s) in response to IH. It has been proposed that repetitive episodes of hypoxia—and particularly of reoxygenation—lead to an increased production of reactive oxygen species (ROS).91 In support of this proposal, increased circulating levels of markers of oxidative stress have been found in patients with OSAS, and in vitro studies have demonstrated increased ROS production from leucocytes of patients with OSAS which was reversed by CPAP therapy.63 However, the involvement of ROS in NF-κB signalling is controversial, and experiments by Hayakawa et al indicate that NF-κB is unlikely to be a sensor of oxidative stress and previous results may have been influenced by cell type dependency and methodological limitations.92 In support of this, we did not detect an influence of the ROS scavenger N-acetyl-L-cysteine on NF-κB activation by IH in our cell culture model (unpublished data).
Collectively, the available evidence indicates that activation of inflammatory transcription factors, particularly NF-κB, by IH is critical in the pathogenesis of atherosclerosis in patients with OSAS.
INTERACTION WITH OBESITY
It is important to distinguish the inflammatory responses directly related to OSAS from obesity-related inflammation. Obesity, particularly visceral adiposity, is associated with chronic low-grade inflammation, as indicated by increased levels of the inflammatory markers CRP and IL6 in the circulation of obese subjects.93 Adipose tissue produces and releases a variety of pro-inflammatory and anti-inflammatory factors, including the adipokines leptin, adiponectin and resistin, as well as cytokines and chemokines such as IL6, TNFα, monocyte chemoattractant protein 1 (MCP-1) and others. These molecules produced by adipose tissue have been implicated as active participants in the development of insulin resistance and cardiovascular diseases.94 Thus, both obesity and OSAS are pro-inflammatory conditions and may mutually enhance the progression and severity of cardiovascular diseases.
FUTURE RESEARCH PERSPECTIVE
While substantial progress has been made in the identification of inflammatory processes in the cardiovascular pathogenesis of OSAS, a significant number of questions remain unanswered. The impact of CPAP therapy on cardiovascular diseases in OSAS has not been fully investigated, but may prove difficult to answer as a long-term randomised trial faces ethical problems. Understanding the basic molecular mechanisms of cardiovascular complications in OSAS can help to fill the gap of missing epidemiological evidence and, therefore, research in this field should be a major priority. Few translational studies have been undertaken so far that have explored basic mechanisms of cardiovascular diseases in OSAS with application of the findings to the clinical setting. Many of the clinical studies looking at inflammatory markers in OSAS have been influenced by small numbers, inadequately matched populations (particularly for BMI) and inclusion of patients with established cardiovascular or metabolic diseases. It is thus not surprising that conflicting results have been reported.
There is therefore a clear need for large-scale multicentre studies of carefully defined patient and control populations. Such studies carry the prospect of evaluating potential interactions between different basic mechanisms and cardiovascular disease and providing potential treatment options. As this review outlines, the basic inflammatory mechanisms underlying cardiovascular complications in OSAS are complex. There is emerging evidence that IH plays a central role in the initiation of the inflammatory processes, but additional studies involving cell, animal and human models are required to adequately explore the mechanisms involved.
CONCLUSIONS
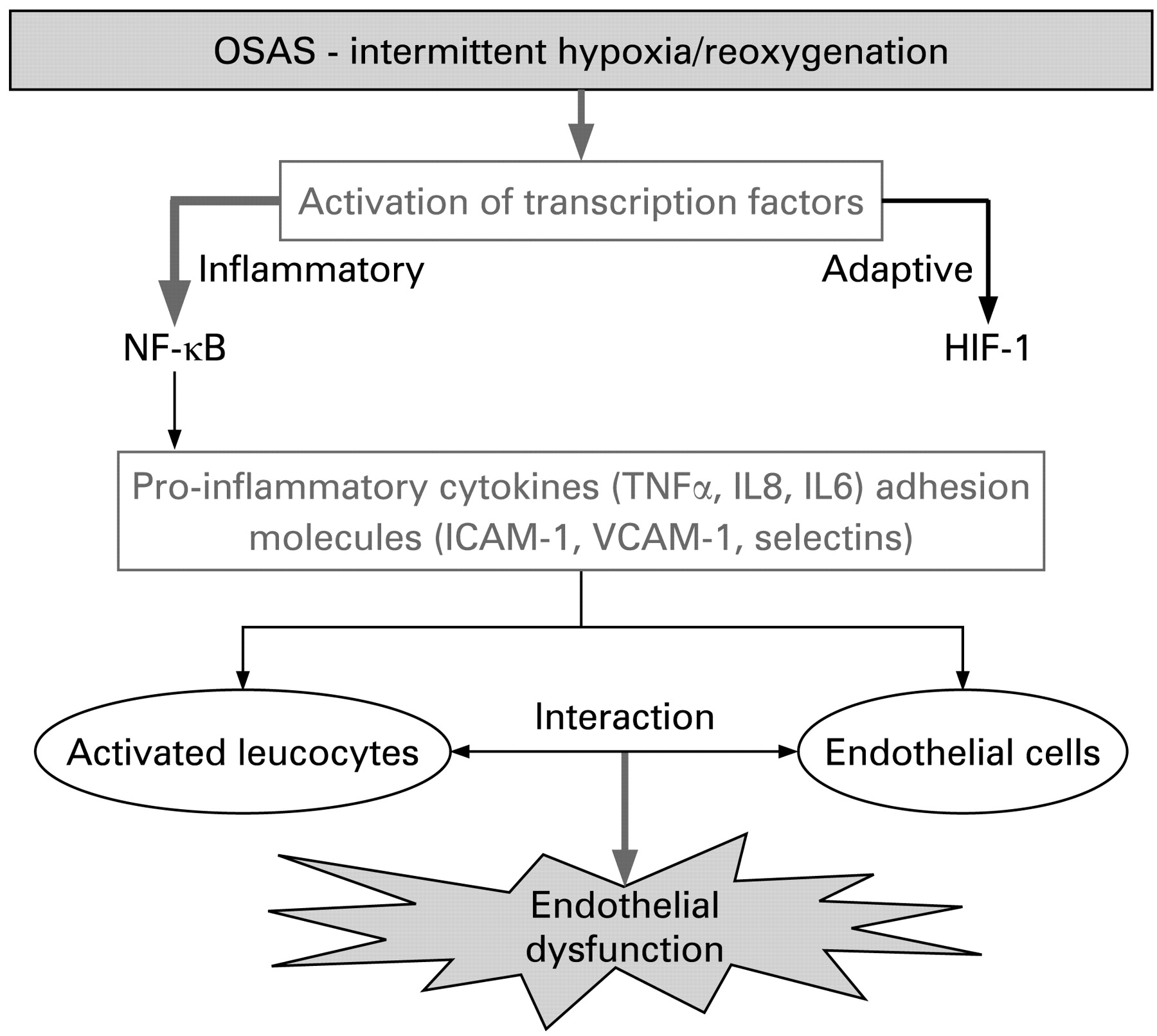
Inflammatory processes are rapidly emerging as playing a central role in the cardiovascular pathogenesis of OSAS. The repetitive cycles of short periods of hypoxia followed by rapid reoxygenation preferentially activate inflammatory—particularly NF-κB-mediated—pathways. These mechanisms result in activation of inflammatory cells, release of inflammatory mediators and associated vascular pathophysiology (fig 2). Future therapeutic approaches to ameliorating the cardiovascular risk factors associated with OSAS should take into account the possibility of inhibiting systemic inflammatory processes.
{kind=link}
{kind=link}
Selective activation of inflammatory pathways by intermittent hypoxia. Intermittent hypoxia leads to a preferential activation of nuclear factor kappa B (NF-κB)-dependent inflammatory pathways over adaptive hypoxia-inducible factor 1 (HIF-1) mediated pathways. This results in the production of various pro-inflammatory mediators which, in turn, mediates the interaction of inflammatory and endothelial cells resulting in endothelial dysfunction. ICAM-1, intercellular adhesion molecule 1; IL, interleukin; OSAS, obstructive sleep apnoea syndrome; TNFα, tumour necrosis factor α; VCAM-1, vascular adhesion molecule 1.
REFERENCES
Footnotes
Funding: Health Research Board (Ireland), Science Foundation of Ireland, Wellcome Trust
Competing interests: None.