Article Text

Abstract
Background: The development of tolerance following the use of long acting β2 agonists in asthmatic patients with either the homozygous arginine (Arg-16) or glycine (Gly-16) genotypes is poorly documented, especially in relation to the acute reliever response to salbutamol in constricted airways. A study was undertaken to evaluate the Arg-16 and Gly-16 genotypes for the acute salbutamol response following methacholine bronchial challenge between the first and last doses of formoterol (FM) and salmeterol (SM) combination inhalers.
Methods: Parallel groups of 10 matched homozygous Arg-16 and 10 homozygous Gly-16 patients completed a randomised, double blind, double dummy, crossover study. Following a 1 week washout period, patients received treatment for 2 weeks with either inhaled budesonide (BUD) 200 µg + FM 6 µg (two puffs twice daily) or inhaled fluticasone propionate (FP) 250 µg + SM 50 µg (one puff twice daily). After washouts and randomised treatments (1 hour after the first and last inhalation) a methacholine challenge was performed followed by salbutamol 200 µg, with recovery over 30 minutes (the primary outcome).
Results: Washout values for forced expiratory volume in 1 second (FEV1), methacholine hyperreactivity, and salbutamol recovery were similar for both treatments and genotypes. Pre-challenge FEV1 values for both genotypes did not differ significantly between the first and last doses of each treatment. Salbutamol recovery as mean (SE) area under the 30 minute time-response curve was significantly delayed (p<0.05) equally in both genotype and treatment groups. There were no differences in salbutamol recovery in either genotype or treatment group.
Conclusion: Acute salbutamol recovery in methacholine constricted airways was significantly delayed to a similar degree in both genotypes due to cross tolerance induced by FM or SM.
- BUD, budesonide
- FEV1, forced expiratory volume in 1 second
- FM, formoterol
- FP, fluticasone propionate
- PEF, peak expiratory flow
- SM, salmeterol
- asthma
- formoterol
- genotype
- salbutamol
- salmeterol
Statistics from Altmetric.com
- BUD, budesonide
- FEV1, forced expiratory volume in 1 second
- FM, formoterol
- FP, fluticasone propionate
- PEF, peak expiratory flow
- SM, salmeterol
The development of tolerance following the use of long acting β2 agonists in asthmatic patients with either the homozygous arginine (Arg-16) or glycine (Gly-16) genotypes is poorly understood, especially with respect to the acute reliever response to salbutamol in constricted airways. In vitro, using transfected cell lines, the Gly-16 genotype has been shown to be associated with an increased β2 agonist promoted downregulation of β2 adrenoceptors1,2 while, in vivo, this genotype has been shown to be associated with enhanced bronchodilator tolerance to both short and long acting β2 agonists.3–5 Other in vivo data have suggested that the Arg-16 genotype is associated with worse outcomes after exposure to regular short acting β2 agonist in terms of peak expiratory flow (PEF) and asthma exacerbations.6,7 No previous studies have compared the genotypes in terms of tolerance development between the first and last dose of β2 agonist.
Long acting β2 agonists in conjunction with inhaled corticosteroids are advocated in current guidelines to improve asthma control at step 3 in patients with moderate to severe persistent asthma.8,9 Blunting of the acute response to salbutamol after methacholine challenge occurs following the use of long acting β2 agonists despite concomitant inhaled corticosteroids.10,11 However, there are currently no prospective data directly comparing the two homozygous genotypes at position 16, particularly in patients receiving long acting β2 agonists such as formoterol (FM) and salmeterol (SM) in combination inhalers with inhaled corticosteroids.
We therefore compared matched groups of patients expressing the homozygous Arg-16 and homozygous Gly-16 genotypes in terms of acute salbutamol recovery following methacholine bronchial challenge between the first and last doses of FM and SM combination inhalers.
METHODS
Patients
Twenty patients who were homozygous for either the Arg-16 or Gly-16 genotypes were identified from our database. Eligible patients were non-smoking moderate persistent asthmatics8 who had been stable for at least 3 months before the study and none had received a course of oral corticosteroids or antibiotics during this period. Patients were required to exhibit hyperreactivity to methacholine on bronchial challenge testing with a provocative dose causing a 20% reduction from baseline FEV1 (PC20) of less than 4.0 mg/ml. Informed consent was obtained from all patients and the Tayside Committee on Medical Research Ethics approved the study.
Study design
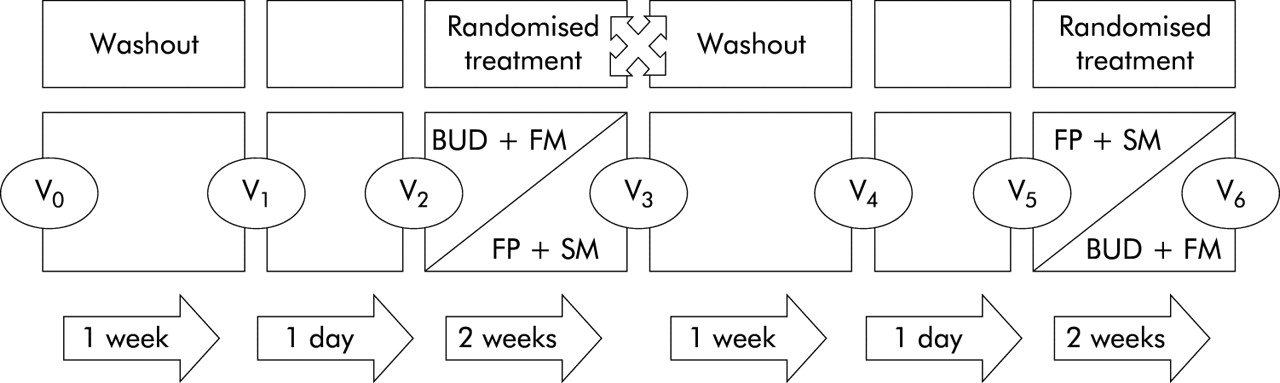
A scheme of the study design is shown in fig 1. The study was conducted in a randomised, double blind, double dummy, crossover, parallel group fashion. Patients were required to stop any second line controller treatment such as long acting β2 agonists (n = 9), leukotriene CysLT1 receptor antagonists (n = 1), and theophylline (n = 1) for a 1 week period before the initial screening visit and for the entire duration of the study. Short acting β2 agonists were withheld for the duration of the study, with ipratropium bromide 20 µg (Atrovent; Boehringer Ingelheim, Bracknell, UK) being given as reliever therapy instead. There was a 1 week washout period before each randomised treatment during which patients continued to receive their usual inhaled corticosteroid treatment. Patients were randomised to receive for 2 weeks an inhaled combination of either budesonide (BUD) 200 µg + FM 6 µg (Symbicort 200/6 Turbohaler; AstraZeneca, Luton, UK) two puffs twice daily or fluticasone propionate (FP) 250 µg + SM 50 µg (Seretide 250 Accuhaler; Allen and Hanburys, Uxbridge, UK) one puff twice daily. The dose of inhaled corticosteroid as FP in Seretide was chosen to be approximately equipotent to that of BUD in Symbicort, given that FP is twice as potent as BUD, while 50 µg SM is approximately equipotent to 12 µg FM. With each active Turbohaler patients also received a placebo Accuhaler and vice versa. All active and placebo Turbohaler and Accuhaler devices were masked to make them identical in external physical appearance.

Study design schematic. Methacholine challenges with salbutamol recovery were performed at V1 and V4 after each washout, before randomised treatments, and 1 hour after the first and last doses of each randomised treatment at V2, V3, V5 and V6.
Measurements
Spirometry
Spirometric tests were performed according to the American Thoracic Society criteria12 using a Micro Medical SuperSpiro (Micro Medical Ltd, Rochester, UK). At each of the study visits FEV1 was measured before and 1 hour after treatment.
Methacholine bronchial challenge
Methacholine challenge was performed following each washout period before each randomised treatment and 1 hour after the first and last doses of each treatment. Methacholine was administered using a standardised breath actuated dosimeter (Mefar; Markos-Mefar SpA, Bovezzo, Italy) at 5 minute intervals in doubling cumulative concentrations from 0.03125 mg/ml to 64.0 mg/ml until a 20% reduction in FEV1 was recorded. Log linear interpolation was performed using a computer assisted program (Micro Medical Ltd) to calculate the PC20 values.
Acute salbutamol recovery
Immediately after methacholine bronchial challenge patients received inhaled salbutamol 200 µg (Ventolin 200 Accuhaler; Allen and Hanburys, UK) and measurements of FEV1 were recorded at 5 minute intervals for 30 minutes.
Domiciliary PEF
Patients recorded morning domiciliary PEF using a Mini-Wright meter (Clement Clarke International Ltd, Harlow, UK) for the duration of the study. The values for the last 5 days following each washout and randomised treatment were used in the analysis.
Statistical analysis
The study was powered at 80% with the α error set at 0.05 (two tailed) and the β error set at 0.2, in order to detect a 50% difference in acute salbutamol recovery (the primary outcome variable) for within patient changes between the first and last doses of each treatment, calculated as the area under the 30 minute time-response curve for the percentage change from pre-challenge (1 hour after treatment inhalation) baseline FEV1. As a secondary outcome, the salbutamol response at 30 minutes was also evaluated, calculated as the percentage change from pre-challenge FEV1. Tolerance was defined as the difference in salbutamol recovery between the first and last doses of each treatment. An overall analysis of variance followed by multiple range testing with Bonferroni correction set at 95% confidence interval (CI) was performed and a p value of <0.05 (two tailed) was considered significant. Comparisons were made between genotypes and randomised treatments. To normalise distribution, data for methacholine PC20 were logarithmically transformed and analyses were performed using Statgraphics statistical software package (STSC Software Publishing Group, Rockville, USA).
RESULTS
Patients
The demographic details of the study patients are shown in table 1. The 10 patients from each homozygous genotype-16 group had similar sex distribution and comparable mean age, FEV1, and inhaled corticosteroid dose. One Gly-16 patient who had completed the FP + SM limb of the study had an exacerbation during the second washout period before BUD + FM and was withdrawn, although data for the patient were included on an intention to treat basis for completed visits.
Demographic characteristics of study patients
Washout values
Values following the washout periods were similar for pre-challenge FEV1, methacholine PC20, and salbutamol recovery for both genotypes and treatment groups (table 2).
Mean (SD) washout values before randomised treatments for pre-challenge FEV1 (% predicted), methacholine PC20 (mg/ml), and salbutamol recovery (%.min)
Methacholine challenge
The pre-challenge FEV1 values (1 hour after inhalation) for each genotype were not significantly different between the first and last doses of each treatment (table 3). There were also no significant differences in methacholine PC20 values for either genotype between the first and last doses of either treatment (table 3).
Mean (SE) values at first and last doses of treatments for pretreatment % predicted FEV1, % predicted FEV1 1 hour after treatment (pre-challenge), and methacholine PC20 (mg/ml)
Salbutamol recovery
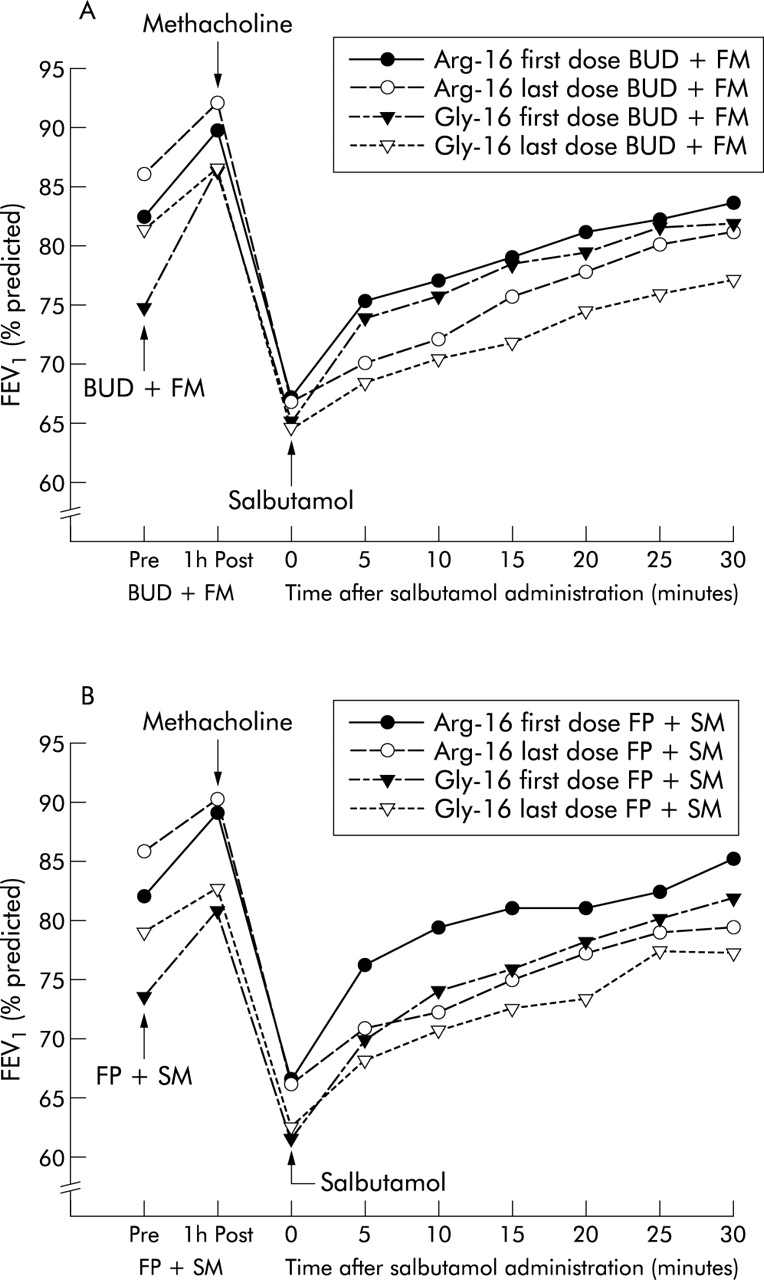
Following methacholine challenge the mean percentage fall in FEV1 from the pre-challenge value (1 hour after treatment) was not significantly different for either genotype or treatment group between the first and last doses of BUD + FM and FP + SM (table 4, fig 2). Salbutamol recovery as area under the 30 minute time-response curve (%.min) was significantly delayed in both genotype and treatment groups between the first and last doses of each treatment (p<0.05; table 4 and fig 3). The mean percentage fall in FEV1 from the pre-challenge value 30 minutes after administration of salbutamol was significantly greater in both genotype and treatment groups between the first and last doses of BUD + FM and FP + SM (p<0.05; table 4 and fig 4).
Mean (SE) % fall in FEV1 from pre-challenge value for first and last doses of randomised treatments after methacholine challenge before salbutamol, salbutamol recovery over 30 minutes (%.min), and % fall from pre-challenge value 30 minutes after salbutamol
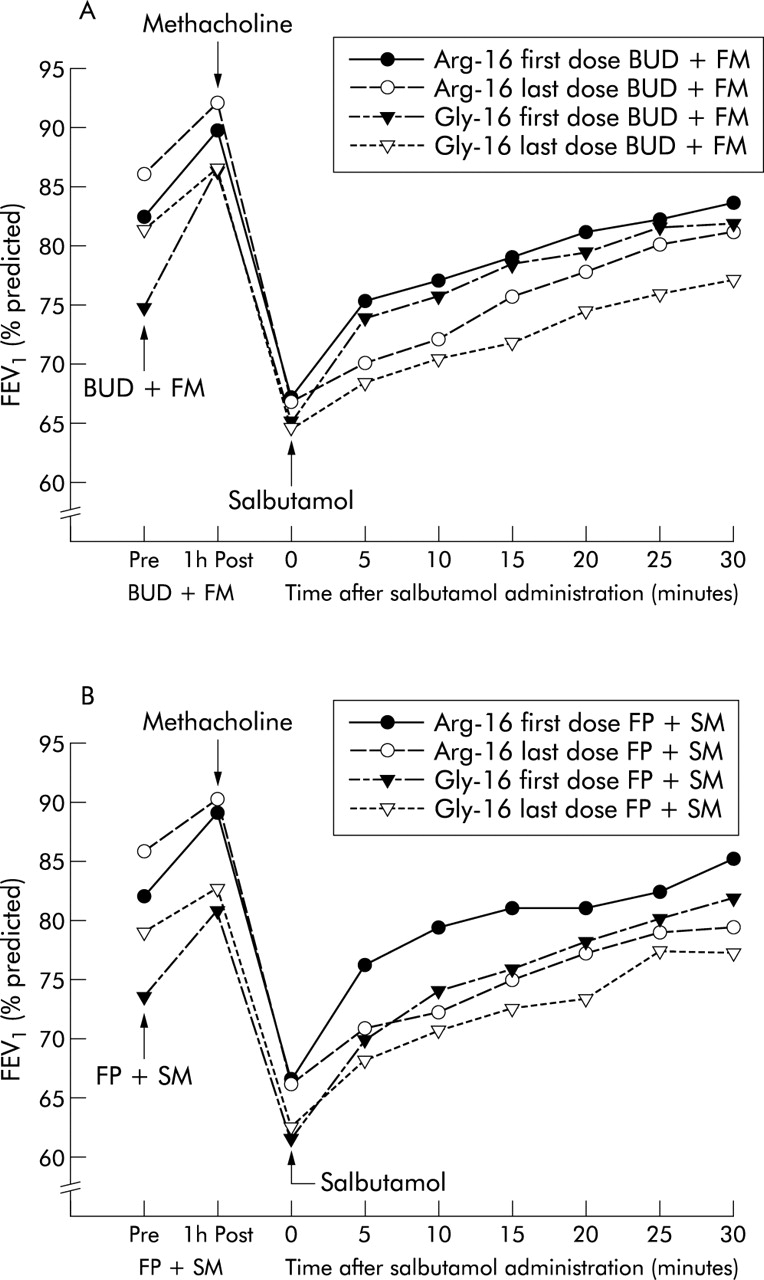
Mean FEV1 values (% predicted) before and 1 hour after first and last doses, methacholine challenge, and salbutamol recovery over 30 minutes for (A) BUD + FM and (B) FP + SM.

Salbutamol recovery after methacholine challenge as the area under the 30 minute time-response curve for the percentage change in baseline FEV1 (%.min) from the pre-challenge value (1 hour after treatment) for each genotype after the first and last doses of (A) BUD + FM and (B) FP + SM. A larger value for the area under the 30 minute time-response curve indicates a greater degree of delayed recovery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual data for percentage fall in FEV1 from the pre-challenge value (1 hour after treatment) 30 minutes after administration of salbutamol for (A) BUD + FM and (B) FP + SM. Data points for each individual are joined together, with mean values depicted as horizontal lines. Values are shown for each genotype after the first and last doses of each randomised treatment.
Pulmonary function
FEV1 values both before and 1 hour after treatment (pre-challenge) were not significantly different for either genotype or treatment group between the first and last doses of BUD + FM and FP + SM (table 3). Domiciliary morning PEF values (l/min) were not significantly different for Arg-16 v Gly-16 in both treatment groups (BUD + FM: mean (SE) washout values 452 (33) v 412 (20) (95% CI −48 to 128), randomised treatment values 479 (29) v 450 (14) (95% CI −41 to 100); FP + SM: washout values 465 (28) v 422 (15) (95% CI −25 to 111), randomised treatment values 482 (31) v 450 (23) (95% CI −50 to 115). PEF values were significantly higher (p<0.05) after treatment in both genotypes. The following PEF values were obtained when washout values were compared with randomised treatment values for BUD + FM (Arg-16: 452 (33) v 479 (29) (95% CI 8 to 47); Gly-16: 412 (20) v 450 (14) (95% CI 22 to 57)) and for FP + SM (Arg-16: 465 (28) v 482 (31) (95% CI 11 to 47); Gly-16: 422 (15) v 450 (23) (95% CI 10 to 45)).
DISCUSSION
Our results show that acute salbutamol recovery in constricted airways following methacholine challenge is significantly delayed to a similar degree in both Arg-16 and Gly-16 genotypes following treatment with either BUD + FM or FP + SM. The cross tolerance for the salbutamol response was evident in terms of the difference between the first and last doses of each combination inhaler.
The values for FEV1, methacholine PC20, and salbutamol recovery after washout for both genotypes were not significantly different before BUD + FM and FP + SM, indicating that there were no carryover effects between the randomised treatment limbs. Furthermore, the values for pre-challenge FEV1 (1 hour after inhalation) and post-challenge FEV1 (after methacholine) were also not significantly different for either genotype or treatment, suggesting that the altered salbutamol response could not be accounted for by alterations in airway calibre. Moreover, there were no differences in methacholine PC20 values for either genotype when the first and last doses of each randomised treatment were compared, suggesting that the delay in salbutamol recovery was independent of the dose of inhaled methacholine.
We observed a non-significant trend towards reduced protection—as indicated by a lower PC20 threshold value—after the last doses compared with the first doses of each randomised treatment with both genotypes, as seen in previous studies.13,14 We did not feel it was necessary to compare the first and last dose salbutamol recovery with that after each washout as the dose of methacholine was much higher after BUD + FM and FP + SM. The higher dose of methacholine after the first and last doses of each randomised treatment would thus have resulted in delayed recovery on its own, irrespective of any effects on β2 adrenoceptor function by the long acting β2 agonists.
Irrespective of genotype-16, salbutamol recovery exhibited cross tolerance in patients exposed to BUD + FM or FP + SM. Long acting β2 agonists have been shown to downregulate and uncouple β2 receptors leading to tolerance of response.15–17 Moreover, prolonged β2 receptor occupancy by long acting β2 agonists may result in attenuation of the salbutamol response, aside from tolerance.18,19 Similar negative interactions between long acting β2 agonists and salbutamol have been shown previously in genotype unselected patients in the presence of methacholine constricted airways.10,11,13,14
We expected to see differences in salbutamol recovery between the genotypes at position 16 on the basis of previous in vitro data which have suggested development of enhanced downregulation of β2 adrenoceptors and tolerance in the homozygous Gly-16 genotype.1,2 Our data would therefore question the clinical relevance of β2 adrenoceptor genotype-16 in determining the potential for interaction between short and long acting β2 agonists. Nevertheless, we recognise that, in retrospect, we should have performed two separate power calculations for differences between treatments and for differences between genotypes, and as such our study may have had low power to detect the latter. We also acknowledge that comparisons between the first and last doses of treatment were uncontrolled in the strictest statistical sense as there were no study limbs evaluating before and after placebo effects.
We elected to use the methacholine challenge model as this produces a high degree of functional antagonism in terms of uncovering a subtle degree of salbutamol cross tolerance induced by prior exposure to long acting β2 agonists.20 Previous data suggesting adverse effects on PEF and asthma exacerbations were associated with regular salbutamol in patients with the Arg-16 genotype,6,7 which may reflect rebound end of dose effects rather than tolerance between the first and last dose per se. It would be interesting to evaluate retrospectively genotyped data on asthma exacerbations from large multicentre trials where long acting β2 agonists conferred improvements,21 as no such analysis has been performed.
There are some retrospective data which suggest that complex β2 adrenoceptor haplotypes may influence the acute bronchodilator response to salbutamol.22 However, as many of these haplotypes are relatively uncommon, one can always question their clinical relevance. We selected our patients according to homozygous genotypes at position 16, irrespective of the genotype at position 27. Data for isoproterenol induced venodilatation in the dorsal hand vein are available which show enhanced tolerance of the response in association with the haplotype comprising homozygous Arg-16 in combination with homozygous glutamic acid (Gln-27) compared with the haplotype combination of homozygous Gly-16 with either homozygous Gln-27 or homozygous glutamine (Glu-27).23 None of our patients had the haplotype combination of homozygous Gly-16 and homozygous Gln-27, which is uncommon due to linkage disequilibrium between homozygous genotypes at position 16 and 27.24 For this reason, our small genotype selected sample was inadequate for the purposes of making any meaningful haplotype comparisons.
There were no differences in the effects of BUD + FM and FP + SM on acute salbutamol recovery, even though there are differences in the β2 adrenoceptor intrinsic activity between FM and SM.25 The present findings are in keeping with previous data showing no difference between both long acting β2 agonists in bronchoprotection as add-on therapy to inhaled corticosteroids in Gly-16 selected patients,26 or in downregulation of peripheral blood lymphocyte β2 adrenoceptors.27 One might have expected to see greater cross tolerance of the salbutamol response with a full β2 agonist such as FM, perhaps due to enhanced uncoupling of the β2 adrenoceptor adenylate cyclase subunit. Indeed, the present data are also in keeping with our previous results which showed a similar degree of cross tolerance to salbutamol recovery between BUD + FM or FP + SM compared with BUD or FP alone.10
We conclude that cross tolerance to the acute salbutamol response occurs in methacholine constricted airways following treatment with FM or SM combination inhalers, irrespective of genotype-16.
REFERENCES
Footnotes
-
This study received no support from the pharmaceutical industry and was funded from a departmental research grant from the University of Dundee.