Article Text

Abstract
Background: Patients with symptoms of GOLD stage I chronic obstructive pulmonary disease (COPD) can have significant abnormalities of ventilatory mechanics with greater exertional symptoms and exercise limitation than age-matched healthy subjects. In such patients the impact of bronchodilator therapy remains unknown and is difficult to evaluate.
Methods: The acute effects of nebulised ipratropium bromide 500 μg (IB) on resting pulmonary function and on dyspnoea and ventilatory parameters during symptom-limited constant work rate cycle exercise were measured. In a randomised double-blind crossover study, 16 patients with COPD (mean (SD) post-bronchodilator forced expiratory volume in 1 s (FEV1) 90 (7)% predicted, FEV1/forced vital capacity (FVC) 59 (7)%) with a significant smoking history (mean (SD) 44 (16) pack-years) inhaled either IB or placebo on each of two separate visits. Pulmonary function tests and cycle exercise at 80–85% of each subject’s maximal work capacity were performed 2 h after dosing.
Results: Compared with placebo, FEV1 increased 5 (9)% predicted, residual volume decreased 12 (20)% predicted and specific airway resistance decreased 81 (93)% predicted (all p<0.05) after IB. At a standardised time during exercise, dynamic inspiratory capacity and tidal volume significantly increased in tandem by 0.12 and 0.16 litres, respectively (each p<0.05), dyspnoea fell by 0.9 (1.8) Borg units (p = 0.07) and dyspnoea/ventilation ratios fell significantly (p<0.05). The fall in dyspnoea intensity at higher submaximal ventilations correlated with the concurrent decrease in end-expiratory lung volume (p<0.05).
Conclusion: In patients with symptoms of GOLD stage I COPD, IB treatment is associated with modest but consistent improvements in airway function, operating lung volumes and dyspnoea intensity during exercise. These results provide a physiological rationale for a trial of bronchodilator therapy in selected patients with milder but symptomatic COPD.
Statistics from Altmetric.com
Patients with chronic obstructive pulmonary disease (COPD) who have relatively preserved measurements of forced expiratory flow rates may have extensive small airway dysfunction.1–4 Such patients report greater intensity of exertional dyspnoea than healthy age-matched controls as a result of the combined effects of abnormal dynamic ventilatory mechanics and higher ventilatory requirements during exercise.5 This physiological impairment of the respiratory system may explain, at least in part, reports of poor perceived health status in subpopulations of patients with apparently mild airway obstruction.6 Successful smoking cessation is the only proven intervention that has been shown to improve small airway function in patients with mild COPD.2 4 However, the optimal clinical management of these smokers with symptoms of mild COPD is not established and remains largely unstudied. It is not known, for example, whether inhaled bronchodilator therapy, which has established efficacy in moderate to severe COPD,7–10 is effective in alleviating activity-related dyspnoea in those with milder disease. Moreover, it remains uncertain whether traditional spirometric criteria for bronchodilator reversibility, based on arbitrary improvement in the forced expiratory volume in 1 s (FEV1), are applicable in mild COPD. This information becomes important for clinical practice and for the design of future clinical trials to evaluate the efficacy of therapeutic interventions in early COPD.
The purpose of the present study was therefore to evaluate the acute effects of an anticholinergic bronchodilator on airway function and exertional dyspnoea in patients with mild COPD, as defined by GOLD stage I criteria.10 Based on the results of a previous mechanistic study in patients with symptoms of mild COPD,5 we hypothesised that inhaled bronchodilator therapy would improve airway function and lung volumes at rest and reduce the rate of dynamic pulmonary hyperinflation during exercise, thus permitting greater tidal volume expansion and reduced dyspnoea intensity at higher submaximal ventilations. To test this hypothesis we undertook a randomised placebo controlled study in 16 well characterised patients with mild COPD symptoms. We compared the acute effects of nebulised ipratropium bromide and placebo on detailed resting pulmonary function measurements as well as dyspnoea ratings, operating lung volumes, breathing pattern and gas exchange during constant work cycle exercise. To explore potential mechanisms of dyspnoea relief, we also measured oesophageal pressure (Pes)-derived indices of dynamic ventilatory mechanics in a small subsample of patients who consented to undertake these more invasive measurements.
METHODS
Subjects
Sixteen patients with symptoms of GOLD stage I COPD (post-bronchodilator FEV1 ⩾80% predicted and FEV1/forced vital capacity (FVC) ratio <0.7)10 who were referred to the COPD Centre at our institution were studied. Patients were excluded if they had (1) other medical conditions which could cause or contribute to breathlessness (ie, metabolic, cardiovascular, asthma or other respiratory diseases) or (2) other disorders which could interfere with exercise testing such as neuromuscular diseases or musculoskeletal problems.
Study design
This randomised, double-blind, placebo controlled, crossover study was approved by the Queen’s University and Affiliated Hospitals research ethics board. After informed consent and screening of medical history, patients completed four visits conducted approximately 7 days apart. At visit 1, subjects completed pulmonary function tests and a symptom-limited incremental cycle exercise test followed, after 60 min of rest, by a familiarisation constant-load cycle endurance test at 80–85% of their maximal achieved work rate (Wmax). At visit 2 the constant-load cycle test was repeated and, after 60 min of recovery, subjects performed pulmonary function tests before and 20 min after administration of salbutamol (400 μg). At visits 3 and 4, subjects were randomised (sequence) to receive either nebulised ipratropium bromide 500 μg (IB) or a placebo (PL). Subjects performed pulmonary function tests before and 60 min after nebulisation, followed by a constant-load exercise test. All series of pulmonary function tests included spirometry, body plethysmography, transfer factor and respiratory muscle strength measurements. All symptom-limited constant-load exercise tests were conducted at the same work rate for each subject. Withdrawal of bronchodilators before each visit included short-acting β2 agonists (8 h), short-acting anticholinergics (8 h), long-acting β2 agonists (48 h) and long-acting anticholinergics (72 h). Subjects avoided caffeine, alcohol and heavy meals for 4 h before visits and avoided major physical exertion entirely on visit days.
Interventions
A 3.5 ml solution containing either 500 μg IB or sterile 0.9% saline (PL) was administered by nebuliser (Parimaster Compressor with Pari LC Jet+nebuliser; PARI Respiratory Equipment, Richmond, Virginia, USA) over a 15–20 min period in a double-blind fashion.
Procedures
Routine spirometry, body plethysmography (ie, functional residual capacity (FRC) and specific airway resistance (sRaw)), transfer factor for carbon monoxide (Tlco) and maximum inspiratory and expiratory mouth pressures (MIP and MEP; measured at FRC and total lung capacity (TLC), respectively) were performed using an automated system (6200 Autobox DL or Vmax229d; SensorMedics, Yorba Linda, California, USA) in accordance with recommended techniques.11–16 Measurements were expressed as percentages of predicted normal values;17–19 predicted normal inspiratory capacity (IC) was calculated as predicted TLC minus predicted FRC.
Symptom-limited exercise tests were conducted on an electronically braked cycle ergometer as previously described.5 20 21 The incremental test consisted of 2 min increments of 20 W to the point of symptom limitation; Wmax was defined as the greatest work rate that the subject could maintain for at least 30 s. Constant-load tests at 80–85% Wmax were performed during all four visits; endurance time was defined as the duration of loaded pedalling. At end-exercise, subjects were asked why they needed to stop exercising. Rest was the steady-state period after at least 3 min of breathing on the mouthpiece before exercise began; peak was the last 30 s of loaded pedalling; and isotime was the duration of the shortest post-treatment test rounded down to the nearest full minute (ie, highest equivalent isotime).
Cardiopulmonary and breathing pattern measurements were collected in a breath-by-breath fashion while subjects breathed through a mouthpiece with nasal passages occluded by a noseclip using a cardiopulmonary exercise testing system (SensorMedics Vmax229d). Pulse oximetry, electrocardiography and blood pressure measurements were also performed. Subjects rated the intensity of their “breathing discomfort” and “leg discomfort” at rest, every minute during exercise and at end-exercise using the modified 10-point Borg scale.22 Operating lung volumes were derived from IC measurements performed at rest, every second minute during exercise and end-exercise, as previously described.5 Maximal flow-volume loops were obtained at rest and at end-exercise. Tidal flow-volume curves at rest, every 2 min during exercise and at peak exercise were placed within their respective maximal flow-volume loops using coinciding IC measurements; expiratory flow limitation was estimated as the percentage of tidal volume (Vt) encroaching on the maximal flow envelope.23 In six subjects, oesophageal pressure (Pes) was recorded continuously during constant-load exercise tests using an integrated data acquisition set-up as described elsewhere (see online supplement).20 Inspiratory sniff manoeuvres were performed before exercise at rest and immediately at end-exercise to obtain maximum values for Pes (PImax).
Statistical analysis
A sample size of 16 was used to provide the power (80%) to detect a significant difference in dyspnoea intensity (Borg scale) measured at a standardised work rate during incremental cycle exercise based on a relevant difference in Borg ratings of ±1, an SD of 1 for changes in Borg ratings found in our laboratory (α = 0.05). Results were expressed as mean (SD). A p<0.05 level of statistical significance was used for all analyses.
Although unlikely in this single-dose study, the possibility of a carryover effect was tested using paired t tests to evaluate pre-dose (pre-treatment) pulmonary function measurements. Period effects were evaluated using the two-sample t test.24 Treatment comparisons were made using paired t tests with appropriate Bonferroni adjustments for multiple comparisons. Responses at rest and at different time points and/or intensities during exercise were also compared. Repeated measures ANOVA (with treatment, time and interaction as fixed effects and subject as a random effect) was applied to compare the overall treatment effects. Dyspnoea descriptors were analysed as frequency statistics and compared using the Fisher exact test. Physiological contributors to exertional dyspnoea intensity were determined by multiple regression analysis: Borg dyspnoea ratings at a standardised exercise work rate (dependent variable) were analysed against concurrent relevant independent variables (ie, exercise measurements of ventilation, breathing pattern, operating lung volumes, cardiovascular and metabolic parameters, and baseline pulmonary function measurements).
RESULTS
Subjects
Subject characteristics are summarised in table 1. All subjects were had symptoms and had a diagnosis of COPD; the majority (11/16) had a diagnosis made within the previous 5 years. Seven subjects did not use any respiratory medications, two only used a short-acting β2 agonist bronchodilator on an “as needed” basis and seven used inhalers on a regular basis. Of these latter seven subjects, all used short-acting β2 agonists, five used a long-acting β2 agonist, five used an anticholinergic (one short-acting, four long-acting) and six used an inhaled corticosteroid (five in combination with a long-acting β2 agonist). Comorbidities included stable coronary artery disease (n = 2), well-controlled diabetes mellitus type 2 (n = 1), treated hypertension (n = 1) and varying degrees of osteoarthritis (n = 4). All subjects had a smoking history of ⩾15 pack-years (range 15–63 pack-years, table 1); four subjects were current smokers and 12 were ex-smokers who had stopped smoking at least 2 years before the study.
Chronic activity-related dyspnoea was assessed with the baseline dyspnoea index (BDI)25 and the Medical Research Council (MRC) dyspnoea scale.26 BDI focal scores ranged from 5 to 12; nine subjects reported a BDI ⩽8 and seven subjects reported a BDI ⩾9. The majority of subjects (11/16) had a rating of ⩾2 on the MRC dyspnoea scale.
All subjects had a normal post-bronchodilator FEV1 and an FEV1/FVC ratio <70%. Lung volumes indicated mild static lung hyperinflation (mean FRC and RV >120% predicted) with a preserved vital capacity and inspiratory capacity (IC) (table 1). Symptom-limited incremental exercise testing showed reduced peak oxygen consumption (V̇o2) and work rate. The subgroup of subjects with Pes-derived measurements had comparable baseline characteristics to the group as a whole (table 1). There were also no significant differences in the baseline characteristics or in the magnitude of the treatment responses between patients who were using respiratory medication and those who were not.
There were no significant differences between predose measurements of pulmonary function on treatment days (ie, no significant carryover effect). No significant period effects were found when examining pulmonary function or exercise test outcomes.
Pulmonary function responses
Differences in pulmonary function after IB compared with PL are shown in table 2. Subjects with the worst baseline prebronchodilator specific airway resistance (sRaw) had the greatest IB-induced improvements in sRaw (r = −0.595, p = 0.015) and IC (r = 0.594, p = 0.015); improvements in sRaw and IC were also strongly interrelated (r = −0.680, p = 0.004). Maximal expiratory flows measured at FRC after PL were compared with the maximal flow at the same absolute volume after IB within each individual: these isovolume flows improved from a mean (SD) of 0.27 (0.18) l/s to 0.43 (0.30) l/s after PL and IB, respectively (p = 0.006).
Responses to constant-load exercise
Post-dose exercise endurance time at 99 (32) W (60 (11)% predicted maximum; 82 (9)% Wmax) did not change significantly after IB compared with PL (table 3): six subjects improved endurance time by ⩾30 s, three subjects decreased endurance time by ⩾30 s and the rest had less than a 30 s difference in endurance time. The distribution of reasons for stopping exercise was not different between treatments. In both visits, leg discomfort was reported as the primary reason for stopping exercise, 2–3-fold more than breathing discomfort (table 3).
Exertional symptoms
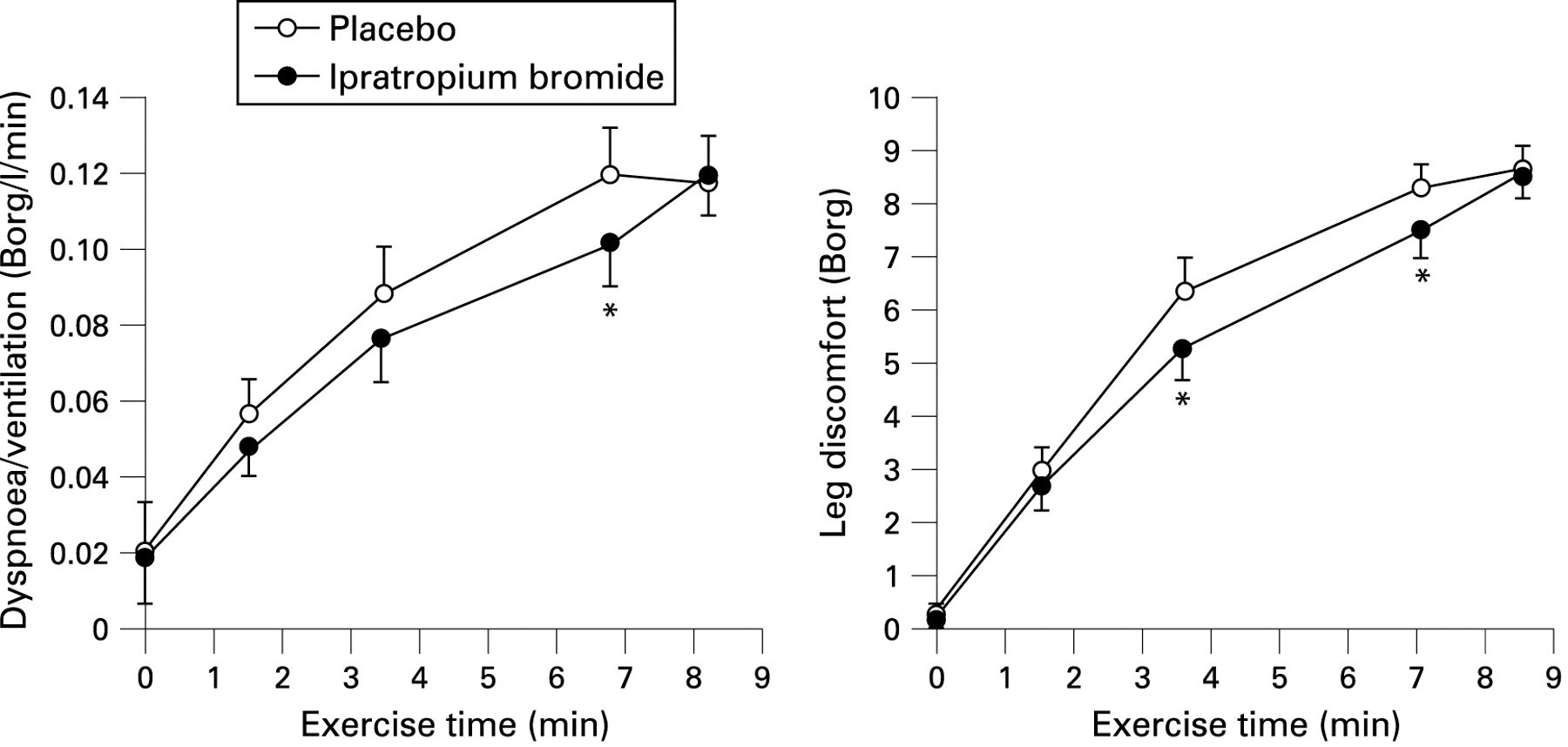
Compared with PL, there was no change in peak Borg ratings of breathing or leg discomfort after IB (table 3). However, ratings of breathing and leg discomfort at the highest equivalent isotime (6.8 (4.5) min) during exercise were lower after IB compared with PL by 0.88 (1.83) Borg units (p = 0.073) and 0.81 (1.28) Borg units (p<0.05), respectively (table 4, fig 1). Ten of the 16 patients decreased the intensity of their breathing discomfort at isotime by at least 1 Borg unit, while the remaining subjects increased (n = 4) or did not change (n = 2) ratings of breathing discomfort after IB compared with PL. Dyspnoea/V̇e ratios were evaluated to account for the potential effects of IB-induced alterations in V̇e on exertional dyspnoea intensity: dyspnoea/V̇e ratios were significantly lower (p<0.05) at isotime after IB than after PL (table 4, fig 1). By repeated measures ANOVA, there were no significant interactions between treatment and time during exercise for exertional symptom ratings (ie, the treatment effect did not vary at different times); however, a significant treatment effect was found for dyspnoea/V̇e ratios (p = 0.075) and leg discomfort ratings (p = 0.021).

Ventilatory responses
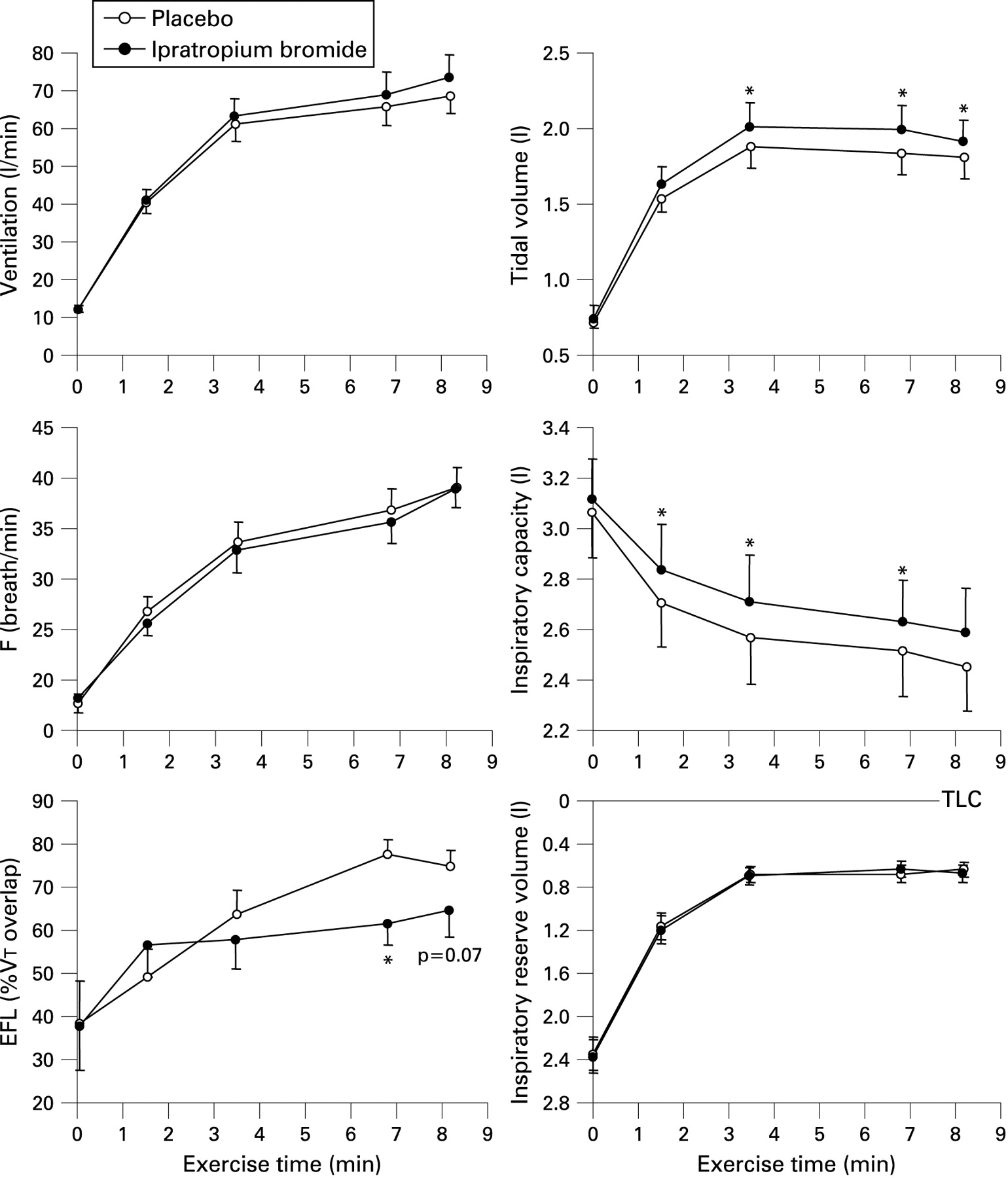
Ventilatory responses to exercise after IB and PL are shown in fig 2. Tidal volume (Vt) was greater after IB compared with PL from minute 4 in exercise to peak exercise by 0.10–0.16 l (p<0.05); increases in Vt were accommodated by concurrent increases in IC of 0.12–0.15 l (p<0.05). Inspiratory reserve volume (IRV) was not different at rest or throughout exercise across treatments. Estimates of expiratory flow limitation were reduced at isotime and at peak exercise by 10% and 17% (p<0.05), respectively, after IB compared with PL. Repeated measures ANOVA also showed a significant treatment effect for Vt (p = 0.012), IC (p = 0.001) and expiratory flow limitation (p = 0.014), with no significant interactions between treatment and exercise time.

Ventilatory mechanics
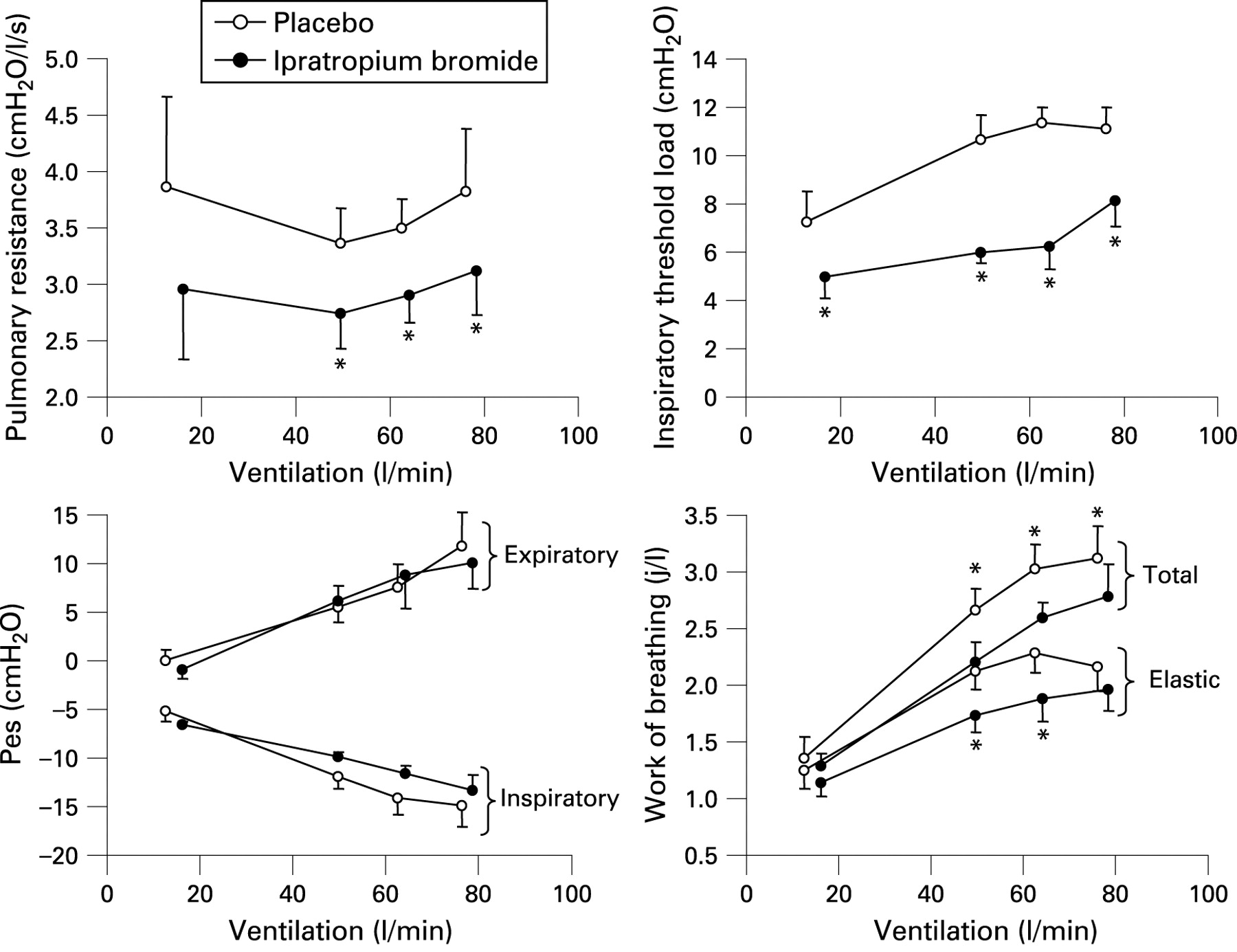
The pressure-time integral and its surrogate, the calculated tension-time index (Pes/PImax×Ti/Ttot), were not different in response to treatment. However, lung resistance was reduced after IB compared with PL in the order of 0.7–0.8 cm H2O/l/s at standardised time points throughout exercise (ie, a reduction of ∼20% (p<0.05), fig 3). Total work of breathing expressed as J/l fell significantly (p<0.05) during exercise but not at rest after IB compared with PL, primarily due to significant (p<0.05) decreases in the inspiratory threshold load and the elastic work performed against this load. Repeated measures ANOVA showed a significant treatment effect for resistance (p = 0.007), the inspiratory threshold load (p<0.001), total work of breathing (p = 0.002) and elastic work of breathing (p = 0.001), with no significant interactions between treatment and exercise time. Work of breathing measurements were not different when expressed as J/min, so differences were offset by increases in V̇e.

{kind=link}
{kind=link}
{kind=link}
Correlates of dyspnoea
The best predictors of the IB-induced decrease in dyspnoea ratings at isotime were the baseline (prebronchodilator) pre-exercise resting IC expressed as percentage predicted (r = 0.637, p = 0.008), the end-inspiratory lung volume (EILV)/TLC ratio (r = −0.561, p = 0.024) and the IRV expressed as percentage predicted TLC (r = 541, p = 0.030); no other baseline pulmonary function parameters correlated. The best correlates of the IB-induced decrease in dyspnoea/V̇e ratios at isotime were also the prebronchodilator pre-exercise resting IC expressed as percentage predicted (r = 0.714, p = 0.002), the EILV/TLC ratio (r = −0.637, p = 0.008) and the IRV expressed as percentage predicted TLC (r = 0.549, p = 0.028). When dyspnoea was expressed as a ratio against V̇e (Borg/(l/min)), the strongest correlate of this treatment difference at isotime was the concurrent difference in EELV/TLC (r = 0.585, p<0.05).
DISCUSSION
The novel findings of this study are as follows: (1) treatment with IB was associated with consistent improvements in forced expiratory flow rates, sRaw and RV in patients with GOLD stage I COPD symptoms; (2) during exercise, IB treatment was associated with significant increases in dynamic IC and Vt in the absence of an increase in cycle exercise endurance time; and (3) improvement in dynamic EELV was linked to a reduction in ratings of exertional dyspnoea intensity at higher levels of ventilation.
Changes in resting pulmonary function
Our patients had extensive physiological impairment and long-term activity-related dyspnoea as measured by validated questionnaires. More than half of the group was already receiving empirical bronchodilator therapy. Our results confirm that release of cholinergic smooth muscle tone improved airway function both at rest and during exercise in these patients. In general, changes in resting spirometry and lung volumes were in the same direction but more modest than those previously reported following a similar dose of IB in moderate to severe COPD.7–9 Airway resistance, corrected for the lower resting operating volume, decreased after IB by 33% of baseline values while isovolume maximal flow rates in the effort-independent range also consistently improved.
In contrast to previous studies of the acute effects of IB in more advanced disease, resting IC did not increase significantly in our cohort with milder COPD. Thus, FRC and TLC fell in tandem and to a similar extent, such that the change in IC underestimated the extent of IB-induced lung deflation. Small but consistent bronchodilator-associated decreases in TLC have previously been reported in COPD, but the precise mechanisms are unknown.27 28 Decreases in the plethysmographically-determined TLC may reflect measurement artefact, since mouth pressure during panting could potentially underestimate true alveolar pressure in patients with airflow limitation. A reduction in this disparity after a bronchodilator may result in an artifactual reduction in TLC. We tried to minimise this effect by controlling panting frequency at ∼1 Hz. It is unlikely that changes in (regional) lung compliance can explain the observed reductions in TLC; lung compliance curves were superimposed before and after IB in our small subsample with mechanical measurements.
The lack of increase in resting IC in our patients is not surprising. Based on the study of Tantucci et al,29 bronchodilator-induced increases in IC are only expected in patients with COPD who have more extensive expiratory flow limitation and lung hyperinflation (ie, IC <80% predicted) at rest.
Altered ventilatory responses to exercise after bronchodilator
Exercise endurance time did not increase after bronchodilator compared with placebo. Possible explanations for this are: (1) the study was powered to detect an improvement in dyspnoea at a standardised work rate and not a change in exercise endurance time; and (2) intolerable leg discomfort and not dyspnoea was the dominant exercise-limiting symptom in the majority of this group.
IC diminished by 0.55 l from rest to peak exercise, confirming the presence of air trapping due to expiratory flow limitation and high ventilatory demand in patients with mild COPD. Compared with placebo, IB treatment was associated with a significant increase in IC by 0.12–0.15 l throughout exercise, despite slightly greater levels of ventilation (∼3 l/min). However, the magnitude of acute change in IC from pre-exercise resting levels at each time point and at peak exercise remained similar (fig 2). We also found consistent reductions in our estimate of expiratory flow limitation at higher exercise levels after IB. Moreover, pulmonary resistance and conductance were significantly improved during exercise in the subsample who consented to oesophageal balloon measurements. The most likely explanation for lung deflation is therefore improvement in the time constant for lung emptying as a result of reduced airway resistance rather than minimal changes in expiratory time (prolongation) and static lung recoil pressure. The improved dynamic IC allowed greater Vt expansion throughout exercise without further encroachment on the dynamic IRV.
Mechanisms of dyspnoea relief
Standardised ratings of exertional dyspnoea intensity as measured by the Borg scale were not statistically different (p = 0.07) after IB compared with placebo, probably due to small concomitant increases in V̇e with IB. However, when IB-induced alterations in V̇e were taken into account by examining dyspnoea/V̇e ratios, these changes reached statistical significance (p<0.05). Compared with placebo, the decrease in the dyspnoea/V̇e ratio after IB correlated best with the concurrent decrease in the dynamic EELV/TLC ratio. In a small subset of patients the measured work of breathing and the pressure-time product (reflecting the oxygen cost of breathing) was not increased after IB despite significantly greater Vt expansion. The work associated with overcoming the inspiratory threshold load (the intrinsic PEEP effect) was significantly reduced at standardised times during exercise. We have argued that increased threshold loading of the inspiratory muscles as a result of dynamic pulmonary hyperinflation plays an important role in dyspnoea causation in asthma during bronchoconstriction and in more advanced COPD during exercise.30–32 Reduction of the inspiratory threshold load by lung deflation should relieve dyspnoea by reducing the disparity between efferent motor output (sensed by increased corollary discharge) and afferent inputs from mechanosensors in the respiratory muscles, chest wall and lungs (ie, neuromechanical coupling).33 Thus, dyspnoea relief was related to improved inspiratory muscle function as a result of a reduced dynamic EELV as well as the recruitment of an increased dynamic IC which allowed greater Vt displacement for the same inspiratory effort.
It is noteworthy that patients who derived the greatest reduction in exertional dyspnoea with IB treatment were those with the most severe lung hyperinflation at baseline. In fact, of all the resting physiological parameters that we measured, only the resting prebronchodilator IC and IRV (percentage predicted) correlated with improved dyspnoea intensity ratings during exercise. Previous studies have shown that, when the normal spontaneous Vt response to increasing central respiratory drive is constrained (either volitionally or by imposition), dyspnoea quickly escalates to intolerable levels.34 35 It follows that release of Vt restriction (ie, IC recruitment) should improve dyspnoea.21 36
In summary, traditional spirometric measurements reliably detected modest but consistent improvements in airway function after bronchodilator treatment in patients with symptoms of mild COPD. Bronchodilator administration was associated with improved dynamic IC and a deeper breathing pattern throughout exercise. Dyspnoea intensity ratings fell only at the higher levels of ventilation with IB treatment, in association with reduced dynamic EELV. Mechanical and subjective improvements during exercise after IB treatment were most pronounced in those with the smallest resting IC (and IRV) and therefore the greatest mechanical constraints on tidal volume expansion.
This study highlights the challenges involved in the assessment of bronchodilator efficacy in milder COPD where no evidence-based guidelines for pharmacotherapy currently exist. Our results provide a sound physiological rationale for consideration of a trial of bronchodilator therapy in selected patients with GOLD stage I COPD who experience troublesome activity-related dyspnoea.
REFERENCES
Supplementary materials
web only appendix 64/3/216
Files in this Data Supplement:
Footnotes
Additional Methods data are published online only at http://thorax.bmj.com/content/vol64/issue3
Presented in part at the ALA/ATS International Conference, Toronto, May 2008 (Ofir D, Laveneziana P, Webb KA, et al. Evaluation of bronchodilator efficacy in symptomatic patients with GOLD stage I COPD. Am J Respir Crit Care Med 2008;177(Suppl):A649).
Funding: Supported by William M Spear endowment fund, Queen’s University.
Competing interests: None.
Ethics approval: This study was approved by the Queen’s University and Affiliated Hospitals research ethics board.
Linked Articles
- Airwaves