Article Text

Abstract
Background: Childhood obstructive sleep apnoea (OSA) is suggested to be associated with cardiac structural abnormalities and dysfunction but existing evidence is limited and the treatment effect on echocardiographic outcome remains controversial.
Objective: To examine the presence of subclinical cardiac abnormalities in childhood OSA and the effects of treatment on cardiac changes.
Methods: Polysomnography (PSG) and echocardiographic examinations were performed in 101 children aged between 6 and 13 years who were invited from a community based questionnaire survey. They were classified into a reference group (apnoea–hypopnoea index (AHI) <1, n = 35), mild OSA group (AHI 1–5, n = 39) and moderate to severe group (AHI >5, n = 27) based on the PSG results. Treatments, including adenotonsillectomy or nasal steroids, were offered to the mild and moderate to severe OSA groups.
Results: The moderate to severe OSA group had greater right ventricular (RV) systolic volume index (RVSVI), lower RV ejection fraction (RVEF) and higher RV myocardial performance index (RVMPI) than the reference group. They also had more significant left ventricular (LV) diastolic dysfunction and remodelling with larger interventricular septal thickness index (IVSI) and relative wall thickness than those with lower AHI values. The moderate to severe OSA group had an increased risk of abnormal LV geometry compared with the reference group (odds ratio 4.21 (95% CI 1.35 to 13.12)). Log transformed AHI was associated with RVSVI (p = 0.0002), RVEF (p = 0.0001) and RVMPI (p<0.0001), independent of the effect of obesity. Improvement in RVMPI, IVSI and E/e′ were observed in those with a significant reduction in AHI (>50%) comparing 6 month with baseline data.
Conclusions: OSA is an independent risk factor for subclinical RV and LV dysfunction, and improvement in AHI is associated with reversibility of these abnormalities.
Statistics from Altmetric.com
Childhood obstructive sleep apnoea (OSA) is being increasingly recognised and its prevalence among the paediatric population is reported as 2–4%.1 Early studies on childhood OSA demonstrated that severe disease could lead to congestive heart failure.2 3 More recent reports have documented the presence of subclinical forms of cardiac/ventricular dysfunction in children with OSA.4–7 However, these paediatric studies were limited by their small sample size and lack of normal children as controls. All cases included in these studies were recruited from hospital attendants which may not truly reflect the situation in the community. Furthermore, the effect of intervention for OSA on cardiac dysfunction has not been well characterised. Preventing the development of subclinical cardiac abnormalities may be important as current evidence suggests asymptomatic ventricular dysfunction predicts future cardiovascular events.8 9 The aims of this study were to assess cardiac structure and function in an OSA cohort recruited from the community and to measure the degree of reversibility following interventions.
METHODS
Subjects and study design
Subjects for this study were drawn from our ongoing childhood OSA epidemiological study which involved children aged between 6 and 13 years recruited from 13 randomly chosen schools. A total of 6447 schoolchildren had completed a validated OSA screening questionnaire10 that stratified them into high (n = 586) or low (n = 5861) risk for OSA. All children classified as high risk by the questionnaire were invited, and subjects classified as low risk were randomly chosen and invited for overnight polysomnography (PSG) and cardiac assessment. A total of 410 high risk and 209 low risk children agreed to participate. Children were excluded from the study if they had an intercurrent upper respiratory tract infection within 4 weeks of PSG, suffered from neuromuscular disorder, craniofacial anomalies, syndromic disorder or if they had previously undergone upper airway surgery. Anthropometric parameters, including weight, height, waist and hip circumferences, and casual systolic and diastolic blood pressure were measured (Datascope Accutorr Plus) on the day of PSG. Two blood pressure measurements were taken with a 5 min interval and the average of the two readings was used for analysis. Body mass index (BMI) was translated to BMI z scores according to the normal reference values of Hong Kong Chinese children.11 This project included the first 101 consecutive children who gave consent for overnight PSG and echocardiographic examination (ECHO).
All children were referred for otorhinolaryngological assessment before their PSG. For those who were diagnosed as having OSA based on PSG, adenotonsillectomy was offered. Those who refused surgical intervention or where surgery was thought not to be indicated based on predetermined criteria (small tonsils; tonsils do not extend beyond the anterior tonsillar pillar and small adenoids; adenoids which occupy less than 25% of the post-nasal space with minimal OSA symptoms or poorly controlled allergic rhinitis with supine nasal obstruction) were offered nasal corticosteroid therapy (mometasone 100 μg/day for 6 months)12 and/or non-invasive positive pressure ventilation. These subjects then underwent repeat PSG and ECHO 6 months after the operation or start of therapy. Children with OSA who refused any form of therapy were also invited to return at 6 months for a repeat assessment. Informed consent from the parents or legal guardian and verbal assent from each child were obtained. The study was approved by the institutional ethics committee.
Polysomnography
Children recruited into the study underwent at least one standard overnight PSG at a dedicated sleep laboratory with CNS 1000P polygraph (CNS; Chanhassen Minnesota, USA). The central and occipital electroencephalogram, bilateral electrooculogram, submental electromyogram, bilateral leg electromyogram and electrocardiogram were recorded. The positions of the subject, respiratory airflow (nasal cannula connected to pressure transducer), respiratory efforts (strain gauge), arterial oxyhaemoglobin saturation (Spo2, Ohmeda 3700 pulse oximeter, measured by finger sensor, averaging time 3 s) were measured. In this study, we scored the presence of both apnoeas and hypopnoeas. Briefly, obstructive apnoea was defined as absence of airflow with persistent respiratory effort lasting longer than two baseline breaths, irrespective of Spo2 changes. Obstructive hypopnoea was defined as reduction of airflow of 50% or more with persistent respiratory effort lasting longer than two baseline breaths and associated with oxygen desaturation of at least 4% and/or arousals. The apnoea–hypopnoea index (AHI) was the total number of obstructive apnoeas or hypopnoeas per hour of sleep. Oxygen desaturation index (ODI) was defined as the total number of dips in arterial oxygen saturation ⩾4% per hour of sleep. Arousal was defined as an abrupt shift in electroencephalogram frequency during sleep, which may include theta, alpha and/or frequencies greater than 16 Hz but not spindles, of 3–15 s in duration. In REM sleep, arousals were scored only when accompanied by concurrent increases in submental electromyogram amplitude. Arousal index (ArI) was defined as the number of arousals per hour of sleep. OSA was defined if AHI ⩾1 per hour of sleep.13
Echocardiography
ECHO studies were performed using the Vivid 5 system (Vingmed-General Electric, Horten, Norway). The examiner was blinded to the subject’s PSG results and therefore group allocation. Left ventricular (LV) volumes and ejection fraction (EF) were assessed by biplane Simpson’s equation using the apical four chamber and two chamber views where the length of the ventricular image was maximised. LV mass was measured by Devereux’s method, as previously described.14 LV mass was divided by subject’s height to the power of 2.7 to provide LV mass index (LVMI). LV hypertrophy was defined as an LVMI greater than the 95th percentile of healthy controls (38.6 g/m2.7) that was previously reported.15 Relative wall thickness (RWT) of the LV, a measure of concentricity, was calculated as the sum of the thickness of the posterior and septal wall divided by LV diastolic diameter. A RWT of greater than the 95th percentile of age matched healthy controls (0.375) that was previously reported was used as the cut-off to define concentric LV geometry.16 LV geometry was classified as normal, concentric remodelling, eccentric hypertrophy or concentric hypertrophy, as described by Ganau and colleagues.17 Right ventricular end systolic (RVSVI) and end-diastolic volume index to height (RVDVI) and the right ventricular ejection fraction (RVEF) were calculated from apical four chamber views, using the area–length method (RV volume = 3/8π [area2/length]). Any significant valvular lesion was examined with haemodynamic assessment made. In children with tricuspid regurgitation, a spectral Doppler profile was used to estimate pulmonary artery systolic pressure from the sum of the modified Bernoulli equation (velocity2×4) product and estimated right atrial pressure. Diastolic function was measured for both ventricles by measuring the ratio of the peak early diastolic (E) and peak atrial (A) velocity from pulse Doppler data from the tricuspid and mitral valves. LV and RV myocardial performance index (MPI) of both ventricles were defined by the sum of isovolumic contraction and relaxation times divided by ejection time obtained from pulse Doppler data. LV filling pressure was approximated from the relationship E/e′ where E is the pulse wave Doppler velocity of the mitral valve and e′ is the pulse wave tissue Doppler velocity of the septal annulus.
Statistical analysis
All parametric and non-parametric data are expressed as mean (SD) and median (IQR), respectively. Parametric and non-parametric data were compared using one way analysis of variance (ANOVA) and the Kruskal–Wallis test, respectively. For parametric data, the Tukey or Games–Howell method was used for post-hoc pairwise comparisons with adjustments made depending on the agreement of the assumption of variance. For non-parametric data, the Mann–Whitney U test with adjusted p values (significant at p<0.016) were used for pairwise comparisons. The χ2 test was performed to investigate the difference in proportions between groups. Further χ2 tests with adjusted p values (p<0.016) were used for pairwise comparisons.
Multiple linear regression analyses were performed to assess the relationship between PSG variables and ECHO measures, while controlling for possible confounders. As some of the PSG data were skewed and contained zero values, these variables were log transformed using special formula (natural log [x+0.1]).
Logistic regression analyses were performed to estimate the odds ratios (OR) for abnormal LV geometry for different severities of OSA compared with the reference group while adjusting for possible confounding factors.
For the follow-up study, subjects were divided into two groups for comparison. One group consisted of subjects who had improvement in their OSA, as defined by >50% reduction in AHI from baseline to follow-up.18 The other group consisted of subjects who had persistent or worsened OSA (<50% reduction in AHI). Wilcoxon signed ranks tests were used to examine the intragroup differences between baseline and follow-up. Mann-Whitney U tests were used to detect the between group differences at baseline, at follow-up and the changes during the treatment period. All analyses were performed using SPSS V.13.0.
RESULTS
Study population
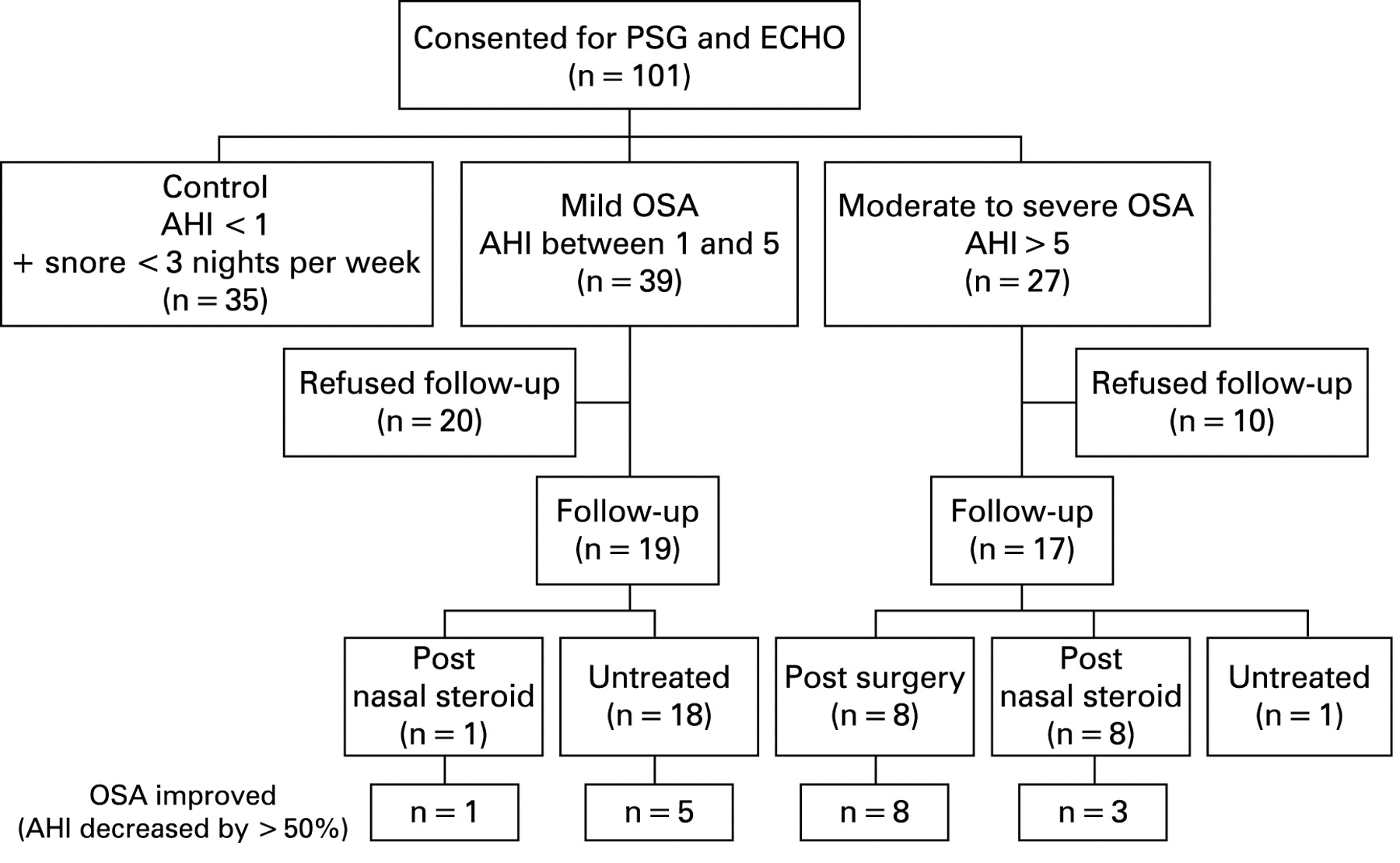
The children were divided into a reference group (AHI <1 and snoring for <3 nights per week, n = 35), mild OSA group (AHI 1–5, n = 39) and moderate to severe OSA group (AHI >5, n = 27) (fig 1). The demographics, anthropometric and PSG data for the groups are shown in table 1, and there were no significant differences in demographic or anthropometric parameters except for BMI z score. Significant differences were found in AHI, ODI, ArI and Spo2 nadir between the groups.

ECHO findings of cardiac structure and function
Right ventricle
RVSVI, RVEF and RVMPI were all significantly different between the three groups. The reference group had a significantly smaller RVSVI and higher EF than both the mild and moderate to severe OSA groups. For RVMPI, the post hoc test showed that the moderate to severe group had a significantly greater value than the mild and reference groups (table 2). No significant tricuspid regurgitation was noted in any of the children.
Multiple linear regression analysis showed that log transformed AHI and log transformed ODI were significantly associated with RVSVI (p = 0.0002), RVEF (p = 0.0001) and RVMPI (p<0.0001) after adjustment for age, gender and BMI z score (table 3).
Left ventricle
RWT and the interventricular septal thickness index to height (IVSI) were significantly higher in the moderate to severe group compared with the mild group (table 2). A similar trend was observed for LVMI although subgroups comparison showed no significant difference. The moderate to severe group also had a greater proportion of subjects having abnormal LV geometry compared with the mild and reference groups. For diastolic function parameters, E/e′, a marker of LV filling pressure, increased with increasing severity of OSA.
Multiple linear regression analysis showed that log transformed ODI were significantly associated with IVSI (p = 0.016) after adjustment for age, gender and BMI z score. The results also showed that the adjusted association between log transformed AHI and E/e′ was nearly significant (p = 0.050) (table 3).
Multivariate logistic regression analyses were used to examine whether the severity of OSA was associated with the presence of abnormal LV geometry. The risk of abnormal LV geometry was 4.29 times (OR 4.29 (95% confidence interval (CI) 1.43 to 12.81), p = 0.009) higher for the moderate to severe group compared with the reference group before adjusting for any confounders. The OR was reduced but remained significant after adjustment for age, gender and BMI z score (OR 4.21 (95% CI 1.35 to 13.12), p = 0.013). Such an increased risk was not found in the mild OSA group.
Treatment effect
Thirty out of 66 OSA subjects refused to have follow-up assessment. Of the remaining 36 OSA subjects, eight had adenotonsillectomy and nine received nasal steroid therapy. No child opted to receive non-invasive positive pressure ventilation in our study. The remaining 19 subjects refused any form of treatment but agreed to have follow-up assessment (recruitment details are described in fig 1). Their characteristics, including anthropometrics, PSG and ECHO parameters were not significantly different from those who did not return for reassessment. At follow-up, 17 had improved OSA, as reflected by their AHI decrement of ⩾50% (improved OSA group).18 The remaining (n = 19) were classified as persistent OSA group.
Significant reductions in RVMPI, IVSI, and E/e′ from baseline to follow-up 6 months later were noted only in the improved OSA group (table 4). Changes in RWT and E/e′ from baseline were significantly different between the improved OSA group and the persistent OSA group (table 4). Furthermore, change in AHI was positively associated with changes in RVMPI (Spearman’s rho (r) = 0.448, p = 0.006), IVSI (r = 0.429, p = 0.009), RWT (r = 0.433, p = 0.008) and E/e′ (r = 0.502, p = 0.002) (fig 2). These changes in ECHO parameters were not significantly associated with change in BMI z score.

{kind=link}
{kind=link}
DISCUSSION
In this study, we were able to document RV and LV dysfunction and remodelling in a cohort of community based children with OSA. The AHI was demonstrated to be a significant independent parameter associated with cardiac dysfunction. Following effective treatment for OSA, the cardiac abnormalities improved whereas in the group with persistent OSA, the abnormalities showed no improvement. These findings are important because children who are otherwise healthy have end organ involvement with RV and LV structural and functional abnormalities similar to those that have been associated with other diseases,19 20 such as hypertension. In adults, evidence supports the fact that abnormalities detected in ECHO, even in asymptomatic patients, predict future cardiovascular events.8 9 Regression of these cardiac abnormalities with treatment is associated with a decrease in cardiovascular morbidity, including atrial fibrillation, heart failure and hospitalisation.21 22
There are disparate conclusions of previous studies on the effect of OSA on RV function and enlargement.4 23–25 Sanner et al has shown that OSA was independently associated with depressed RVEF by radionuclide ventriculography.23 In other studies, RV dimensions and RV systolic function measured by ECHO were not shown to be significantly different between subgroups with varying OSA severity.23 24 A possible explanation for the discrepancy is that previous studies were in subjects with varying degrees of obesity recruited from hospital attendants. Obesity is an important risk factor of OSA in adults and children,26 and it is well established that obesity and its metabolic complications are risk factors for cardiac abnormalities.27 28 Thus failing to control for obesity could have given conflicting results in the relationship between OSA and RV dysfunction. Our study showed that RVSVI, RVEF and RVMPI worsen with OSA severity, and AHI independently correlated with these parameters, even after adjusting for age, gender and BMI z score. Cor pulmonale was consistently observed in a previous study in children with severe OSA.7 29 On the other hand, none of the children in our study had cor pulmonale. Nonetheless, our study provides evidence for the first time that subclinical RV dysfunction already exists in children with mild degrees of OSA. Further evidence to support RV involvement in childhood OSA is that RVMPI significantly improved after interventions, as shown in our study as well as in that reported by Tal and colleagues.4 Moreover, the change in RVMPI from baseline to follow-up was significantly associated with the change in AHI (fig 2).
After controlling for age, gender and BMI z score, children with moderate to severe OSA had a 4.2-fold increased risk of abnormal LV geometry compared with the reference group. This finding has important clinical implications as previous studies have found that in individuals with similar LV mass, altered LV geometry was associated with greater cardiovascular risk.31 32 Altered LV diastolic filling is expected from concentric hypertrophy but there was no difference in mitral valve E/A between the groups. The result may be accounted for by the sensitivity of early transmitral velocity (E) to loading condition, heart rate, as well as increase in LV mass. Transmitral flow in relation to tissue diastolic velocity Ea may be a better method of assessing diastolic function,27 28 and E/e′ was indeed shown to increase with OSA severity. This is in agreement with another study on LV function in children with OSA where the authors also demonstrated a dose dependent decrease in diastolic function with increased OSA severity.6 Adenotonsillectomy in children with OSA has been shown to improve growth, neurocognitive function and nocturnal enuresis.33 Well conducted studies that reported on the outcome of OSA treatment on cardiac findings are scarce. Görür et al showed improvement in RV dimension, LV end diastolic diameter and IVS assessed by ECHO after adenotonsillectomy.34 Unique to our study is the presence of a persistent OSA group that consisted of subjects who refused any treatment or did not have significant improvement after treatment. All children who underwent adenotonsillectomy had a ⩾50% reduction in AHI, suggesting that adenotonsillectomy is indeed an effective treatment for childhood OSA (fig 1). On the other hand, only four out of nine children who received nasal steroid therapy had a ⩾50% reduction in AHI. Significant improvements in RVMPI, IVSI, and E/e′ comparing 6 month with baseline data were seen only in the improved OSA group, and indeed the change in RVMPI and E/e′ was associated with a change in AHI. In the mild OSA group, five out of 18 untreated children had significant improvement in AHI, suggesting that some mild OSA cases may spontaneously improve with time. There may be a practical need for follow-up PSG for assessment of treatment efficacy and to monitor progress for those who do not receive treatment.
The severity of OSA in our sample population was milder than in other studies as they were recruited from the community. The results generated from our study are however, important as abnormal cardiac function and structure were already demonstrated in this community based cohort, emphasising the need to recognise OSA early in its progression. A proportion of OSA children did not return for repeat assessment at 6 months, which is one of our limitations and a common difficulty faced by paediatric researchers.35 On further analysis, there were no significant differences in anthropometric, PSG and ECHO measurements between those who did not return and untreated subjects. Cases with persistent OSA at follow-up had less severe disease at baseline than the improved OSA group which may be a potential bias. As treatment was not randomised, naturally parents of children with more severe OSA were more likely to opt for treatment and especially surgery. Although with milder disease at baseline, the ECHO parameters of the persistent OSA group did not improve with time. In contrast, significant improvements were seen following treatment in the improved OSA group, signifying genuine beneficial effects of intervention. The clinical significance of cardiac structural and functional changes described in this study, despite being shown in adult studies8 9 30–32 to predict future clinical events, is not certain in children, and will require longer follow-up to better delineate their implications.
CONCLUSIONS
Childhood OSA is associated with RV and LV remodelling and dysfunction. Community based screening programmes may allow early detection and treatment of OSA that could potentially reverse myocardial dysfunction, remodelling and lessen the risk for future cardiovascular disease.
Acknowledgments
We are grateful for the support of all the staff of the Sleep Assessment Unit of Shatin Hospital, and the cooperation and participation of all the schools, children and their parents.
REFERENCES
Footnotes
J Y S Chan and A M Li are joint first authors.
Funding: This study was supported by a grant (CUHK4161/02M) from the Research Grants Council of the Hong Kong Special Administrative Region, China.
Competing interests: None.
Ethics approval: The study was approved by the institutional ethics committee.
Linked Articles
- Airwaves