Article Text

Abstract
Background: Neutrophils are thought to play an important role in the pathogenesis of idiopathic pulmonary fibrosis (IPF). Human neutrophils contain antimicrobial and cytotoxic peptides in the azurophil granules which belong to a family of mammalian neutrophil peptides named α-defensins. A study was undertaken to investigate the role of α-defensins in the pathogenesis of IPF.
Methods: The concentrations of α-defensins (human neutrophil peptides (HNPs) 1, 2, and 3) in plasma and bronchoalveolar lavage (BAL) fluid of 30 patients with IPF and 15 healthy subjects were measured by radioimmunoassay.
Results: The concentrations of α-defensins in plasma, but not in BAL fluid, were significantly higher in IPF patients than in controls. BAL fluid concentrations of interleukin (IL)-8 in patients with IPF, which were significantly higher than in controls, correlated with those of α-defensins. An inverse relationship was seen between plasma α-defensin levels and the arterial oxygen tension (Pao2) and pulmonary function (vital capacity (%VC), forced expiratory volume in 1 second (FEV1), and carbon monoxide transfer factor (%Tlco)) in patients with IPF. Plasma levels of α-defensins also correlated with the clinical course in IPF patients with an acute exacerbation. Immunohistochemically, positive staining was observed inside and outside neutrophils in the alveolar septa, especially in dense fibrotic areas.
Conclusion: These findings suggest that α-defensins play an important role in the pathogenesis of IPF, and that the plasma α-defensin level may be a useful marker of disease severity and activity.
- idiopathic pulmonary fibrosis
- α-defensins
- surfactants
- interleukin 8
Statistics from Altmetric.com
Idiopathic pulmonary fibrosis (IPF), a chronic progressive disorder of the lung parenchyma, is characterised by both inflammation and fibrosis.1 Increasing evidence points to the importance of neutrophils, in addition to eosinophils and alveolar macrophages, in the pathogenesis of pulmonary fibrosis, and increased numbers of neutrophils occur in the bronchoalveolar lavage (BAL) fluid and lung tissue of patients with IPF.2–8 However, it has also been reported that the number and proportion of neutrophils in BAL fluid do not correlate with the activity of neutrophil alveolitis and that they have limited prognostic value,4,9,10 so the prognostic value of the neutrophil count in BAL fluid and the exact role of neutrophils in the pathogenesis of IPF remain controversial. Obayashi and colleagues7 recently reported the presence of high levels of neutrophil elastase in lung parenchyma, BAL fluid and serum of patients with IPF, but no increase in neutrophil count in BAL fluid. Yamanouchi et al11 also reported high levels of the neutrophil elastase:α1-proteinase inhibitor complex (E-PI) in the serum of patients with IPF, and found that serum and BAL fluid levels of E-PI were correlated with some clinical parameters. The involvement of matrix metalloproteinase-9 derived from activated neutrophils in the pathogenesis of IPF has also been reported.12 These findings suggest that neutrophils may indeed play an important role in the pathogenesis of IPF.
α-Defensins are cationic proteins with antimicrobial activity against Gram positive and Gram negative bacteria, fungi, and enveloped viruses.13,14 Six α-defensins have so far been recognised in humans—four exclusive to neutrophils (human neutrophil peptides (HNPs) 1–4) and two others in Paneth cells in the small intestine.13,14 Because HNP-1, HNP-2, and HNP-3 constitute 5–7% of the total protein content of the human neutrophil and 30–50% of the total protein content of the azurophilic granules, it is thought that they are the most abundant antimicrobial proteins present in the neutrophil. In contrast, HNP-4, which has only 32% amino acid sequence homology with other HNPs, shows anti-corticotrophin activity and is less antimicrobial than HNPs 1–3.13,14 Increased concentrations of α-defensins in the plasma and body fluids of patients with various infections have previously been reported by us and by other workers.15,16 Moreover, through their cytotoxic effects on human lung cells,17,18 α-defensins are thought to be related to various neutrophil related lung diseases such as cystic fibrosis, diffuse panbronchiolitis (DPB), and mycobacterial infection.18–20
In this study we have measured the concentrations of α-defensins (HNPs 1–3) in plasma and BAL fluid of patients with IPF to clarify their role in the pathogenesis of this disease.
METHODS
Study population
The study population consisted of 30 patients with IPF (24 men) of mean (SD) age 61 (8) years and included seven smokers, eight ex-smokers, and 15 who had never smoked. The diagnosis of IPF was based on standard criteria1 which included clinical findings (exertional dyspnoea, non-productive cough, fine crackles on auscultation of the lung bases), pulmonary function tests (restrictive pattern), and chest radiographic and high resolution CT findings (bilateral diffuse parenchymal abnormalities consistent with the diagnosis of IPF). A transbronchial lung biopsy and BAL were performed in all patients for whom IPF was a possible diagnosis to rule out other diseases. A diagnosis of IPF was confirmed by surgical lung biopsy in 22 of the 30 patients. None of the patients included in this study had a history of environmental or occupational exposure, clinical findings of hypersensitivity pneumonitis, connective tissue disease, or evidence of granulomas or vasculitis. In all patients current infection caused by bacteria, mycobacteria, or fungi was excluded by negative cultures of BAL fluid. We also included three IPF patients with an acute exacerbation for examination of the time course of plasma α-defensin concentrations.
Fifteen age and sex matched healthy volunteers were included as controls. All normal volunteers had normal chest radiographs, were free of symptoms, and were not taking any medication.
Bronchoalveolar lavage
With informed consent, BAL was performed as described previously21 using a flexible fibreoptic bronchoscope (Olympus, P-20 Olympus, Tokyo, Japan). Briefly, the bronchoscope was wedged into one of the segmental or subsegmental bronchi of the right middle lobe and 50 ml sterilised saline at body temperature was then instilled through the bronchoscope. The fluid was immediately retrieved by gentle suction using a sterile syringe and the procedure was repeated three times. BAL fluid was passed through two sheets of gauze and then centrifuged at 500g for 10 minutes at 4°C. After washing twice with phosphate buffered saline (PBS) free of calcium and magnesium (PBS, Gibco, UK), the remaining cells were suspended in PBS supplemented with 10% heat inactivated fetal calf serum and counted using a haemocytometer. An aliquot was then diluted to a concentration of 2 ×105 cells/ml and a 0.2 ml cell suspension was spun down onto a glass slide at 1100 rpm for 2 minutes using a Cytospin 2 cytocentrifuge (Shandon Instruments, Sewickley, PA, USA). The remaining fluid was centrifuged at 500g for 5 minutes and the supernatant was stored at –80°C until examined. The slides were dried, fixed, and then stained by the May-Giemsa method. More than 200 cells were identified using a photomicroscope.
Measurement of α-defensin, KL-6, SP-A, and SP-D levels
The concentrations of α-defensins in plasma and BAL fluid samples were measured by radioimmunoassay (RIA) established by our laboratory.22 Full length HNP-1 was synthesised using a peptide synthesiser Model 430 (Applied Biosystems, Foster City, CA, USA) and purified by reverse phase high performance liquid chromatography (RP-HPLC). In RP-HPLC, synthetic HNP-1 was eluted at a position identical to that of native HNP-1 isolated from human leucocytes. Synthetic HNP-1 was used for immunising New Zealand white rabbits by multiple intracutaneous and subcutaneous injections. It was radioiodinated and the 125I-labelled peptide was purified by RP-HPLC on a TSK ODS 120A column (Tosoh Co, Tokyo, Japan). A diluted sample or standard peptide solution (100 μl) was incubated for 24 hours with 100 μl antiserum diluent (final dilution 1/21 000). The 125I-labelled HNP-1 solution (16 000 cpm in 100 μl) was added and the mixture was incubated again for another 24 hours. Normal rabbit serum and anti-rabbit IgG goat serum were then added and stored for 16 hours. Bound and free ligands were separated by centrifugation. All procedures were performed at 4°C and duplicate assays were carried out. Volumes of 0.5 μl plasma and 1–10 ml BAL fluid were used to determine the levels of α-defensins. The antiserum recognised HNP-1, HNP-2, and HNP-3 equally on a molar basis, so the RIA data were expressed as the sum of HNPs 1–3 and their precursor proteins, the presence of which was confirmed by simultaneous measurements using RP-HPLC and RIA.23 The intra-assay and inter-assay coefficients of variation were 3.5% and 8% at 50% binding, respectively, in this RIA.
Serum samples were used to measure pulmonary surfactant protein (SP)-A,24 SP-D,24 and KL-625 which are known markers of disease activity in interstitial lung diseases. SP-A (the Teijin Institute of Bio-medicine, Tokyo, Japan), SP-D (SP-D kit Yamasa, Yamasa Shoyu Co, Tokyo, Japan), and KL-6 (ED 406, Eisai, Tokyo, Japan) assays were performed using commercially available ELISA kits. The concentration of interleukin (IL)-8 was also measured with a commercially available kit (Toray Fuji Bionics, Tokyo, Japan).
Immunohistochemistry of lung tissues
Immunohistochemical analysis of α-defensins in the lungs of patients with IPF was performed as described previously.19,26 Surgical lung biopsy specimens were obtained from six IPF patients. As a control, normal lung tissue specimens resected at surgery from a 45 year old man with tuberculosis were also studied. The tissue samples were immersed in Zamboni's fixative (2% paraformaldehyde and 0.25% picric acid in 0.1 M PBS adjusted to pH 7.4) or in 10% formaldehyde in PBS and, after dehydration in serial ethanol concentrations, they were embedded in paraffin. The specimens (3 mm thick) were deparaffinised in xylene, rehydrated in serial ethanol solutions, and treated with 0.3% hydrogen peroxide for 30 minutes to inactivate any endogenous peroxidase. Non-specific binding was blocked with normal goat serum. Anti-HNP 1–3 antiserum at a final dilution of 1/10 000 was allowed to react overnight with each preparation at 4°C in a moist chamber. Goat biotinylated anti-rabbit IgG was used as the second antibody. The samples were stained by the ABC alkaline phosphatase (ABC-AP) method using an ABC-AP kit (Dako Co, Carpinteria, CA, USA) and the tissue samples were counterstained with haematoxylin.
Statistical analysis
Data were expressed as mean (SD) values. Differences between groups were examined using the Mann-Whitney U test. Correlations between two groups were determined using the Spearman's rank correlation analysis. A p value of <0.05 was considered to be statistically significant.
RESULTS
BAL fluid findings and α-defensin levels
The total number of cells recovered in the BAL fluid was significantly higher in patients with IPF than in controls (table 1). In patients with IPF the percentage of alveolar macrophages was lower and the number and percentage of neutrophils were significantly higher than in controls (table 1). There were no significant correlations between the number and percentage of neutrophils in BAL fluid and various clinical parameters including arterial oxygen tension (Pao2) and pulmonary function tests. As shown in fig 1, the mean plasma concentration of α-defensins was higher in patients with IPF (768.2 (422.4) ng/ml) than in controls (323.3 (173.1) ng/ml, p<0.01), but there was no significant difference between the two groups in the concentration of α-defensins in the BAL fluid (IPF: 52.0 (92.0) ng/ml; control: 12.9 (15) ng/ml).
Mean (SD) BAL fluid cells in control subjects and patients with idiopathic pulmonary fibrosis (IPF)

Concentrations of α-defensins in (A) plasma and (B) bronchoalveolar lavage (BAL) fluid of patients with idiopathic pulmonary fibrosis (IPF) and controls.
There was no significant correlation between plasma and BAL fluid concentrations of α-defensins in patients with IPF, but the number (r=0.395, p=0.034) and percentage (r=0.436, p=0.019) of neutrophils correlated with the concentrations of α-defensins in the BAL fluid of IPF patients. Plasma concentrations but not BAL fluid concentrations of α-defensins correlated negatively with Pao2, %VC, FEV1, and %Tlco in patients with IPF (fig 2 and table 2). A correlation analysis of the levels of KL-6, SP-A, and SP-D (which are known markers of disease activity in interstitial lung diseases) with these clinical parameters revealed only significant correlations between SP-A and %VC or %Tlco (table 2). Plasma α-defensin concentrations in patients with IPF did not correlate with the serum concentrations of KL-6 (r=–0.223, p=0.346), SP-A (r=–0.273, p=0.26), or SP-D (r=–0.297, p=0.236).
Correlation analysis between levels of α-defensins, KL-6, SP-A, and SP-D and pulmonary function tests
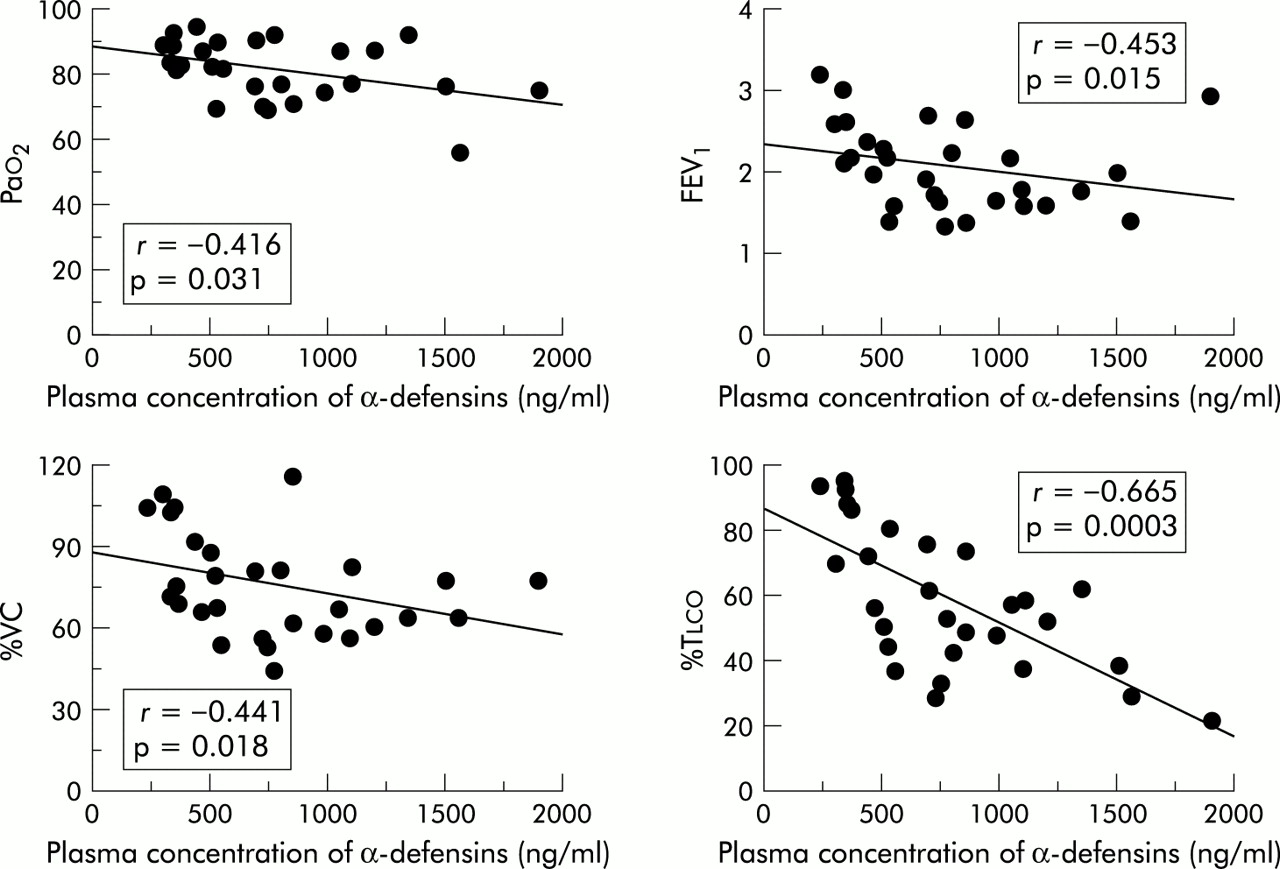
Correlation between plasma concentrations of α-defensins and Pao2, FEV1, %VC, and %Tlco.
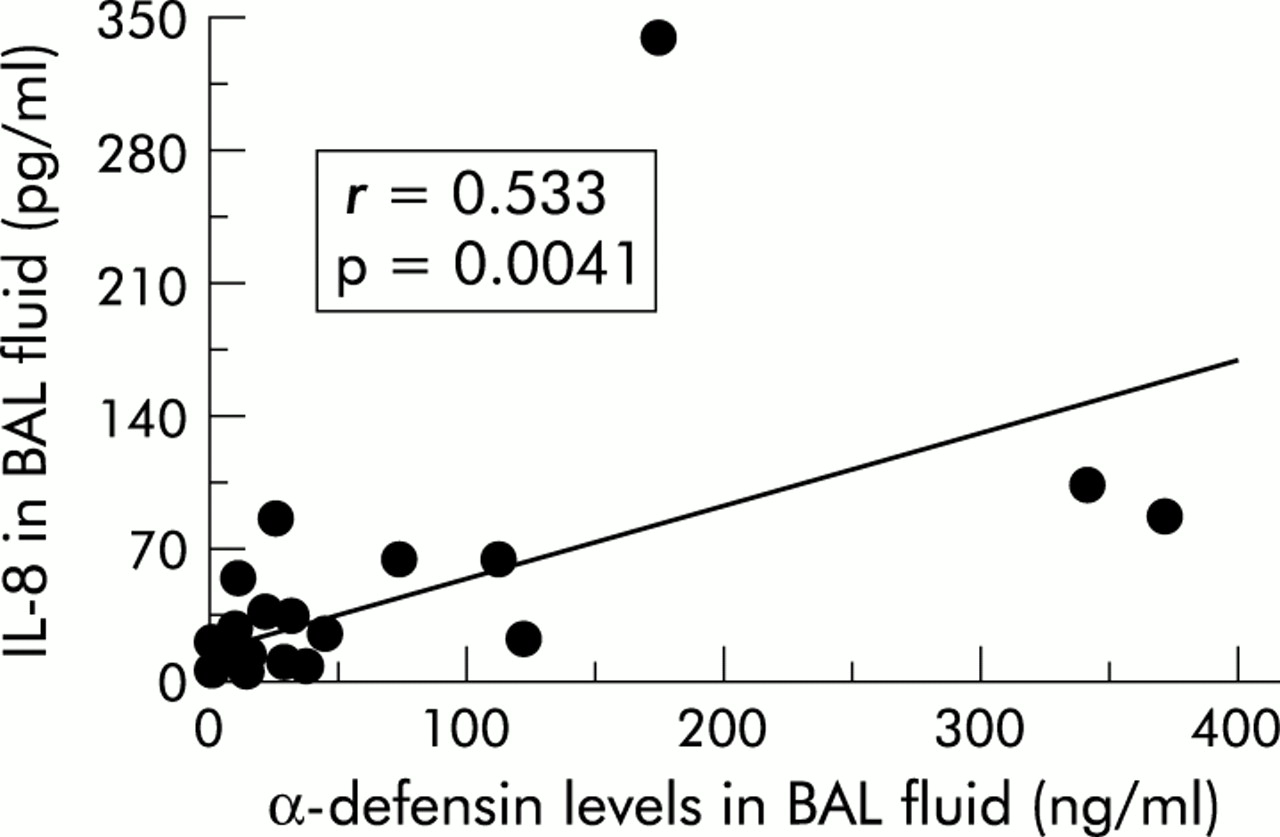
As shown in fig 3, concentrations of IL-8 in both BAL fluid (37.2 (64.2) pg/ml) and serum (27.5 (69.8) pg/ml) in patients with IPF were significantly higher than in control subjects (5.9 (5.7) pg/ml in BAL fluid; 0.9 (2.4) pg/ml in serum). Although no significant correlation was observed between the BAL fluid concentration of IL-8 and the plasma concentration of α-defensins, there was a positive correlation between α-defensins and IL-8 in BAL fluid (r=0.533, p=0.0041, fig 4). A significant correlation was also observed between IL-8 levels and the number (r=0.424, p=0.0217) and percentage (r=0.491, p=0.0079) of neutrophils in the BAL fluid of patients with IPF.
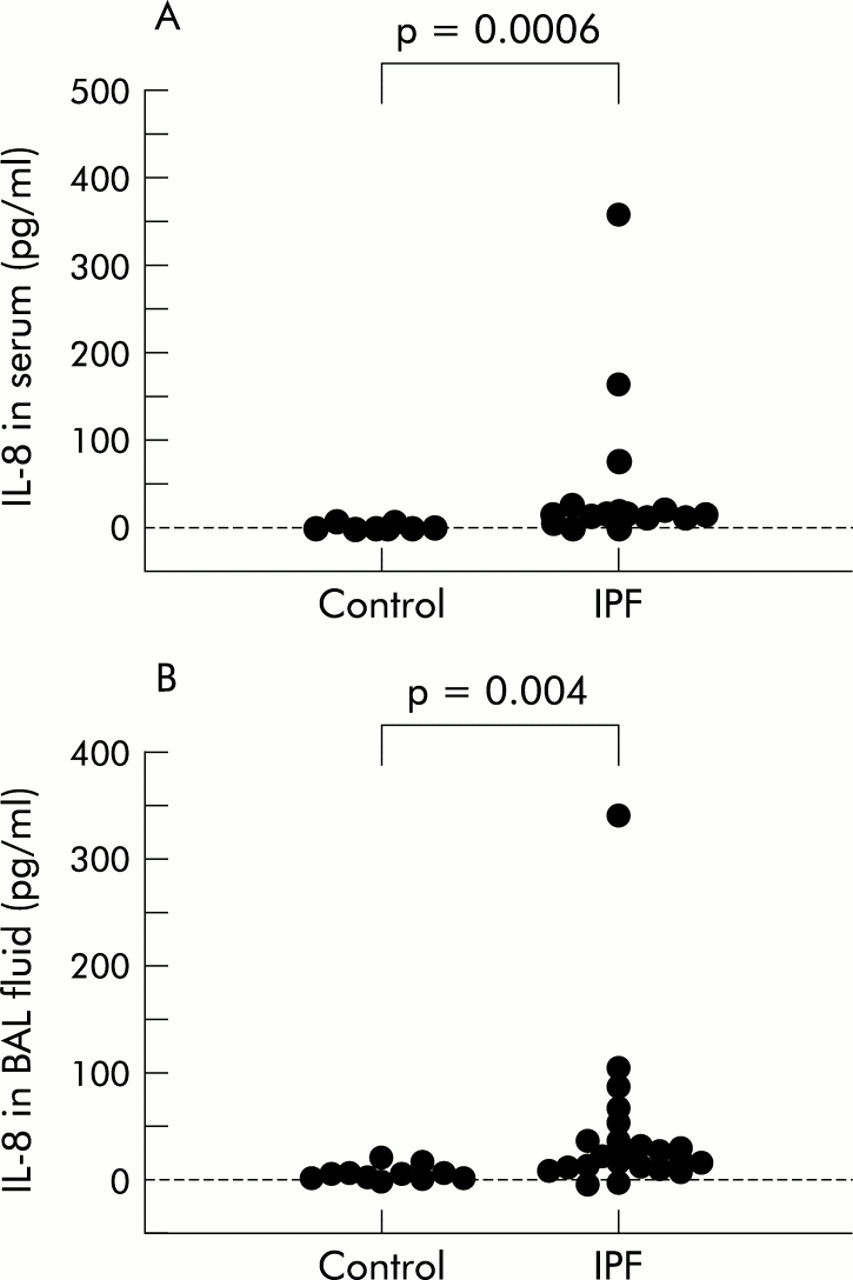
Concentrations of interleukin (IL)-8 in (A) serum and (B) bronchoalveolar lavage (BAL) fluid of patients with idiopathic pulmonary fibrosis (IPF) and controls.

Correlation between α-defensins and interleukin (IL)-8 levels in bronchoalveolar lavage (BAL) fluid of patients with idiopathic pulmonary fibrosis (IPF).
The clinical course and serial changes in plasma concentrations of α-defensins in two representative IPF patients with acute exacerbations are depicted in fig 5. In one patient an acute exacerbation was associated with a rise in the plasma concentration of α-defensins while clinical improvement and resolution of chest radiographic findings induced by steroid and cyclophosphamide treatment were associated with a fall in the plasma α-defensin concentration (fig 5A). Two patients with IPF died of respiratory failure due to an acute exacerbation with a concomitant increase in plasma concentrations of α-defensins. The clinical and laboratory data of one of these two patients are shown in fig 5B.

Summary of clinical course and serial changes in plasma concentrations of α-defensins in two representative patients with IPF. (A) A patient who exhibited progressive dyspnoea associated with high plasma concentrations of α-defensins. Steroid treatment resulted in an improvement in symptoms and chest radiographic findings with a corresponding decrease in plasma concentrations of α-defensins. (B) A patient who died from respiratory failure due to an acute exacerbation with a concomitant rise in plasma concentrations of α-defensins.
Immunostaining of α-defensins
Immunohistochemical studies in six patients with IPF using anti-HNPs 1–3 antiserum showed the presence of α-defensins both inside and outside neutrophils in the interstitium, especially in dense fibrotic tissues (fig 6A,B). Some neutrophils were also observed in the alveolar space. In addition, neutrophil adhesion occurred along the endothelium in pulmonary microvessels in patients with IPF (fig 6C). In control lung tissue only neutrophils were stained with anti-HNPs 1–3 antiserum (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical staining of IPF lung specimens using anti-human neutrophil peptides (HNPs) 1–3 antiserum. Note the presence of α-defensins inside and outside the neutrophils in the alveolar septa, especially in dense fibrotic areas (A: original magnification ×10; B: ×50). Neutrophil adhesion was also observed along the endothelium in pulmonary microvessels in patients with IPF (C: original magnification ×25).
DISCUSSION
We have evaluated the role of neutrophils in patients with IPF through its granule protein, α-defensins. The major finding was that patients with IPF had significantly increased concentrations of α-defensins in plasma but not in BAL fluid. In addition, the plasma levels of α-defensins correlated inversely with several clinical parameters including Pao2 and pulmonary function tests (%VC, FEV1, and %Tlco) in patients with IPF. Immunohistochemical studies also demonstrated the accumulation of a considerable number of neutrophils in lung parenchyma biopsy specimens.
Increased numbers of neutrophils in BAL fluid and lung tissue have been reported in patients with IPF.2–8 However, the neutrophil count in the BAL fluid has not been shown to have a prognostic value.9,10 We found no correlation between the number of neutrophils and the BAL fluid concentration of α-defensins or clinical parameters, although there was a significantly higher number of neutrophils in the BAL fluid of patients with IPF. Obayashi and colleagues7 found increased numbers of infiltrating neutrophils in the lung parenchyma of IPF patients using immunohistochemistry for neutrophil elastase, but no increase in neutrophil count in the BAL fluid. These findings suggest that the BAL procedure does not sample the underlying interstitial process accurately in patients with IPF. Our study showed an inverse relationship between plasma concentrations of α-defensins and Pao2, %VC, FEV1, and %Tlco in patients with IPF. In this context, Yamanouchi et al11 found increased serum levels of E-PI, another neutrophil granule protein, in patients with IPF, and a positive correlation between serum and BAL fluid levels of E-PI and some clinical parameters including Pao2. The present immunohistochemical studies (for α-defensins) and those of other laboratories7 (for neutrophil elastase) showed that positive staining was observed both inside and outside neutrophils in the alveolar septa, especially in dense fibrotic areas. These findings suggest the involvement of neutrophils through their cytotoxic granules in the pathogenesis of pulmonary fibrosis. This is supported by a previous report which showed that administration of neutrophil elastase inhibitor attenuated the severity of bleomycin induced lung injury and of subsequent pulmonary fibrosis.27 The plasma concentration of α-defensins, as well as neutrophil elastase, may therefore be a useful marker of disease severity in IPF. In addition, our finding that plasma concentrations of α-defensins reflect the clinical course in patients with an acute exacerbation suggests that the plasma concentration of α-defensins is also a useful marker of disease activity.
Using immunohistochemistry, we also found the expression of α-defensins in neutrophils attached to the capillary endothelium (fig 5C). This finding is similar to that reported by Obayashi et al7 and suggests that activation of neutrophils at the site of the endothelium of pulmonary microvessels may take place in patients with IPF. Westlin and colleagues28 have shown the direct cytotoxic effect of neutrophils on human vascular endothelium, and α-defensins also have a direct cytotoxic effect on human endothelial cells.17 “Neutrophilic endothelitis” as part of “neutrophilic alveolitis” could therefore be an important pathogenic feature of IPF.29
Our finding of a positive correlation between IL-8 and α-defensin levels in the BAL fluid of patients with IPF fits well with previous reports of the relationship between IL-8 and α-defensins in various types of pulmonary infectious diseases. IL-8 is a potent neutrophil attractant that can induce the release of α-defensins from neutrophils,19,30 which subsequently stimulate IL-8 synthesis by airway epithelial cells.31 The relationship between IL-8 and IPF is now well known, and alveolar macrophages located predominantly within the airspaces are the major source of IL-8 in IPF.32,33 Thus, IL-8 may be a key cytokine in the accumulation of neutrophils and the high concentration of α-defensins in BAL fluid in this disease. However, the concentrations of both IL-8 and α-defensin in the BAL fluid of patients with IPF were lower than in patients with DPB (α-defensins: 429 ng/ml, IL-8: 324 pg/ml)19 and Mycobacterium avium-intracellulare infection (α-defensins: 680 ng/ml, IL-8: 568 pg/ml).20 This finding may merely reflect the smaller number of neutrophils in the BAL fluid of patients with IPF (0.2 (0.3) × 105/ml) compared with DPB (9.8 (2.4) × 105/ml)19 and M avium-intracellulare infection (3.5 (1.8) × 105/ml).20
We have previously shown34 that BAL fluid levels of granulocyte colony-stimulating factor (G-CSF) in patients with IPF, which were higher than in other lung diseases, correlated with the BAL fluid neutrophil count, and that in BAL fluid samples from patients with IPF the mean value of neutrophil chemotactic activity was reduced by 35% after neutralisation with anti-human G-CSF antiserum. Administration of recombinant human G-CSF in patients with lung cancer enhances α-defensin biosynthesis in neutrophils.35 Thus, G-CSF might also be involved in neutrophil alveolitis and high plasma concentrations of α-defensins in patients with IPF as well as IL-8.
SP-A, SP-D, and KL-6 are useful biomarkers of interstitial lung diseases.24,25 SP-A and SP-D belong to the collectin subgroup of the C-type lectin superfamily. They are produced by two types of epithelial cells in the peripheral airway—Clara cells and alveolar type II cells—and their levels can predict IPF disease activity.24 The serum level of KL-6, MUC1 mucin, derived from damaged or regenerating type II pneumocytes in IPF is also useful for the diagnosis and evaluation of the activity of the disease.25 In our study we could not find any correlation between plasma concentrations of α-defensins and serum concentrations of SP-A, SP-D, or KL-6, probably because of differences in the origin of these markers. In addition, the plasma level of α-defensins was the most useful marker for evaluating disease severity in this study (table 2). Although the plasma concentration of α-defensins is not necessarily a useful marker for the clinical diagnosis of IPF as raised levels are also seen in other lung diseases,15,19,20 it is a distinct new marker for disease severity and activity in IPF.
In conclusion, we have shown that plasma concentrations of α-defensins were raised in patients with IPF. Our findings suggest that neutrophil related pulmonary dysfunction may be mediated through α-defensins in IPF, and that these peptides could serve as new parameters of disease severity and activity.
Acknowledgments
The authors thank S Yokoyama and S Tajiri for their technical assistance. This study was supported in part by a research grant from the Ministry of Education, Science, Sports, and Culture of Japan.