Article Text

Statistics from Altmetric.com
Respiratory acidosis and alkalosis are associated with compensatory physiological changes, including extracellular and intracellular buffering, and altered renal ion handling. In clinical practice, mixed acid-base disturbances may be misdiagnosed if the expected magnitude of compensation for a primary respiratory disorder is not known.
The ability to assess physiological compensation rapidly for acid-base disorders can be achieved either through intuition gained after many years of clinical experience, by use of a graph or nomogram,1 or through the application of one of the published formulae for predicting compensation.2 3 However, nomograms are often not readily available in clinical environments, and the most accurate formulae are complex and difficult to memorise reliably.
A comprehensive summary of previously published measurements of metabolic compensation for respiratory disorders was recently published.3 Using these data, simple but accurate “rules of thumb” for the assessment of physiological compensation for respiratory disorders are developed here.
Methods
In SI units, carbon dioxide tension (Pco2) and bicarbonate (HCO3−) are linked by the equation [H+] = 182.36 Pco2/[HCO3−]. For clinical purposes, this can be simplified to [H+] = 180 Pco2/[HCO3−]. Manually extracted graphical data from the study by Schilchtig et al3 are used here to generate new rules which more accurately estimate metabolic compensation for respiratory disorders. For the purpose of calculations, normal HCO3− concentration was taken as 24.4 mM and normal Paco2 is taken as 5.3 kPa.
Results
Of several methods tried, the most easily memorised approach was to calculate the number of mM change in HCO3− (ΔHCO3−) for a 1 kPa change in Pco2. This method enables the quick estimation of the appropriate HCO3− from a given value of Pco2 for metabolic compensation for respiratory disorders.
The following rules are proposed:
Acute respiratory acidosis: ΔHCO3− = 1 mM for each 1 kPa change in Pco2
Acute respiratory alkalosis: ΔHCO3− = 2 mM for each 1 kPa change in Pco2
Chronic respiratory acidosis: ΔHCO3− = 4 mM for each 1 kPa change in Pco2
Chronic respiratory alkalosis: ΔHCO3− = 3 mM for each 1 kPa change in Pco2
The spread of clinical data (fig 1) shows that these rules predict compensation accurately within the approximate range ±5 mM.

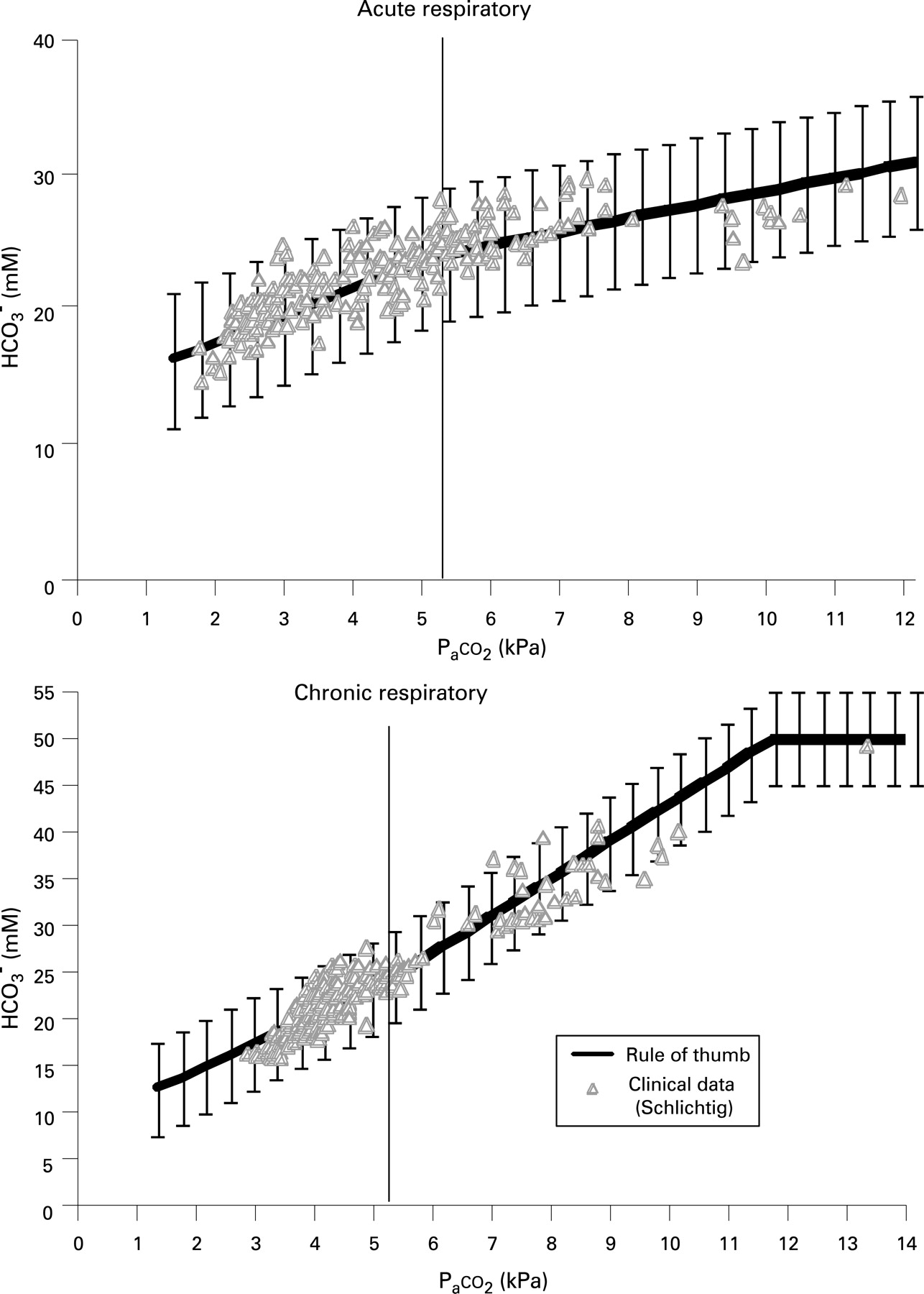{kind=link}
Discussion
The proposed rules fit the published data more closely than those proposed previously (fig 1).2 There appears to be a maximum metabolic compensation for chronic respiratory acidosis and neither the rules of thumb presented here nor the published formulae accommodate this. Even in extreme circumstances, the maximum range for metabolic compensation appears to lie between 12 mM4 and 50 mM.5 Incorporating this additional information, the rule for chronic respiratory acidosis adopts a better fit with the published data (fig 1).
The data plotted in fig 1 also give evidence for the widely accepted tenet that overcompensation for primary acid-base disorders does not occur. This means that any change in [H+] opposite to that produced by the primary disorder must be pathological. In these conditions it is therefore not necessary to use the methods described here.
Finally, acute compensation for respiratory disorders is usually small. Thus, for normal clinical practice, only two rules must be learnt: chronic respiratory alkalosis (3 mM for each kPa of CO2), and chronic respiratory acidosis (4 mM for each kPa).
Acknowledgements
The author would like to thank Dr C Richard and Dr AAR Thompson for their comments and suggestions on the manuscript.