Article Text

Abstract
Backround: A fall in FEV1 of ⩾10% following bronchoprovocation (eucapnic voluntary hyperventilation (EVH) or exercise) is regarded as the gold standard criterion for diagnosing exercise induced asthma (EIA) in athletes. Previous studies have suggested that mid-expiratory flow (FEF50) might be used to supplement FEV1 to improve the sensitivity and specificity of the diagnosis. A study was undertaken to investigate the response of FEF50 following EVH or exercise challenges in elite athletes as an adjunct to FEV1.
Methods: Sixty six male (36 asthmatic, 30 non-asthmatic) and 50 female (24 asthmatic, 26 non-asthmatic) elite athletes volunteered for the study. Maximal voluntary flow-volume loops were measured before and 3, 5, 10, and 15 minutes after stopping EVH or exercise. A fall in FEV1 of ⩾10% and a fall in FEF50 of ⩾26% were used as the cut off criteria for identification of EIA.
Results: There was a strong correlation between ΔFEV1 and ΔFEF50 following bronchoprovocation (r = 0.94, p = 0.000). Sixty athletes had a fall in FEV1 of ⩾10% leading to the diagnosis of EIA. Using the FEF50 criterion alone led to 21 (35%) of these asthmatic athletes receiving a false negative diagnosis. The lowest fall in FEF50 in an athlete with a ⩾10% fall in FEV1 was 14.3%. Reducing the FEF50 criteria to ⩾14% led to 13 athletes receiving a false positive diagnosis. Only one athlete had a fall in FEF50 of ⩾26% in the absence of a fall in FEV1 of ⩾10% (ΔFEV1 = 8.9%).
Conclusion: The inclusion of FEF50 in the diagnosis of EIA in elite athletes reduces the sensitivity and does not enhance the sensitivity or specificity of the diagnosis. The use of FEF50 alone is insufficiently sensitive to diagnose EIA reliably in elite athletes.
- EIA, exercise induced asthma
- EVH, eucapnic voluntary hyperventilation
- FEF50, forced expiratory flow at 50% of vital capacity
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- asthma
- sensitivity
- diagnosis
- eucapnic voluntary hyperventilation
- elite athletes
Statistics from Altmetric.com
- EIA, exercise induced asthma
- EVH, eucapnic voluntary hyperventilation
- FEF50, forced expiratory flow at 50% of vital capacity
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
Exercise induced asthma (EIA) occurs in approximately 90% of chronic asthmatics1 and has previously been reported to occur in 7–50% of athletic individuals.2–6 Asthmatic elite athletes currently require evidence of asthma to obtain a therapeutic use exemption certificate which enables them to use therapeutic doses of inhaled β2 agonists in and out of competition.7 EIA has previously been diagnosed by a number of challenge methods including exercise,8,9 eucapnic voluntary hyperventilation (EVH),10,11 methacholine,12,13 histamine,14 saline,15 and mannitol.16,17 The International Olympic Committee’s Medical Commission (IOC-MC) considers positive tests from exercise, EVH, saline, histamine, and methacholine challenges as evidence of EIA. Methacholine and histamine, however, have been shown to be less specific than exercise for EIA diagnosis.16,18,19 Exercise and EVH challenges are regarded as the most specific methods of diagnosing EIA in elite athletes.11
In all EIA tests recognised by the IOC-MC, forced expiratory volume in 1 second (FEV1) is the parameter by which changes in maximal expiratory function are assessed, but no “gold standard” methodology exists for athletes or non-athletes.20 Previous studies that have used FEV1 to diagnose EIA have suggested using falls in FEV1 ranging from 7% to 20% as cut off criteria.21–23 The work carried out by Helenius et al23 suggests that a fall of 10% in FEV1 following an exercise test is not sensitive enough to diagnose EIA in elite athletes. Despite the absence of a “gold standard” methodology for diagnosing EIA in athletes, the IOC-MC has ruled that an exercise or EVH challenge is positive for EIA when the FEV1 falls ⩾10% from the baseline measurement.
It is possible that the addition of other measurements of expiratory lung function may provide greater sensitivity in the diagnosis of EIA. For example, forced expiratory flow between 25–75% of vital capacity (FEF25–75) has been used in conjunction with FEV1 to aid the diagnosis of EIA in children24,25 and athletes.8,26 Implicitly, FEV1 measures expiratory flow at high and mid lung volumes, whereas FEF25–75 and forced expiratory flow at 50% of vital capacity (FEF50) are markers of expiratory flow through middle lung volumes. It has been suggested that FEF25–75 and FEF50 are more sensitive to airway obstruction in the small airways than FEV1.27,28 Custovic et al24 noted that cut off points for EIA in children (defined as the normal group mean value −2 SD) occurred with a fall in FEV1 of >10% and a fall in FEF25–75 of >26%. In this study, the combined application of FEV1 and FEF25–75 criteria enabled detection of all subjects with EIA. Furthermore, using both FEV1 and FEF25–75 criteria, none of the subjects with allergic rhinitis or dermatitis presented with EIA. The fall in FEV1 after exercise in children with allergic rhinitis was within the normal range (⩽2SD), but with a significantly lower mean value than control subjects. The study by Custovic et al24 therefore provides promising evidence to support the addition of mid expiratory flow rates to FEV1 in the diagnosis of EIA in children that might also be applied to elite athletes. FEF50 and FEF25–50 measurements are highly correlated and the ratio of the two is reasonably constant. Based on this finding, Bar-Yishay et al29 suggested that reporting both measurements is unnecessary, and they suggested that FEF50 should be the preferred measure. This preference was based on the argument that FEF50 is easily and directly determined while FEF25–50 is a calculated parameter that is affected by the spirometer manufacturer’s choice of algorithm.
The purpose of the present study was to examine the role of FEF50 as an adjunct to FEV1 in the diagnosis of EIA in elite athletes following a bronchoprovocation challenge.
METHODS
Following ethical approval from Harrow local research ethics committee, 66 male elite summer and winter athletes of mean (SD) age 25.1 (4.9) years, height 180.7 (7.8) cm, body mass 77.3 (12.5) kg and 50 female elite athletes of mean (SD) age 24.3 (5.4) years, height 168.2 (7.9) cm, and body mass 62.6 (9.9) kg who held either a Gold or Silver British Olympic Association passport (indicating current or potential Olympic competitive standard) provided written informed consent and volunteered for the study. Of the athletes who participated in this study, 83 had a previous diagnosis of EIA and where using asthma medication. The other 33 athletes had reported symptoms of EIA to a sports physician who had referred them to be tested for EIA. The testing took place at the Olympic Medical Institute, Harrow between June 2003 and June 2004. Athletes were tested at least 2 weeks after a respiratory infection and at least 12 hours following a training session.
Each athlete completed either an exercise or EVH challenge. Exercise challenges involved exercising at an intensity of >85% of maximal heart rate for 6–10 minutes in a sport-specific environment.30 EVH challenges consisted of hyperventilating for 6 minutes at a rate of 85% maximal voluntary ventilation (30 × baseline FEV1). The gas inspired during the EVH challenge was a medical gas containing 21% O2, 5% CO2 and 74% N2.31 For both exercise and EVH challenges, maximal flow-volume loops were measured before and at 3, 5, 10 and 15 minutes after stopping exercise or EVH using a digital spirometer (MicroLab ML3500, Micro Medical Ltd, Rochester, UK) which met ATS guidelines. The lowest values of FEV1 and FEF50 following either exercise or EVH were recorded and the change was calculated (Δ). A ΔFEV1 of ⩾−10% and ΔFEF50 of ⩾−26% were considered cut off criteria for EIA diagnosis.24
RESULTS
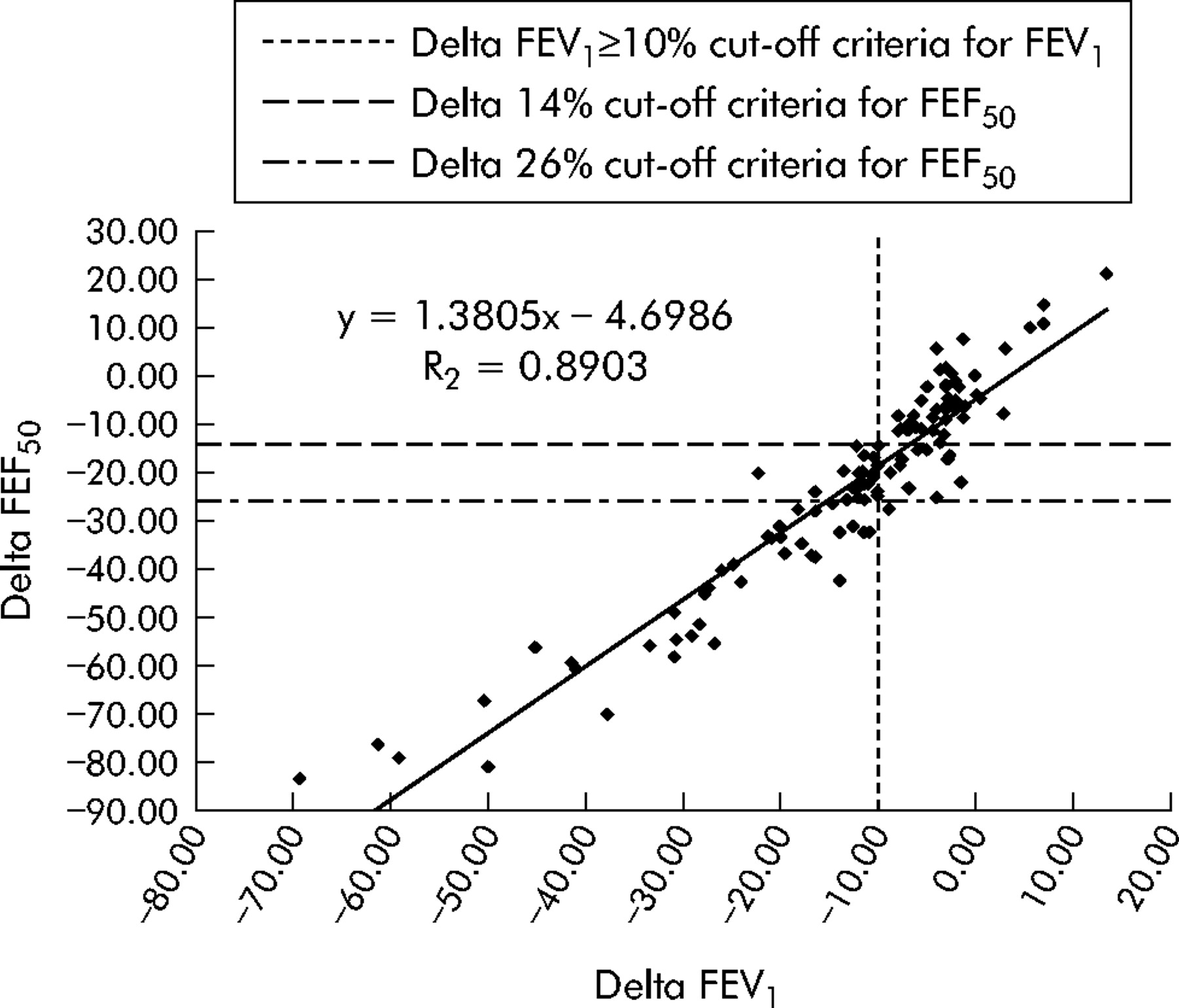
There was a strong positive correlation between ΔFEV1 and ΔFEF50 following bronchoprovocation (r = 0.94, p = 0.000). Sixty athletes (52%) had a ΔFEV1 fall of ⩾10% leading to the diagnosis of EIA (fig 1). Using the FEF50 criteria alone led to 21 (35%) asthmatic athletes receiving a false negative diagnosis; thus, 39 athletes met both FEV1 and FEF50 criteria. The lowest fall in ΔFEF50 in an athlete with a ⩾10% fall in FEV1 was 14.3%. Reducing the FEF50 criterion to a ⩾14% fall included 13 athletes whose ΔFEV1 was not ⩾10% (mean ΔFEV1 = 5.7, range −8.9 to −1.5). Only one athlete had a ⩾26% fall in FEF50 in the absence of a ⩾10% in FEV1 (ΔFEV1 = 8.9%).

{kind=link}
Delta FEV1 versus delta FEF50.
Of the 83 athletes with a previous diagnosis of EIA, 33 failed to develop EIA (ΔFEV1 <10%) following bronchoprovocation challenge. Of the 33 athletes who had been referred for testing but had no previous diagnosis of EIA, 10 athletes presented with EIA following bronchoprovocation.
The values for FEF50 and forced vital capacity (FVC) before and after bronchoprovocation challenge are shown in table 1. FEF50 (p = 0.000) and FVC (p = 0.000) were significantly lower after bronchoprovocation in the asthmatic athletes. There was no significant change in FEF50 or FVC before and after bronchoprovocation challenge in athletes who did not have a fall in FEV1 of ⩾10%.
Mean (SD) changes in FEF50 and FVC following bronchoprovocation challenge
The specificity, sensitivity, predictive value of positive test and efficiency of FEF50 cut off criteria of 26% and 14% are shown in tables 2, 3 and 4, respectively.
True and false positive and negative diagnoses based on FEF50 cut off value of 26%
True and false positive and negative diagnoses based on FEF50 cut off value of 14%
Effectiveness of FEF50 cut off criteria of 26% and 14%
DISCUSSION
This study shows that the addition of FEF50 reduces the sensitivity of EIA diagnosis following exercise or EVH challenge. Of the 60 athletes who were diagnosed with EIA using IOC-MC criteria of a ⩾10% fall in FEV1, 21 (35%) would have received a false negative diagnosis using a combination of FEV1 and FEF50 falls. Furthermore, only one athlete exceeded the criterion for FEF50 but not for FEV1. Our study therefore suggests that FEF50 does not improve the diagnosis of EIA in elite athletes using the IOC-MC criteria.
In previous studies, measurements of FEF25–75 have been used to supplement FEV1 in the diagnosis of EIA in children24,25 and athletes.8,26 The studies conducted on children have supported the addition of FEF25–75 measurements to improve the diagnosis of EIA. It has been suggested that FEF25–75 is a more sensitive measure of obstruction in the small airways than FEV1.32 Thus, EIA may be a disease that consistently affects the expiratory flow through the small airways. Fonseca-Guedes et al25 noted that only 60% of children with “intermittent” EIA met the criteria for both FEV1 and FEF25–75 compared with 94.4% of children with “severe persistent” EIA. They suggested that FEF25–75 is more likely to fall significantly than FEV1 in children with mild EIA. Our data do not agree with this finding and suggest that FEV1 is more likely to fall significantly in athletes with mild asthma. Indeed, only one athlete had a significant fall in FEF50 (⩾26%) in the absence of a significant fall in FEV1, while 21 athletes had a significant fall in FEV1 (⩾10%) in the absence of a significant fall in FEF50. Only 39 athletes met both criteria for FEF50 and FEV1, which would have resulted in 21 (35%) athletes (who met FEV1 criteria) receiving a false negative diagnosis for EIA. The reduced sensitivity found following the inclusion of the FEF50 measurement suggests that, in elite athletes with mild EIA, expiratory airflow is just as likely to be restricted in the larger airways as in the smaller airways. It is therefore appropriate to assess expiratory flow using an index of function for both the larger and smaller airways of the lung—that is, FEV1.
A number of studies have examined the diagnosis of EIA in athletes but they have not specifically used mid-expiratory flow rates as a criterion for making the diagnosis. Rundell et al8 suggested that a fall in FEF25–75 of 14% is significant in the diagnosis of EIA in winter athletes. This lower limit was calculated by taking the mean post exercise change from baseline spirometry and subtracting 2 standard deviations. Lowering the FEF50 cut off value in our data to ⩾14% resulted in an increase in the sensitivity but a decrease in the specificity from 98% to 77%. Using a 14% cut off value, 13 athletes would have been diagnosed with EIA who did not meet the IOC-MC criterion of a 10% fall in FEV1 from baseline values.
A further problem associated with the use of FEF50 as a criterion measurement is that its reliability is dependent upon the constancy of FVC. Our results show that the mean fall in FEF50 following bronchoconstriction was accompanied by a mean fall in FVC in athletes with EIA. The fall in FEF50 seen in some of athletes following a bronchoprovocation test may therefore be partially attributable to a reduction in FVC. The reduction in FVC in asthmatic athletes may be due to the prolongation and discomfort associated with exhaling to residual volume during bronchoconstriction. Despite standard controls, this may cause the athlete to stop exhaling before reaching residual volume. This shortcoming further undermines the potential value of FEF50 for diagnosing EIA.
In conclusion, the addition of FEF50 to FEV1 reduces the sensitivity of a diagnosis of EIA in elite athletes. Our data suggest that a more global measure of maximal expiratory airflow (FEV1) provides the most sensitive and specific diagnosis of EIA, especially when the severity of the disease is thought to be mild. This would suggest that EIA is a disease that is associated with expiratory flow limitation in the larger and smaller airways of elite athletes. However, methodological issues associated with assessment of FEF50 (reliance upon FVC) mean that this interpretation should be viewed cautiously. The authors suggest that future studies should investigate the efficacy of the IOC-MC criterion of a 10% fall in FEV1 to define a more statistically justified cut off point for the diagnosis of EIA in elite athletes.
REFERENCES
Footnotes
-
Published Online First 16 October 2005
-
The authors are grateful to the European Olympic Committee, UK Sport, British Olympic Medical Trust, Olympic Medical Institute, and Micro Medical Ltd.
-
Competing interests: none declared