Article Text

Abstract
Background: Airway obstruction in acute asthma is the result of airway smooth muscle contraction, inflammation and mucus plugging. Case reports suggest that mucolytic therapy might be beneficial in acute asthma. The aim of this study was to determine the efficacy of the mucolytic drug recombinant human deoxyribonuclease (rhDNase) in addition to standard treatment at the emergency department in children with an asthma exacerbation.
Methods: In a multicentre randomised double-blind controlled clinical trial, 121 children brought to the emergency room for a moderate to severe asthma exacerbation were randomly assigned to receive either a single dose of 5 mg nebulised rhDNase or placebo following the second dose of bronchodilators. An asthma score (scale 5–15) was assessed at baseline and at 1, 2, 6, 12 and 24 h. The primary outcome variable was the asthma score 1 h after the study medication.
Results: One hour after the study medication the asthma score in the rhDNase group showed an adjusted mean decrease from baseline of 1.0 (95% CI 0.5 to 1.6) points compared with 0.7 (95% CI 0.3 to 1.2) points in the placebo group (mean difference 0.4 (95% CI −0.2 to 1.0) points; p = 0.23). The asthma score over the study period of 24 h also did not differ significantly between the rhDNase and placebo group (mean difference 0.2 (95% CI −0.3 to 0.7) points, p = 0.40). The duration of oxygen supplementation and number of bronchodilator treatments in the first 24 h were similar in both groups.
Conclusion: Adding a single dose of nebulised rhDNase to standard treatment in the emergency room has no beneficial effects in children with moderate to severe acute asthma.
Statistics from Altmetric.com
The standard treatment for children with acute asthma consists of frequent nebulised bronchodilators and early systemic corticosteroid therapy.1 Since airway obstruction by viscous mucus is one of the pathophysiological features of acute asthma,2–4 a logical approach to treatment might be to use a mucolytic agent. It is the DNA present in mucous plugs following lysis of inflammatory cells that contributes to increased viscosity and adhesiveness of the mucus,5 and free DNA was indeed noted in the mucus of subjects with acute asthma.6 Such mucus can be liquefied by recombinant human deoxyribonuclease (rhDNase; dornase alfa) which cleaves extracellular DNA.7 8 The efficacy of rhDNase has been well documented in patients with cystic fibrosis,9 and several publications suggest that it is also effective in children with severe acute asthma with10–12 or without atelectasis.11 13
We performed a randomised controlled trial to determine whether nebulised rhDNase added to standard treatment would improve symptoms in children with moderate to severe acute asthma.
METHODS
Patients
Eligible subjects for this study were children aged 2–18 years with symptoms of acute asthma whose asthma score (table 1) at arrival in the emergency room was ⩾8 and who required at least two treatments with nebulised bronchodilators. We did not include children with other causes of dyspnoea, a chronic cardiopulmonary disease other than asthma or those with a neurological condition.
Study design
This was a multicentre double-blind parallel-group randomised study comparing the effect of inhaled rhDNase with placebo on the asthma score in children aged 2–18 years with symptoms of acute asthma. The trial was carried out in emergency rooms of eight participating hospitals in the Netherlands between September 2005 and October 2006. The study was approved by the ethics review boards of all eight centres and written parental informed consent was obtained for each child.
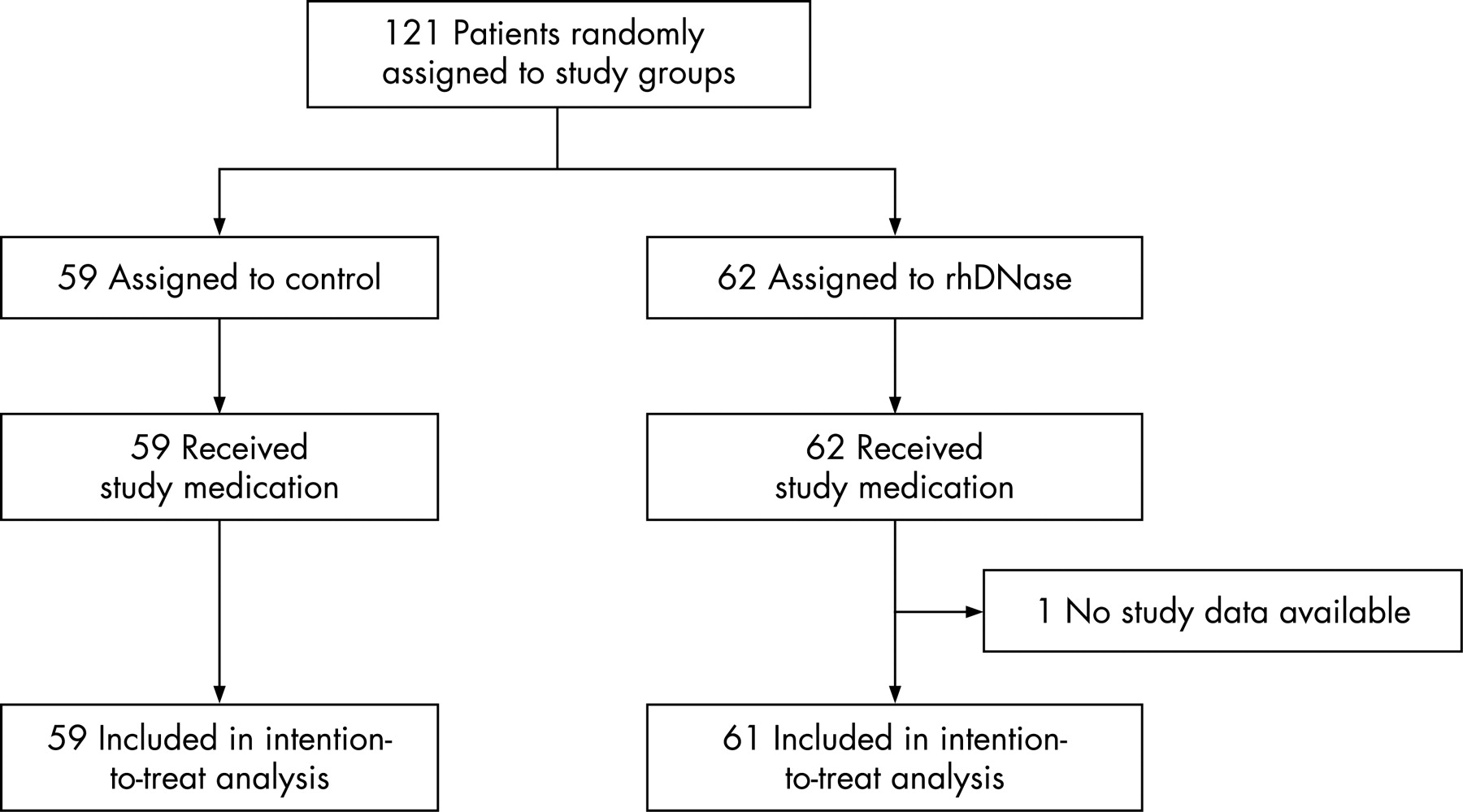
All children received a dose of nebulised bronchodilators on arrival (<4 years old: 2.5 mg salbutamol, 0.25 mg ipratropium; ⩾4 years old: 5 mg salbutamol, 0.5 mg ipratropium). After parental consent, patients were randomly assigned to receive a single nebulisation of 5 mg rhDNase (5 ml solution of 1 mg/ml rhDNase; Roche, Basel, Switzerland) or 5 mg placebo (5 ml sodium chloride 0.9%) following the second nebulisation of bronchodilators (fig 1). We opted for a dose of 5 mg in anticipation of the expected suboptimal lung deposition in young children with airways obstruction due to asthma. Study medication was prepared by the hospital pharmacists and had identical appearance and aroma. The vials with study medication were stored in a refrigerator located in the emergency department.

Study medication was administered with the use of a jet nebuliser using a mouthpiece when possible or through a firmly applied facemask at a constant oxygen supply rate of 6–8 l/min from a wall outlet. The same nebulising equipment (Pari LC Star, Pari GmbH, Germany) was used in all participants.
Randomisation was carried out in the hospital pharmacies of the participating hospitals using a random table sample with blocks of four numbers prepared by the study statistician. Throughout the study, physicians, nurses, parents and the trial coordinator remained unaware of the treatment assignment.
The dosing interval of nebulised bronchodilators was determined by the attending physician based on symptom severity and clinical improvement rate. Systemic corticosteroids (1 mg/kg prednisolone as a starting dose and subsequently 1–2 mg/kg/day for 5–7 days to a maximal dose of 60 mg/day) were given after the second dose of bronchodilators according to Dutch national asthma guidelines.
On the child’s arrival at the emergency department (TA) the attending physician recorded the clinical history (including previous admissions for asthma, duration and possible triggers of the current symptoms) and medication use. Vital signs, the need for supplemental oxygen and the asthma score were also assessed at TA and again just before nebulisation of the second dose of bronchodilators that was followed by the single dose of study medication (T0). The asthma score was subsequently assessed at 1±0.25 h (T1), 2 ±0.5 h (T2), 6±1 h (T6), 12±2 h (T12) and 24±2 h (T24) after nebulisation of the study medication (fig 1). Supplemental oxygen was started when haemoglobin saturation was consistently lower than 93% and was stopped when saturation was consistently above 92%. The total number of nebuliser treatments in the first 24 h after the study medication, time until discharge and duration of oxygen supplementation were recorded.
The decision to admit or discharge the child was up to the discretion of the treating physician. If the child was discharged home from the emergency department or within 24 h after admission, the researcher reported 3–5 days later whether any subsequent visits had been made to a medical facility within 72 h after the initial presentation.
Efficacy end points
The primary outcome measure was the asthma score 1 h after the study medication. We used the asthma score developed by Qureshi and colleagues14 in which respiratory rate, haemoglobin saturation, auscultatory findings, retractions and dyspnoea are scored on a 3-point scale, yielding a total score ranging from 5 (mild) to 15 (severe) (table 1). A previous study showed good inter-rater reliability of this asthma score (Pearson correlation statistic 0.92).14 The asthma score had been introduced as a clinical tool in all participating centres before the start of the study, so all participating physicians were experienced in using the score.
The secondary outcome measures were the mean asthma scores at 2, 6, 12 and 24 h after the study medication, need for hospital admission, duration of admission, duration of supplemental oxygen and the number of nebuliser treatments in the first 24 h.
Estimate of sample size
In a pilot study of 26 children the mean (SD) asthma score decreased 0.8 (1.4) points between the time points T0 (before the second dose of bronchodilators) and T1 (1 h after the second dose of bronchodilators). To demonstrate an additional decrease of 0.8 points at T1 at a 5% significance level for a two-sided test with 80% power would require 100 patients (50 children in each group).
Statistical analysis
Data were analysed on an intention-to-treat basis. Differences between baseline group characteristics and secondary outcome measures were assessed by χ2 or Fisher exact tests and the Mann-Whitney test, as appropriate. Main analyses of between-group comparisons regarding asthma score changes were performed by repeated measures of analysis of variance (RmANOVA) with baseline (T0) asthma score, age, sex and study centre as covariates. In calculating mean values of the asthma score, the individual asthma score after discharge was arbitrarily set at 5 points. Linear interpolation of the asthma score was used if scores had been assessed outside the prespecified time range. Linear interpolation was also used when the item “dyspnoea” could not be assessed accurately because the child was asleep at the time of observation. The analysis was performed with SPSS software Version 11.5 and SAS PROC MIXED. For all the analyses, a two-tailed p values of <0.05 was considered to indicate statistical significance.
RESULTS
A total of 121 children were enrolled and randomly assigned to treatment groups: 62 to rhDNase and 59 to placebo (fig 2). There was no difference in the demographic and baseline clinical characteristics of the two groups (table 2).

All children were treated with a dose of nebulised bronchodilators on arrival in the emergency department. Overall, the asthma score decreased after this first nebuliser treatment by a mean of 1.55 (95% CI 1.32 to 1.79) points (fig 3). The study medication in the rhDNase group was given a median of 1.3 h (interquartile range (IQR) 1.0–2.0) after arrival and in the placebo group after 1.3 h (IQR 1.0–1.8) (p = 0.95).

Primary end point
Both groups showed a similar improvement in the asthma score during the first 24 h (fig 3). At baseline, the mean asthma score was 10.2 in the rhDNase-treated group and 10.4 in the placebo group. One hour after nebulisation of the study medication the asthma score in the rhDNase group showed an adjusted mean decrease of 1.0 (95% CI 0.5 to 1.6) points from baseline compared with 0.7 (95% CI 0.3 to 1.2) points in the placebo group (mean difference 0.4 (95% CI −0.2 to 1.0) points; p = 0.23).
Overall, compared with baseline, the asthma score 1 h after the study medication had improved in 72 children (37 in the rhDNase group, 35 in the placebo group), had not changed in 21 (12 rhDNase, 9 placebo) and had worsened in 27 children (12 rhDNase, 15 placebo); p = 0.68.
Repeated measures analysis of variance showed no significant difference between the groups in the asthma score over the whole period of 24 h: the adjusted mean decrease was 4.1 (95% CI 3.6 to 4.6) points in the rhDNase group and 3.9 (95% CI 3.3 to 4.5) points in the placebo group (mean difference 0.2 (95% CI −0.3 to 0.7) points; p = 0.40).
The item “dyspnoea” of the asthma score could not be assessed accurately in some children who were asleep at the time of the observation. In these cases, linear interpolation of the item “dyspnoea” was used in order to obtain a total asthma score. An analysis in which the interpolated asthma scores of sleeping children were not included showed similar results (data not shown).
Subgroup analyses
There was no significant effect modification by baseline asthma score, age or the use of anti-inflammatory medication prior to the asthma attack. A separate analysis of the subgroup of children with a severe asthma score (⩾12) at baseline (n = 35) also showed no significant difference in the asthma score over time between the rhDNase group and the placebo group (mean difference −0.1 (95% CI −1.3 to 1.1); p = 0.85).
Secondary end points
Need for hospital admission
Most of the children (88%) were admitted to hospital. Only 14 children (6 in the rhDNase group, 8 in the placebo group) were discharged home from the emergency department. Four of the admitted children (4%) required intensive care (2 in the rhDNase group, 2 in the placebo group).
Thirty-one children were discharged within 24 h of study entry (14 in the rhDNase group, 17 in the placebo group). Three of those in the placebo group were readmitted to hospital within 72 h of discharge because symptoms had worsened (1 child after 1 day, 2 children within 1.5 h of discharge) compared with none in the rhDNase group (p = 0.23).
Time until discharge
The time until discharge did not differ between the rhDNase group and the placebo group (geometric mean (SE) 36.9 (1.2) vs 33.9 (1.2) h; mean difference 0.92 (95% CI 0.55 to1.54), p = 0.75).
Duration of oxygen supplementation
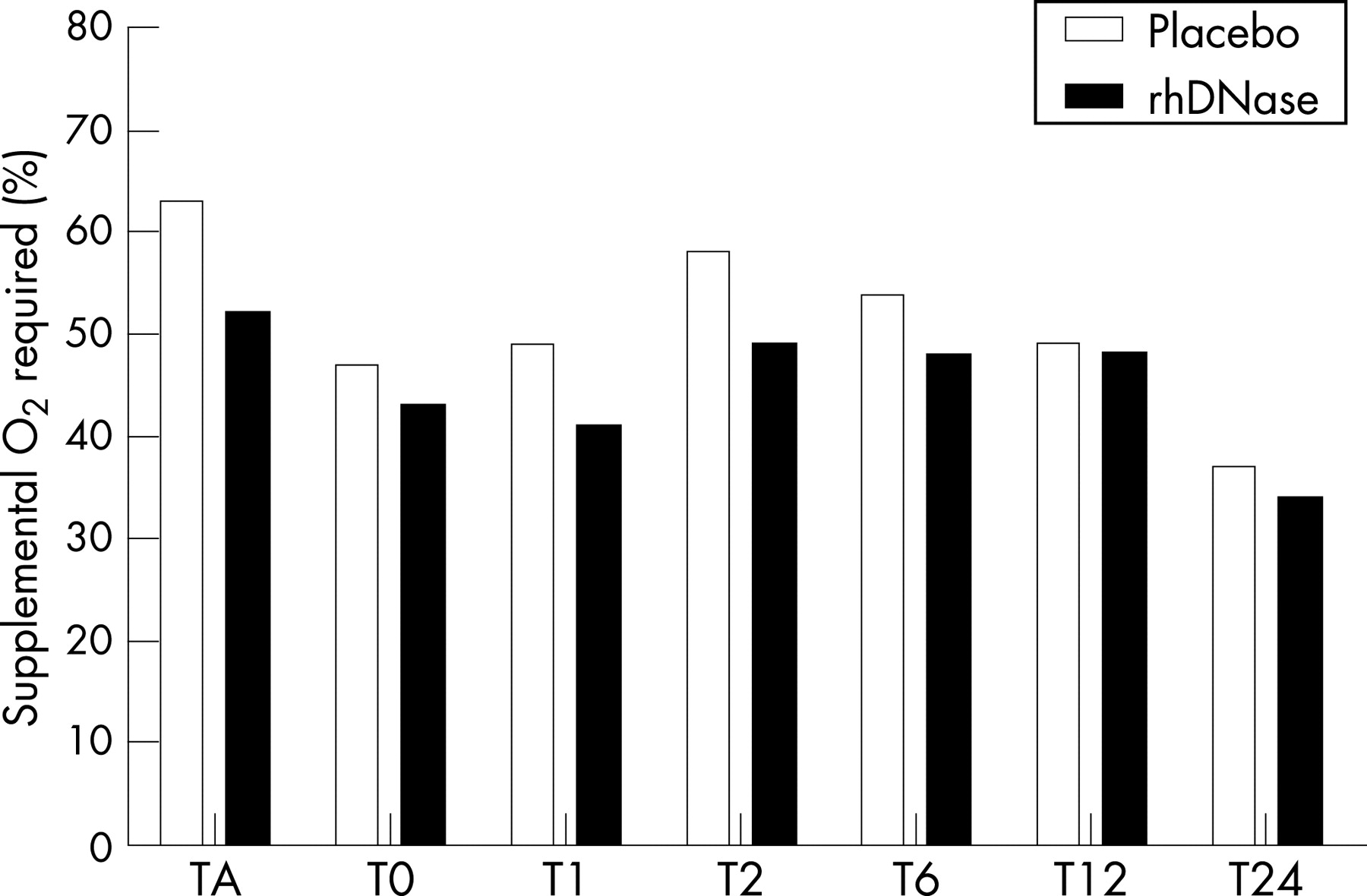
The proportions of children requiring oxygen supplementation to maintain a haemoglobin saturation ⩾93% were similar in both groups over time (fig 4). The geometric mean (SE) time of oxygen supplementation did not differ; for both groups it was 28.3 (1.2) h (p = 0.99).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Co-interventions
Overall, there was no difference between the two groups in the number of treatments with nebulised bronchodilators given in the first 24 h during the hospital stay. Children in the rhDNase group received a median number of 7.0 (IQR 5.5–11.0) nebuliser treatments compared with 8.0 (IQR 6.0–10.0) in the placebo group (p = 0.81). In the subgroup of children who were discharged within 24 h (n = 30), the number of nebuliser treatments did not differ between the rhDNase and placebo group (2.0 (IQR 0.0–5.3) and 2.5 (IQR 0.0–7.0), respectively, p = 0.40).
Prednisolone was administered to 90% of all children (55 of 59 in the placebo group and 53 of 61 in the rhDNase group). Twelve patients did not receive a course of systemic steroids (5 were discharged home from the emergency department after their symptoms had resolved following the dose of study medication).
Safety data
One child had a transient desaturation with an increase in dyspnoea and tachypnoea directly after the initiation of the nebulisation with rhDNase, which resolved quickly after the nebulisation was stopped. Hoarseness was reported in two children (one in each group).
Asthma scores for 27 children were higher (worsened) 1 h after nebulisation of the study medication compared with baseline (12 children in the rhDNase group vs 15 in the placebo group, p = 0.47).
DISCUSSION
We report the first randomised double-blind controlled trial of nebulised rhDNase in children (aged 2–18 years) with an acute asthma exacerbation. The findings show no evidence to suggest that nebulisation with the mucolytic rhDNase alleviates symptoms in children brought to the emergency room for moderate to severe acute asthma. We thus must reject our hypothesis that rhDNase is an effective additional treatment for children with acute asthma. This was based on the important role of mucus plugs in the pathophysiology of acute asthma,2 3 and the finding that the DNA content is increased in the mucus of patients with acute asthma.6
To date, only case reports have suggested a benefit from rhDNase in children with status asthmaticus unresponsive to conventional treatment,10–13 and in children with acute severe asthma treated at the emergency department.11 Intervention with rhDNase, administered endotracheally or by means of a bronchoscope, was safe and improved ventilator settings12 13 and arterial blood gas values13 and resolved atelectasis10 12 in children receiving intensive care. Nebulisation of rhDNase in three children brought to the emergency department improved lung function parameters, the effectiveness of coughing and resolved atelectasis.11
There may be several explanations for the lack of effect of rhDNase in our study. First, the children might have had relatively mild disease with too little mucus plugging for rhDNase to be effective. Indeed, although all selected children had a moderate to severe asthma exacerbation and required at least two doses of bronchodilators, only four children required intensive care treatment. However, a subgroup analysis of children with an asthma score of at least 12 points after their first bronchodilator dose also could not demonstrate an effect of rhDNase. Because this analysis is underpowered (n = 35), definite conclusions about the effect of rhDNase in severe acute asthma cannot be drawn. We cannot exclude the possibility that rhDNase might have been effective in children with a more severe asthma exacerbation and/or atelectasis, or in those requiring admission to the intensive care unit. A separate study is needed to answer this question. In earlier case reports rhDNase was administered to children with a severe asthma exacerbation who also had atelectasis. We had no information about the presence or severity of atelectasis in our population because it was not considered necessary or ethical to perform two chest radiographs during treatment at the emergency department.
A second explanation might be that the amount of DNA present in the mucus was too low for rhDNase to be effective. The average DNA content of mucus in patients with stable asthma is higher than that in healthy controls (7.1 vs 3.6 μg/ml).15 Even higher levels were found in patients with an asthma exacerbation (0.5 mg/ml).6 The DNA content of mucus in patients with asthma is much lower, however, than in those with cystic fibrosis (3–14 mg/ml)16 in whom the beneficial effects of rhDNase have clearly been documented.9
A third explanation could be suboptimal lung deposition of rhDNase in children with bronchial obstruction, resulting in deposition of rhDNase mainly in the more central airways17 and not reaching the peripheral airways. To compensate for suboptimal deposition, patients received a dose of 5 mg (twice the dose used as maintenance treatment in patients with cystic fibrosis). Arguably, it might have been more effective to administer the study medication immediately on arrival in the emergency department or following the first dose of bronchodilators rather than after the second dose, or to use repeated nebulisations of study medication instead of one. However, we think that other timing or dosing frequency would not change the results, since neither the symptom scores at any time points nor any of the secondary end points differed between the groups. Moreover, a single dose of rhDNase has an effect lasting many hours.18
Finally, as diagnosing asthma in preschool children is difficult, part of our study population might have had “exclusive viral wheeze” and not asthma. The exact role of mucus plugging in the pathophysiology of airway obstruction in children with “exclusive viral wheeze” has not been investigated to our knowledge. Our study focused on current emergency clinical practice which does not take into account the child’s asthma phenotype.
Most of the participating hospitals routinely admitted children with an acute asthma exacerbation who required at least two doses of nebulised bronchodilators. It was not therefore meaningful to assess the effect of rhDNase on the admission rate. Even if a longer period of observation in the emergency room had been possible, we probably would not have found a positive effect of rhDNase on the admission rate since the decision to admit a child is based on the symptoms and we found no significant effect of rhDNase on the asthma score over time.
In this study the administration of rhDNase in acute asthma appeared to be safe. It was stopped in one case of temporary desaturation with an increase in dyspnoea and tachypnoea directly after the start of nebulisation. The mechanism of this desaturation is unclear, but we speculate that it might have been caused by the child’s inability to clear mucus effectively after quick liquefaction by rhDNase.
Because our study population reflects the population of children with acute asthma treated in the emergency rooms of district and tertiary care hospitals, our results can be generalised to the large majority of children with a moderate to severe acute asthma exacerbation. Further studies on the effect of rhDNase in children with acute asthma requiring intensive care or with large atelectasis are still needed.
In conclusion, our study shows that a single dose of nebulised rhDNase in addition to nebulised bronchodilators and systemic steroids is not effective in the treatment of children with moderate to severe acute asthma.
Acknowledgments
The authors thank the children, their parents and the staff of the eight participating centres.
REFERENCES
Footnotes
-
Funding: Roche BV, The Netherlands provided an unrestricted grant for this study and financed the study medication. Pari GmbH, Germany donated the nebulising equipment. The study sponsors were not involved in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
-
Competing interests: None.