Article Text

Abstract
Background: Secretory phospholipases A2 (sPLA2) have functions relevant to asthmatic inflammation, including eicosanoid synthesis and effects on dendritic cells and T cells. The aim of this study was to measure sPLA2 activity in patients with stable and acute asthma and to assess potential associations with body mass index (BMI), and plasma cholesterol and vitamin C concentrations.
Methods: Plasma sPLA2 activity and concentrations of cholesterol and vitamin C were measured in 23 control subjects and 61 subjects with stable asthma (42 mild to moderate, 19 severe). In addition, sPLA2 activity was measured in 36 patients experiencing acute asthma and in 22 of these patients after recovery from the acute attack.
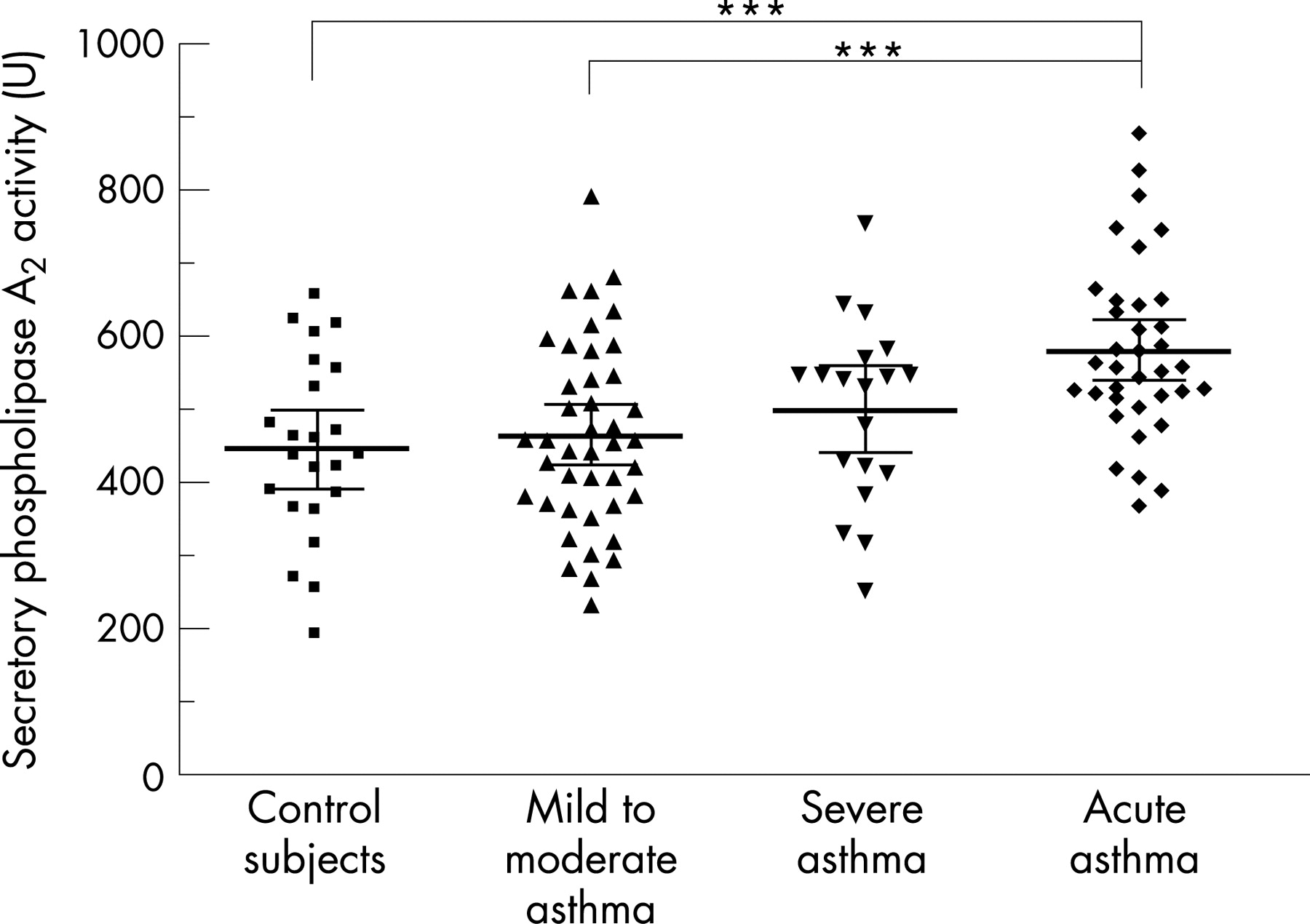
Results: sPLA2 activity was not significantly greater in severe (499.9 U; 95% confidence interval (CI) 439.4 to 560.4) compared with mild to moderate asthmatic subjects (464.8; 95% CI 425.3 to 504.3) or control subjects (445.7; 95% CI 392.1 to 499.4), although it was higher in patients with acute asthma (581.6; 95% CI 541.2 to 622.0; p<0.001). Male gender, high plasma cholesterol, increased BMI and atopy were associated with increased sPLA2 activity, while plasma vitamin C was inversely correlated with sPLA2 activity in patients with stable asthma and in control subjects. There were significant interactions between gender and plasma cholesterol and between gender and vitamin C in relation to sPLA2 activity.
Conclusions: Plasma sPLA2 may provide a biological link between asthma, inflammation, increased BMI, lipid metabolism and antioxidants. Interactions among these factors may be pertinent to the pathophysiology and increasing prevalence of both asthma and obesity.
Statistics from Altmetric.com
Phospholipases A2 (PLA2) are a large group of enzymes that hydrolyse fatty acids, including arachidonic acid, from the sn-2 position of glycerophospholipids, providing the substrate for synthesis of leucotrienes, prostaglandins, platelet activating factor and lysophospholipids that are important in lung inflammation and asthma.1 The PLA2 superfamily also plays crucial regulatory roles in phospholipid metabolism, host defence and signal transduction.2 The secretory phospholipases A2 (sPLA2) are low molecular weight enzymes found in extracellular fluids, including plasma. In humans, there may be as many as six or seven of these calcium dependent enzymes that are resistant to proteolysis and denaturation.3 4 A role for these sPLA2 enzymes in inflammatory processes has been suggested by studies showing increased serum sPLA2 activity in acute pancreatitis and rheumatoid arthritis.5 6
Asthma is a chronic inflammatory disease, involving T lymphocytes, eosinophils, basophils, neutrophils and mast cells,7 and many of these cells express and release sPLA2.4 8 Furthermore, recent studies indicate that sPLA2 is likely to have numerous biological functions that are relevant to the pathogenesis of asthma, including eicosanoid synthesis,1 4 maturation and migration of dendritic cells,9 10 T cell proliferation11 as well as cytokine and chemokine production by monocytes, macrophages, neutrophils and eosinophils.12–15 However, patient studies directly implicating sPLA2 in the pathophysiology of asthma are limited. Increased serum and leucocyte PLA2 activity has been reported in patients with asthma and rhinitis.16 17 An increase in sPLA2 activity was also observed in nasal lavage following challenge of allergic subjects,18 and in bronchoalveolar lavage fluid following antigen challenge of patients with asthma.19
Recent epidemiological studies have identified associations between obesity and increases in the incidence and prevalence of asthma.20 21 Therefore, lipid parameters such as plasma triglyceride and cholesterol concentrations that are associated with increased body mass index (BMI)22 may also be associated with the activities of lipid modifying enzymes, such as sPLA2 in patients with asthma. Furthermore, the antioxidant vitamins C and E appear to inhibit the oxidative modification of lipoproteins that are substrates for sPLA2.23 24
We recently developed an assay for a low molecular weight sPLA2 in serum, and showed that this enzyme was associated with high density lipoproteins and was strongly correlated with total cholesterol, low density lipoprotein cholesterol and triglyceride concentrations in healthy subjects.25 The aim of the present study was to extend these findings by comparing sPLA2 activity in patients with stable, mild to moderate or severe asthma, or acute exacerbations of asthma, with that in healthy control subjects. In addition, we assessed the potential associations between sPLA2 activity and BMI, plasma total cholesterol and plasma vitamin C concentrations in patients with stable asthma and in control subjects.
METHODS
Subjects
Patients with stable asthma were recruited from the databases of the Lung Institute of Western Australia and Sir Charles Gairdner Hospital, Perth. These institutions treat patients with mild to moderate to severe asthma from the entire Perth metropolitan area. All patients had been diagnosed as asthmatic by a respiratory physician and were categorised as having severe asthma if they met at least four of the following criteria, which were modifications of the National Asthma Education and Prevention Program, Expert Panel Report II guidelines26: (1) β2 agonist use ⩾3 times per day, on most days in the previous 3 months, (2) regular inhaled corticosteroid use (⩾2000 μg beclomethasone equivalent/day) in the previous 3 months, (3) use of oral corticosteroids within the past 12 months, (4) hospital admission for asthma in the previous 12 months, (5) ⩾3 unplanned visits to a general practitioner in the previous 12 months because of asthma exacerbations, (6) daily asthma symptoms including cough, wheeze, chest tightness and breathlessness when asthma was unstable in the previous 3 months and (7) nocturnal awakening due to asthma symptoms more than twice a week in the past 3 months. All patients were studied when their asthma was stable, and the severity categorisation was designed to reflect their chronic long term asthma severity. On this basis, 19 patients were categorised as having severe asthma, while the 42 patients who did not meet the criteria for severe asthma were categorised as having mild to moderate asthma.
In order to recruit non-asthmatic control subjects from a comparable population, letters inviting subjects to participate were mailed to addresses randomly selected from the Perth metropolitan telephone directory. The 23 non-asthmatic subjects who were recruited completed a brief questionnaire relating to their general health status. All patients and control subjects were recruited within a 6 month period. They completed a lung function test, and their atopic status was assessed by skin prick testing. A weal diameter ⩾3 mm was considered to be a positive reaction. A blood sample was taken and placed on ice for transfer to the laboratory within 2 h. The characteristics of the patient and control groups are presented in table 1.
For the study of plasma sPLA2 activity in acute asthma, patients were recruited on presentation to the emergency department at Sir Charles Gairdner Hospital with an acute exacerbation of their asthma. A blood sample was taken while the patient was being assessed and before oral corticosteroid treatment was commenced. These patients were followed-up 6–8 weeks later when their lung function had returned to normal or to their previous best, and at this time a second blood sample was taken. The characteristics of the patients recruited for the acute asthma study are presented in table 1. All of the research undertaken was approved by the Sir Charles Gairdner Hospital Human Research Ethics Committee and all subjects gave informed consent.
Assay of plasma sPLA2 activity
Plasma samples were purified on heparin–sepharose affinity columns (HiTrap Heparin HP; Amersham Biosciences, Sydney, Australia) that were prewashed with 50 mM Tris-HCl, pH 7.5, before application of the plasma sample (0.5 ml). Columns were washed with 50 mM Tris-HCl, pH 7.5, 150 mM NaCl, and sPLA2 activity was eluted with 0.5 ml of 50 mM Tris-HCl, 1 M KCl. sPLA2 activity in purified plasma samples was assayed using 4-nitro-3-octanoyloxy-benzoic acid as substrate, as described previously.25 Briefly, substrate solution (180 μl, 2 mM final concentration) and purified plasma (20 μl) were incubated in microplate wells at room temperature for 2 h. Absorbances at 425 and 600 nm (to correct for turbidity in the sample) were then measured on a spectrophotometer (Molecular Devices, Sunnyvale, California, USA). A unit (U) of sPLA2 activity was defined as nmol of product formed by 1 ml of plasma in a 1 h incubation and was calculated as
[(OD425nm − OD600nm) × 78.62 × 25]
where 78.62 is the nmol of product producing an OD425 of 1.0 in 0.2 ml and 25 is the correction factor for 20 μl of plasma to 1 ml and a 2 h incubation to 1 h.
Cholesterol and vitamin C concentrations
These analyses were performed in the Department of Clinical Biochemistry, PathWest, Perth, Western Australia. Total plasma cholesterol was determined by a standard automated spectrophotometric method. For vitamin C analyses, plasma was deproteinised with dithiothreitol-EDTA-perchloric acid, and ascorbic acid in the supernatant was separated and quantified by reverse phase high pressure liquid chromatography using external standards (0–227 μM). Ascorbic acid measurements were not corrected for recovery, which was ∼90%. The inter-analysis precision coefficient of variation was 5.4%.
Data analysis and statistics
Data are expressed as means with 95% confidence interval (CI), SD or SEM. Differences between group mean values were assessed for statistical significance by one way ANOVA followed by Bonferroni’s multiple comparison test or by the unpaired t test as appropriate. In univariate analyses, Pearson’s correlation was used to assess the statistical significance of associations between parameters of interest. In order to identify significant independent predictors of sPLA2 activity after adjusting for confounding factors, and to assess interactions, a multiple linear regression analysis was performed. The independent variables entered into the model were gender, age, BMI, severe asthma, atopy, use of inhaled corticosteroids, smoking status, and plasma cholesterol and vitamin C concentrations. In addition, interactions between gender and cholesterol concentration, gender and vitamin C concentration and BMI and cholesterol concentration were assessed. All statistical analyses were performed using SPSS for Windows V.11.5 (SPSS Inc, Chicago, Illinois, USA) and a p value <0.05 was considered significant.
RESULTS
The characteristics of the patients with asthma and the control subjects are presented in table 1. Plasma sPLA2 activity in patients with stable, mild to moderate (464.8 U; 95% CI 425.3 to 504.3) or severe asthma (499.9 U; 95% CI 439.4 to 560.4) did not differ significantly from that in control subjects (445.7 U; 95% CI 392.1 to 499.4) (fig 1). However, among these control subjects and patients with stable asthma, sPLA2 activity was significantly greater in atopic (483.5 U; 95% CI 455.3 to 511.6) than in non-atopic subjects (419.7 U; 95% CI 349.6 to 489.7; p<0.05) and in males (501.3 U; 95% CI 455.4 to 547.3) compared with females (442.1 U; 95% CI 409.4 to 474.8; p<0.05). sPLA2 activity in the 15 patients with asthma who were not using inhaled corticosteroids (516.5 U; 95% CI 452.0 to 581.1) was not significantly different compared with that in the 46 patients who were (462.4 U; 95% CI 424.5 to 500.4), and there was no correlation between inhaled corticosteroid dose and sPLA2 activity.
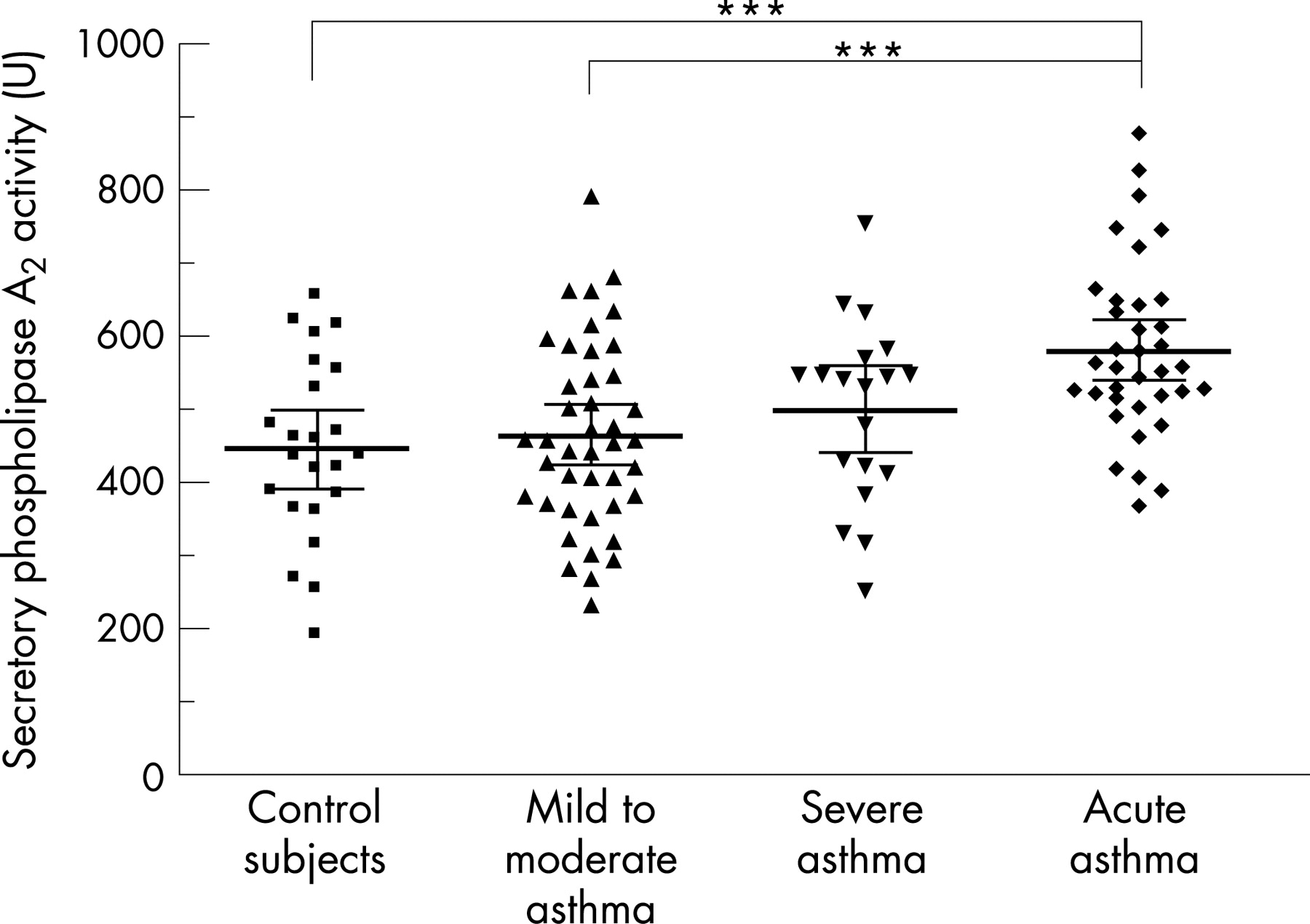
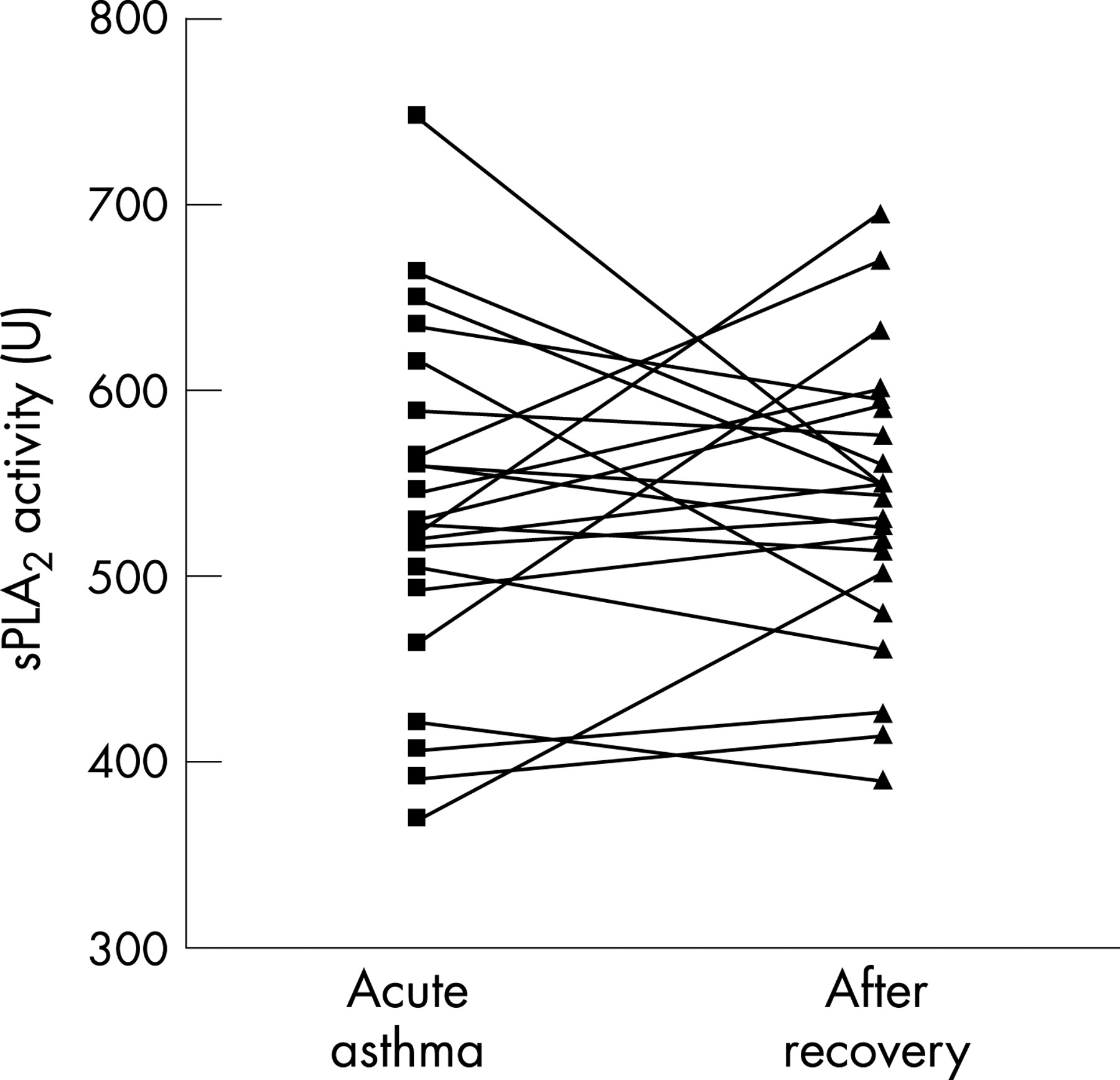
sPLA2 activity in patients presenting with an acute exacerbation of asthma (581.6 U; 95% CI 541.2 to 622.0) was significantly higher than that in control subjects or in patients with mild to moderate asthma (p<0.001) (fig 1). However, mean plasma sPLA2 activity measured in 22 of the 36 patients after recovery from the acute attack (540.2 U; 95% CI 506.0 to 574.4) was not different to that measured during the acute asthma episode (536.3 U; 95% CI 494.9 to 577.7) (fig 2). While sPLA2 activity decreased substantially after recovery in some patients, it increased or remained unchanged in others. There was no correlation between inhaled corticosteroid dose and sPLA2 activity during or after recovery from the acute attack.

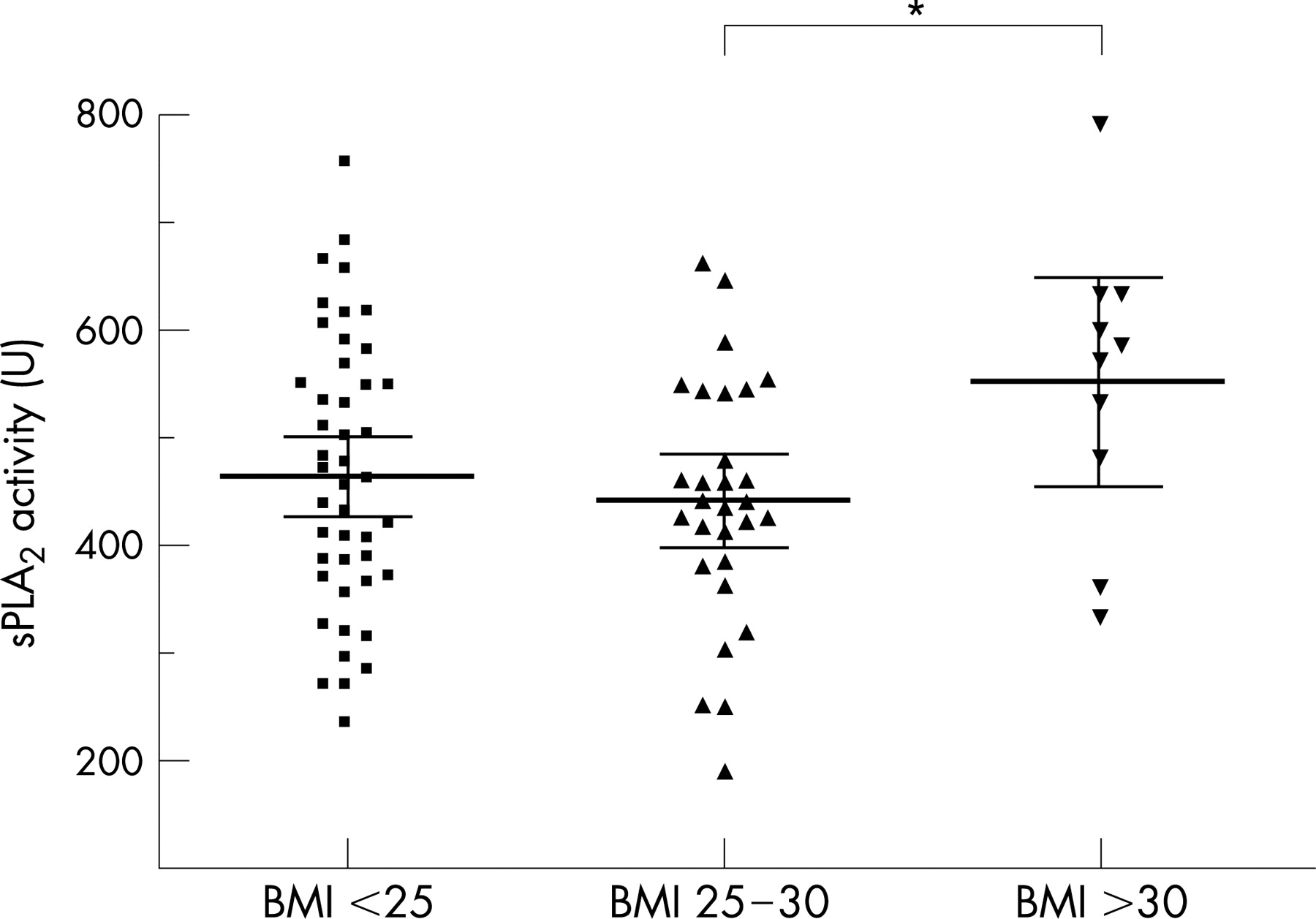
Mean BMI in patients with stable, severe asthma (28.8; 95% CI 25.4 to 32.1) was significantly higher than that of control subjects (23.8; 95% CI 22.3 to 25.4; p<0.02). sPLA2 activity was significantly greater in subjects who were clinically obese (BMI >30: 552.4 U; 95% CI 455.6 to 649.1) compared with those who were overweight (BMI 25–30: 442.1; 95% CI 399.2 to 485.0; p<0.05) (fig 3). Plasma total cholesterol concentration was significantly higher in subjects with BMI >25 (5.78 mM; 95% CI 5.42 to 6.13) compared with those with BMI ⩽25 (5.24 mM; 95% CI 4.98 to 5.50; p<0.02). Plasma cholesterol also tended to be higher in patients with severe asthma (5.96 mM; 95% CI 5.46 to 6.46) compared with controls (5.26 mM; 95% CI 4.89 to 5.63) or patients with mild to moderate asthma (5.41 mM; 95% CI 5.09 to 5.73), although the differences were not statistically significant.

Plasma vitamin C concentration was significantly lower in patients with severe asthma (33.1 μM; 95% CI 23.4 to 42.8) compared with those with mild to moderate asthma (49.6; 95% CI 43.5 to 55.6; p = 0.01) and control subjects (49.9; 95% CI 41.4 to 58.5; p = 0.02) (fig 4). Vitamin C concentration was also lower in males (38.4 μM; 95% CI 31.1 to 45.7) compared with females (51.4 μM; 95% CI 46.0 to 56.7; p<0.005) (fig 4).

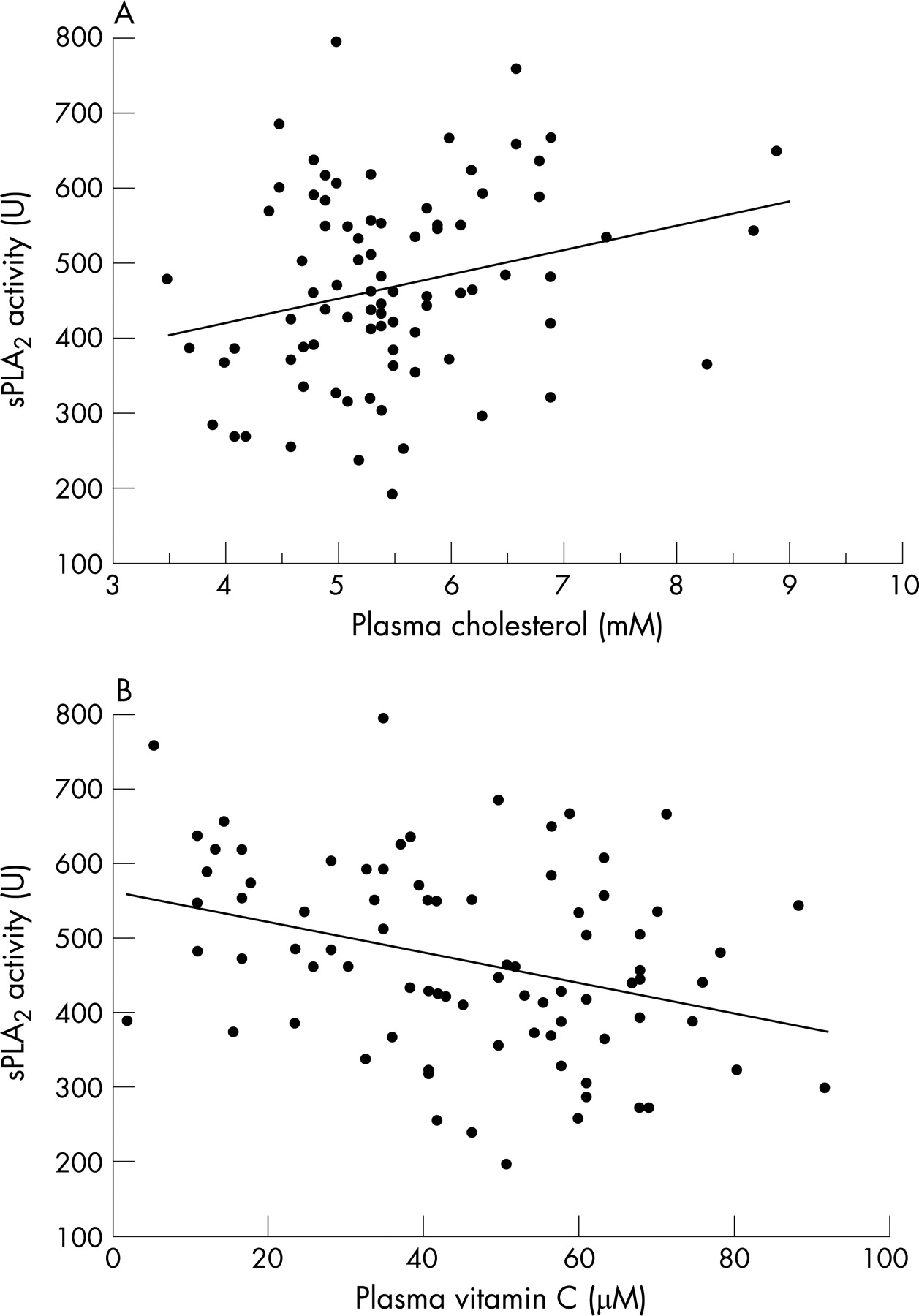
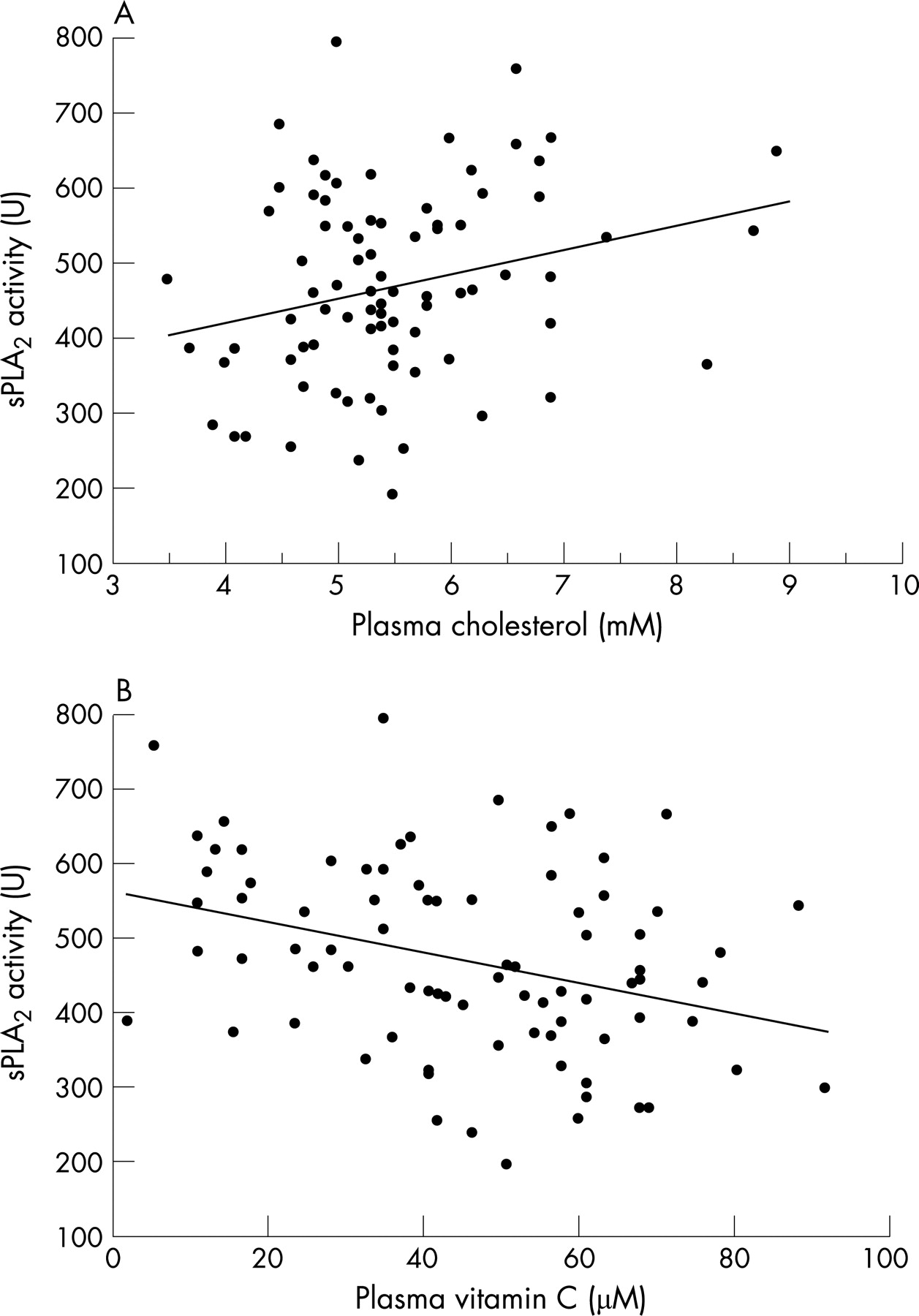
Univariate analysis of the data showed weak but statistically significant positive correlations between sPLA2 activity and BMI (r = 0.23; p<0.05) and also between sPLA2 activity and cholesterol (r = 0.26; p<0.02) (fig 5A) in control subjects and in those with stable asthma. The correlation between sPLA2 activity and cholesterol was, however, stronger in patients with severe asthma (r = 0.62; p = 0.005). In contrast with these positive associations, sPLA2 activity was inversely correlated with plasma vitamin C concentration (r = −0.33; p = 0.002) (fig 5B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A multiple linear regression analysis to identify factors independently associated with sPLA2 activity in the control subjects and in patients with stable asthma showed that male gender and higher plasma cholesterol were independently associated with greater sPLA2 activity (table 2). In addition, there were indications that atopy and increased BMI, although not reaching statistical significance in this model, were associated with increased sPLA2 activity. Although there was no independent association between sPLA2 activity and plasma vitamin C, there were significant interactions between gender and plasma vitamin C and also between gender and plasma cholesterol in relation to sPLA2 activity.
DISCUSSION
Cytosolic PLA2 plays a major role in the production of arachidonic acid derived lipid mediators, such as prostaglandins and leucotrienes, that contribute to airway inflammation in asthma.1 However, recent evidence suggests that secretory PLA2 isozymes may also have an important role in eicosanoid synthesis and amplification of the inflammatory process, both directly and by functional coupling with cytosolic PLA2 and cyclooxygenase-2.27–29 In the present study, the activity of potentially proinflammatory plasma sPLA2 enzymes with heparin binding domains was measured in patients with stable asthma and patients presenting with acute asthma, in whom upregulation of inflammatory pathways might be expected. We previously measured “total” sPLA2 activity in unpurified serum samples25 whereas in the present study samples were purified on heparin affinity columns and the sPLA2 activity measured was therefore much less. However, it was more likely to represent the activities of groups IIA, IID and V sPLA2 that interact with heparan sulphate proteoglycans in lipid rafts, bringing them into contact with enzymes such as cyclooxygenase and 5-lipoxygenase that are important for the generation of eicosanoid mediators in asthma.4
The observation that plasma sPLA2 activity was not significantly increased in patients with stable, severe asthma compared with those with mild to moderate asthma and control subjects may suggest that this sPLA2 activity is not proinflammatory or that inflammatory pathways were not upregulated in these patients with stable, severe asthma. However, there was a trend towards increased sPLA2 activity in patients with severe asthma, and a power calculation indicated that 80 subjects would have been required in each group for the measured difference between controls and patients with severe asthma to be considered statistically significant. Therefore, another explanation for the lack of a significant difference in sPLA2 activity between these two groups is that the study was insufficiently powered. There is one previous report that serum PLA2 activity was significantly increased in patients with stable asthma.16 However, in that study, it is likely that total sPLA2 activity was measured, rather than the activity of heparin binding isoforms, and it is possible that other isoforms of sPLA2 excluded by heparin affinity purification may be differentially expressed in patients with asthma. Furthermore, the patients in that study had not received any corticosteroid treatment, which may reduce sPLA2 activity in patients with stable asthma, either directly by inhibiting sPLA2 expression30 or indirectly by moderating inflammation.31
The possibility that there was a real increase in sPLA2 activity in patients with severe asthma, but that the present study was inadequately powered to detect this increase, is supported by the finding of a significant increase in plasma sPLA2 activity in patients experiencing an acute exacerbation of asthma. This increase in plasma sPLA2 activity in patients with acute asthma is also consistent with previous findings in patients with acute appendicitis, rheumatoid arthritis and coronary artery disease.6 32 33 The link between sPLA2 and inflammation is further supported by the finding in the present study of a probable association between atopy and increased sPLA2 activity. Atopy may be associated with an increase in airway and/or systemic inflammation, as evidenced by the increase in exhaled nitric oxide in atopic subjects.34 The mechanisms that might lead to an increase in plasma sPLA2 activity and the source of this enzyme are uncertain, but one possibility is that sPLA2 is an acute phase protein, released as a consequence of systemic inflammation, together with other molecules, such as interleukin 6 (IL6) and C reactive protein.27 35 Increased sPLA2 activity may also result from localised production and release of sPLA2 in the respiratory tract, as indicated by the finding of increased sPLA2 activity in bronchoalveolar lavage fluid after allergen challenge of patients with asthma.19 In addition, eosinophils contain significant amounts of sPLA2,8 which may be secreted in the lungs and peripheral blood of patients with asthma. However, a recent trial showed that a sPLA2 inhibitor had no effect on early or late forced expiratory volume in 1 s following allergen challenge of atopic asthmatics.36
It is also possible that sPLA2 activity is genetically determined, and is high in patients who are prone to acute asthma episodes. As such, sPLA2 may be a potential biomarker of patients who are more likely to experience acute exacerbations. Furthermore, sPLA2 activity was not reduced in many of the 22 patients in whom it was measured after recovery from the acute episode of asthma, suggesting that treatment, including corticosteroids, may not suppress inflammatory processes such as sPLA2 activity in all patients with asthma.
The previously observed correlation between sPLA2 activity and total cholesterol25 was confirmed in the present study, but the correlation was much stronger in patients with severe asthma. In addition, mean BMI was significantly higher in patients with severe asthma, while plasma cholesterol was increased in overweight subjects and sPLA2 activity was greater in obese subjects and positively associated with increased BMI. These results are strongly suggestive of interactions between increased BMI, dysregulation of lipid metabolism and more severe asthma, lending support to the large number of recent epidemiological studies that have reported associations between the prevalence and incidence of asthma, and increased BMI in both adults and children (reviewed by Ford21).
There are a number of plausible mechanisms that may explain the association between increased BMI and asthma.20 In obese subjects, adipose tissue may contribute significantly to inflammation through production of IL6, tumour necrosis factor α (TNFα), transforming growth factor β1 and eotaxin, as well as the adipokine, leptin, which has been shown to regulate T cell proliferation and activation.20 37 The results from the present study suggest that upregulation of sPLA2 may be a proinflammatory consequence of increases in BMI and adipose tissue metabolism, similar to the increases in other inflammation associated molecules, such as TNFα, IL6, leptin and C reactive protein, that have been observed in obese as well as asthmatic subjects.37–40 However, it is interesting that in this study, sPLA2 activity was higher in atopic subjects whereas increased levels of C reactive protein were associated with non-allergic asthma.40 Upregulation of sPLA2 activity may have important functional consequences for inflammatory processes in both obesity and asthma. Specifically, lipoprotein associated sPLA2 may increase the catabolism of phospholipids to biologically active lipids, including prostaglandins, leucotrienes, platelet activating factor and lysophospholipids, which are likely to play a role in chronic inflammation in asthmatic and obese subjects. In addition, sPLA2, like leptin, has been implicated in T cell proliferation and cytokine and chemokine production.11–15
sPLA2 activity was inversely correlated with plasma vitamin C concentration, although the latter was not an independent predictor of lower sPLA2 activity. Importantly, however, there was a marked gender interaction, with sPLA2 activity being higher and vitamin C concentration lower in males compared with females. Lower plasma vitamin C concentrations may contribute to increased oxidative modification of lipoproteins23 and a resultant increase in the activity of enzymes such as sPLA2 that catalyse the hydrolysis of lipoproteins.24 In contrast, the multiple regression analysis performed in the present study indicated that the positive association between sPLA2 activity and plasma cholesterol was stronger in females than in males. This is in keeping with observations from a number of studies suggesting a stronger association between asthma and obesity in females than in males.20 21 Factors such as the influence of female sex hormones,20 low dietary intake of vitamin C by male asthmatics and lower plasma concentrations of vitamin C in severe asthma,41 are likely to be confounding factors in the associations among asthma, increased BMI, sPLA2 activity and cholesterol and vitamin C concentrations.
In conclusion, this study has demonstrated a significant upregulation of plasma sPLA2 activity in patients with acute asthma. In addition, the study has identified potentially important associations between sPLA2 activity, increased plasma cholesterol, increased BMI and atopy, as well as gender interactions in the positive association of cholesterol and the inverse association of vitamin C with sPLA2 activity. sPLA2 may therefore be one of the biological links between asthma, inflammation, increased BMI, lipid metabolism and antioxidants. Further studies, possibly with larger numbers of subjects, are required to unravel these complex interactions and the mechanisms by which they may contribute to the pathophysiology and increasing prevalence of both asthma and obesity.
Acknowledgments
The authors thank Dr Roberta Littleford, Lung Institute of Western Australia, and Dr John Beilby, Clinical Biochemistry, PathWest, Nedlands, Western Australia, for their assistance.
REFERENCES
Footnotes
Competing interests: None.