Article Text

Abstract
Background: A study was undertaken to examine the expiratory flow response to a negative pressure (NEP) applied at the airway in patients with no abnormalities of the intrathoracic airway but suffering from the obstructive sleep apnoea syndrome (OSAS).
Methods: Nineteen patients with OSAS with normal spirometric values were studied. NEP of –5 cm H2O and –10 cm H2O was applied to the mouth when sitting and when supine.
Results: Thirteen patients exhibited expiratory flow limitation when supine (group 1). Of these, three also had flow limitation in the sitting position. The remaining six patients (group 2) had no flow limitation. Patients in groups 1 and 2 were similar with respect to age, sex, and body mass index, but the apnoea/hypopnoea index (AHI) was higher in group 1 than in group 2 (p<0.05). There was a significant correlation between the degree of flow limitation (expressed as a percentage of the expired tidal volume over which the NEP induced flow did not exceed spontaneous flow) and the AHI (p<0.05 for both pressure levels) as well as the desaturation index (DI, number of desaturations per hour of sleep; p<0.05 at –10 cm H2O).
Conclusion: This study confirms that the NEP technique can detect expiratory flow limitation of extrathoracic as well as of intrathoracic origin. This technique could be useful for studying the collapsibility of the passive upper airway in awake subjects and might help to predict the severity of OSAS.
- obstructive sleep apnoea syndrome
- negative expiratory pressure
- expiratory flow limitation
Statistics from Altmetric.com
The detection of expiratory flow limitation, defined as a lack of difference between tidal and forced expiratory flow, is relevant to the pathophysiological understanding of various clinical situations, including chronic obstructive pulmonary disease (COPD)1 and cardiac failure related airway obstruction.2 The advent of the negative expiratory pressure (NEP) technique has dramatically simplified the detection of expiratory flow limitation by obviating the need to resort to body plethysmography.3 The technique involves application of a negative pressure at the airway opening during tidal expiration. The ensuing flow-volume curve is then compared with that of the previous control expiration.4,5 Its non-volitional nature is a major advantage over methods based on forced expiratory manoeuvres. In addition, the technique detects flow limitation under the prevailing breathing conditions, thus providing clinically relevant information.
However, studying the expiratory flow in response to a negative pressure applied at the airway opening (as opposed to the expiratory flow in response to a positive alveolar pressure) has one major drawback—namely, except in tracheostomised or intubated patients, it can result in the collapse of the extrathoracic airway. In such a situation flow limitation will occur but will have a radically different meaning. Patients with the obstructive sleep apnoea syndrome (OSAS) are highly likely to exhibit such behaviour. Liistro et al6 showed that expiratory flow limitation is common in a population of patients with OSAS with no airway obstruction. Once this problem is known and understood, advantage can be taken of it. In the absence of any underlying lung disease likely to promote intrathoracic flow limitation, the NEP technique could be used to study the flow dynamics of the passive upper airway during wakefulness and thus could possibly help to refine the diagnosis strategy of OSAS. It could be postulated that, in the absence of intrathoracic airway obstruction as detected by pulmonary function tests, the presence of flow limitation could indicate upper airway abnormalities and the degree of flow limitation could correlate with their severity. The data provided by Liistro et al,6 who found a statistically significant relationship between the degree of flow limitation and the number of desaturations per hour of sleep, indirectly support this hypothesis.
The present study was undertaken to assess the effects of NEP applied at the mouth in awake patients suffering from OSAS, and to relate the results to the apnoea/hypopnoea index (AHI).
METHODS
Patients
Nineteen patients with clinical features of OSAS were included in the study. The diagnosis had previously been confirmed by a polysomnographic sleep recording study. The anthropometric characteristics of the patients and the results of the sleep studies are reported in table 1. The study was approved by the appropriate regulatory authority and the patients gave informed consent to participate.
Anthropometric characteristics, lung function, and polygraphic data
Measurements
All the measurements were obtained during the same visit to the laboratory in awake patients.
Sleep recording
The polysomnographic recordings (CID102p Device, Cidelec, Saintes Gemmes-sur-Loire, France) consisted of in-laboratory continuous acquisition transcutaneous oxyhaemoglobin saturation (Spo2), chest wall and abdominal movements, and tracheal sounds. From these data, apnoeic and hypopnoeic events and desaturation episodes were characterised according to standard criteria. In addition to the usual sleep parameters, the apnoea index (AI) and the apnoea/hypopnoea index (AHI) were calculated and the desaturation index (DI) was measured as the sleep time spent with a Spo2 below 90%.
Spirometric tests
Maximal flow-volume curves were obtained in the seated position. Vital capacity (VC) and forced expiratory volume in 1 second (FEV1) were measured using a Fleish no 2 pneumotachograph (Spirometer Micro 5000; Medisoft, Dinan, Belgium) and FEV1/VC was calculated. Maximal expiratory flow and flow at 25%, 50%, and 75% of VC were also measured. In 12 patients the functional residual capacity (FRC) and total lung capacity (TLC) were measured using a body plethysmograph (Jaeger, Witzburg, Germany). Quality criteria and reference values were those of the European Community.7
Expiratory flow limitation
An NEP of –5 cm H2O and –10 cm H2O was applied at the mouth during tidal breathing using a specially devised system (Medisoft, Dinan, Belgium). The patients breathed through a standard rubber mouthpiece connected to a low dead space (45 ml) low resistance circuit while wearing a nose clip. Three reproducible tracings were recorded for each patient, both in the seated and the supine posture, and averaged to calculate the degree of flow limitation (see below).
Data analysis
Flow limitation was deemed to be present when the NEP induced expiratory flow did not exceed the corresponding spontaneous expiratory flow, whether present throughout expiration or during any part of it. The presence or absence of flow limitation was used as a dichotomous variable for the statistical analysis. When present, the degree of flow limitation was expressed as the percentage of tidal expiration over which NEP did not induce any appreciable change in flow with respect to the control expired tidal volume (%Vt).5 The value of this index was, by definition, zero when flow limitation was absent.
Statistical analysis
The patients with flow limitation (group 1) were compared with those without flow limitation (group 2) using a one way analysis of variance (ANOVA). Differences between the degree of flow limitation (%Vt) between the two levels of NEP studied were assessed using the Wilcoxon non-parametric test. The association between the degree of flow limitation and variables derived from the sleep studies was studied using correlation analysis. Statistics were calculated using Statview and SuperAnova software (Abacus Concept, Berkeley, CA, USA) on an Apple Macintosh computer. Results were considered significant when the p value of a type I error was 0.05 or less. Data are provided as mean (SD) values.
RESULTS
All patients had normal forced expiratory flow/volume loops except one (patient no 8) who had a moderate obstructive ventilatory defect (FEV1 = 79% predicted, FEV1/VC = 79% predicted). Four patients had a decreased FRC (≤80% predicted) which was associated in two cases with a decreased TLC.
In the supine position 13 of the 19 patients exhibited expiratory flow limitation with both levels of NEP (group 1; table 2). Only three of these patients also had flow limitation in the seated position, again with both levels of NEP. Flow limitation was absent in the remaining six patients (group 2), whatever the position and NEP level. Figure 1 shows examples of the different patterns observed with an NEP of –5 cm H2O. In the supine position the degree of flow limitation with NEP levels of –10 cm H2O and –5 cm H2O was not significantly different (61 (25)% v 58 (24)%, respectively). Nevertheless, in four patients a difference exceeding 10% was noted between the two levels of NEP (patient 3: 56% at –5 cm H2O v 68% at –10 cm H2O; patient 4: 81% at –5 cm H2O v 93% at –10 cm H2O; patient 10: 26% at –5 cm H2O v 53% at –10 cm H2O; patient 16: 21% at –5 cm H2O v 53% at –10 cm H2O).
Degree of expiratory flow limitation (as % spontaneous tidal volume, %Vt) when seated and supine at both pressure levels

Examples of negative expiratory pressure (NEP) tracings (NEP –5 cm H2O; right tracings in sitting position, right tracings in supine position) illustrating the absence of flow limitation in both positions (top), the occurrence of flow limitation when shifting from the sitting to the supine position (middle), and flow limitation in both positions (bottom).
Groups 1 and 2 were similar with respect to height, weight, BMI, VC, FEV1, and FEV1/VC. The AHI was significantly higher in group 1 than in group 2 (mean difference –22 n/h (95% CI –42 to –2), p<0.05; fig 2).

Comparison of (A) the apnoea/hypopnoea index (AHI) and (B) body mass index (BMI) in groups 1 (flow limitation) and 2 (no flow limitation). Each point represents one patient, the horizontal bar marks the median of the distribution.
Correlation analysis demonstrated a significant association between the degree of flow limitation and the AHI with NEP levels of both –5 cm H2O (R=0.496, p=0.0295, 95% CI 0.054 to 0.776) and –10 cm H2O (R=0.486, p=0.0339, 95% CI 0.040 to 0.77; fig 3). This was also the case for the desaturation index (DI, number of desaturations per hour of sleep) with an NEP of –10 cm H2O (R=0.537, p=0.0376, 95% CI 0.034 to 0.823) but, as expected, a strong correlation existed between the AHI and DI (R=0.79; p<0.001). Because visual inspection of the data suggested the existence of an apnoea/hypopnoea threshold beyond which the percentage flow limitation would be linked with the AHI, the correlation analysis was repeated after logarithmic transformation of the AHI data. This improved the strength of the above associations, again with NEP levels of both –5 cm H2O (R=0.544, p=0.0147, 95% CI 0.120 to 0.801) and –10 cm H2O (R=0.531, p=0.0179, 95% CI 0.102 to 0.794). This was also the case for the DI with an NEP of –10 cm H2O (R=0.582, p=0.0274, 95% CI 0.074 to 0.850).
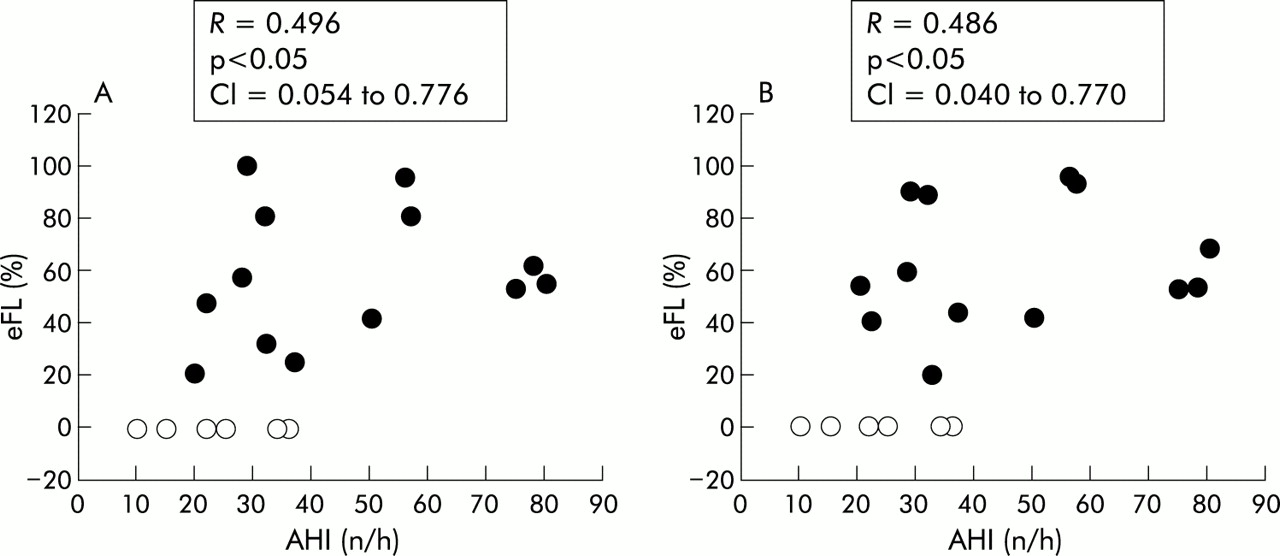
Relationship between flow limitation (eFL), expressed as the percentage of tidal volume over which the NEP induced flow does not exceed the spontaneous expiratory flow, and the apnoea/hypopnoea index (AHI) with a negative expiratory pressure (NEP) of (A) –5 cm H2O and (B) –10 cm H2O in the supine position. Closed symbols correspond to patients from group 1 (flow limited) and open symbols represent patients from group 2 (not flow limited).
No relationship was found between the degree of flow limitation and any of the anthropometric or spirometric variables.
In group 1 flow limitation of 20% or more of the tidal volume identified 100% of the patients with an AHI above 20. Flow limitation of 26% or more identified 77% of the patients with an AHI above 30.
DISCUSSION
This study confirms the work of Liistro et al6 and shows that expiratory flow limitation in the supine position is common, although inconsistent, in patients with OSAS who are free of obstructive lung disease. It also shows a significant relationship between the extent of flow limitation over tidal expiration and the severity of OSAS. This would suggest that the greater the flow limitation over tidal volume, the more abnormal is the upper airway in the apnoeic population.
Intrathoracic v extrathoracic flow limitation
It is not possible to discern the source of an expiratory limitation from NEP tracings, except when the NEP induced flow sharply and transiently becomes lower than the spontaneous expiratory flow. Such a pattern suggests acute airway closure and can be observed in normal subjects. It corresponds to the behaviour of the passive upper airway faced with a sudden negative pressure gradient (fig 4). The re-increase in the NEP induced flow that follows probably corresponds to a reflex activation of the airway dilator muscles, mainly the genioglossus.8 Apart from these accidents, a limited expiratory flow response to NEP is the same whatever the source of the limitation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Example of a negative expiratory pressure (NEP) tracing (–5 cm H2O) highly suggestive of extrathoracic expiratory flow limitation. At the beginning of the NEP induced expiration the flow in response to NEP falls below the spontaneous expiratory flow; both traces are then briefly matched and finally flow limitation disappears. This dynamic probably illustrates the effects of the activation of the genioglossus muscle in response to NEP (see text for details).
In patients with COPD, flow limitation at rest is closely linked to dynamic hyperinflation1,5 and tends to appear earlier in the supine position.1 All but one of our patients were free of any history of asthma or COPD. Their FEV1/VC ratios (table 1) and visual inspection of their expiratory flow/volume curves suggest that their limitation was not obstructive. In addition, none of them exhibited signs of hyperinflation on pulmonary function tests. We are therefore confident that the expiratory flow limitation that we observed could not be accounted for by COPD related abnormalities. Left heart failure can also induce expiratory flow limitation.2 To date this has been observed only in patients with severe cardiac disease and during episodes of acute left heart failure. Although we do not have precise cardiac evaluations in our patients and hence cannot rule out moderate cardiac dysfunction in some of them, there is no reason to think that any of them could have suffered cardiac failure to an extent sufficient to induce flow limitation. Finally, early small airway closure can be a feature of obesity in the absence of obstructive disease, and particularly so in the supine position where FRC tends to decrease independently of smoking habits.9,10 This could be another intrathoracic source of expiratory limitation. Only six patients in our study population had a BMI above 30 kg/m2 and only one could be classified as severely obese (BMI 40.5 kg/m2, table 1). We therefore consider it likely that the expiratory flow limitation patterns observed in our patients were extrathoracic rather than intrathoracic in origin.
Expiratory flow limitation and upper airway collapsibility
Augmented upper airway compliance typically occurs in patients with OSAS11,12 compared with normal subjects or non-apnoeic snorers and is a major determinant of the pathophysiology of OSAS. Indeed, the combination of increased airway compliance and abnormalities in the temporospatial repartition of the inspiratory command (that normally synchronises the activity of upper airway dilator muscle with that of inspiratory muscle) leads to an increased risk of airway collapse when the intrathoracic pressure becomes negative.12 In awake OSAS patients this can easily be shown using phrenic nerve stimulation to dissociate the activities of the upper airway dilators and the diaphragm.13
The same phenomenon can occur when the direction of the pressure gradient across the upper airway is in the opposite direction: the application of subatmospheric pressure at the nose can collapse the airway. This gives access to measurements of the critical pressure (Pcrit),12,14,15 a widely used index for characterising upper airway collapsibility in patients with sleep disordered breathing. Expiratory flow limitation with the NEP technique is therefore to be expected in this clinical setting. Its predominant occurrence in the supine position is also expected. Indeed, shifting from the seating to the supine position decreases pharyngeal areas16,17 and increases upper airway collapsiblity.18 Tantucci et al19 observed an NEP induced flow limitation in awake non-apnoeic snorers that was more pronounced in the supine position and associated with an increase in expiratory resistance.
Our study did not include a control group. This should not be an important limitation because we know from several studies that non-apnoeic and non-snoring patients of various ages do not exhibit NEP induced flow limitation. This has been shown by Tantucci et al8 and was also the case in the control group in the study by Duguet et al2 and in the series reported by Liistro et al6 in which 16 of the 22 patients with OSAS were flow limited with NEP whereas the six who were free of sleep related breathing disorders were not.
Liistro and coworkers6 found a statistically significant relationship between the degree of supine expiratory flow limitation (expressed as a percentage of tidal breathing, NEP of –5 cm H2O) and the frequency of desaturation episodes during sleep, but a possible relationship between flow limitation and the AHI was not tested. The frequency of desaturation episodes and the AHI do not provide exactly the same information. The latter is probably a more direct reflection of upper airway abnormalities than the former. In addition, the AHI is less sensitive to any prevailing gas exchange abnormality than the DI would be. This seems to be confirmed in our study by the slightly higher significance of the relationships between the degree of expiratory flow limitation and the AHI than with the DI (fig 3), particularly after logarithmic transformation of the AHI to account for the shape of the relationship. It is important to emphasise that a flow limitation of extrathoracic origin sustained during part or throughout expiration rather than being transient after the application of NEP might be taken as indicative of the incapacity of the airway dilator muscle to re-open the airway. Indeed, the genioglossus muscle is normally reflexively activated by a negative pressure at the airway opening8,20,21 which accounts for the restoration of flow that, in some cases, follows a transient limitation (fig 4). The absence of this restoration could be due either to a defect in the activation of the genioglossus muscle or to its failure to overcome the collapsing forces acting on the airway. It should be noted that at times the initial transient flow limitation depicted in fig 4 is absent and that extrathoracic flow limitation follows an initial non-limited flow pattern (fig 1). This may be due to differences in the passive mechanical properties of the upper airway but, in any case, the flow limitation prolonged over expiration should be an expression of the force imbalance that is the hallmark of OSAS which makes the correlation with the AHI logical. This hypothesis needs to be verified by studies including EMG recordings of upper airway dilator muscles and their force-balance analysis.
Interestingly, six of our patients had documented OSAS with an AHI of 10–36 events/h but did not exhibit expiratory flow limitation either in the sitting or in the supine position. One explanation for this apparent discrepancy could be the use of the oral route to apply the NEP in patients in whom the site of upper airway obstruction during sleep could have been nasopharyngeal or palatal. Indeed, the site of upper airway obstruction varies and Hudgel et al22,23 have shown that this is not predictable from pressure measurements made during wakefulness. It is interesting to note, however, that these six patients had AHI values that tended to be lower than those with expiratory limitation. Although this might be stretching the data too far, if the absence of expiratory flow limitation was indeed due to a nasopharyngeal or palatal obstruction, this would suggest that this site of obstruction determines less severe OSAS than lower obstruction sites. Further studies are needed to test this hypothesis, putting expiratory flow limitation at the precise site of the obstruction. Comparison of the response to NEP applied at the mouth and at the nose may also be of interest.
In conclusion, this study confirms that the NEP technique can detect expiratory flow limitation of extrathoracic as well as of intrathoracic origin. This implies that the upper airway must be carefully characterised in patients to whom the technique is applied before interpreting its results. When this is not possible or when there is a high suspicion of upper airway instability, studying flow in response to abdominal compression rather than to a negative airway pressure could prove useful.24 The NEP technique could also be useful for studying the collapsibility of the upper airway in patients with OSAS. Larger studies will be needed to determine the operating characteristics of the technique for OSAS screening in awake patients in routine clinical applications.
REFERENCES
Footnotes
-
Funding: This study was supported in part by ADOREP (Association pour le Développement et l'Organisation de la Recherche en Pneumologie) Paris, France.