Article Text

Abstract
Background: In infants the impedance of the nasal pathways (Zn) is a significant proportion of the total respiratory impedance (Zrs).
Methods: In 11 infants Zrs was partitioned into Zn and lower respiratory system impedance (Zlrs) using a nasal catheter. A low frequency oscillatory signal (0.5–20 Hz) was applied during a pause in breathing to obtain the impedance spectra. A model of the respiratory system containing an airway and tissue compartment was then fitted to Zrs and Zlrs. The airway compartment consisted of a frequency independent resistance (R) and inertance (I), while the tissue compartment was described by coefficients of tissue damping (G) and elastance (H).
Results: Zrs could be reliably partitioned into Zn and Zlrs. The nasal pathway acted as a purely resistive-inertive impedance and contributed approximately half of the airway resistance (mean (SE) 44.6 (4.9)%) and most of the respiratory system inertance (71.7 (3.5)%).
Conclusion: In studies investigating changes in airway resistance in nasally breathing infants, the separation of nasal and lower respiratory system mechanics will increase the sensitivity of the tests.
- nasal resistance
- respiratory impedance
- infant lung function
- G, tissue damping
- H, tissue elastance
- I, inertance
- Rn, nasal resistance
- Rrs, resistance of the respiratory system
- TGV, thoracic gas volume
- Xn, nasal reactance
- Xrs, reactance of the respiratory system
- Zn, impedance of the nasal pathways
- Zrs, total respiratory impedance
- Zlrs, impedance of the lower respiratory system
Statistics from Altmetric.com
- G, tissue damping
- H, tissue elastance
- I, inertance
- Rn, nasal resistance
- Rrs, resistance of the respiratory system
- TGV, thoracic gas volume
- Xn, nasal reactance
- Xrs, reactance of the respiratory system
- Zn, impedance of the nasal pathways
- Zrs, total respiratory impedance
- Zlrs, impedance of the lower respiratory system
In early life infants are preferential nose breathers, so the nose is an integral part of the infant's respiratory system. In studying the mechanical properties of the respiratory system it is important to study the system as used by the infant. The nasal pathway should act as a rigid tube in series with the remaining respiratory system and should thus impose a resistive and inertive load on the infant's breathing. The majority of current methodologies for ascertaining infant lung function involve measuring flow and pressure via a face mask placed over the nose and mouth. In infants the nasal resistance (Rn) may account for a significant proportion of the overall resistance of the respiratory system (Rrs).1–3 Nasal impedance (Zn)4 and resistance5,6 have been well characterised in older children and adults, while relatively few studies have been conducted in infants. Studies of Rn and Zn in infants have used a range of techniques including rhinometry,1,7,8 acoustic rhinometry,9 oesophageal manometry,2,10 and forced oscillations3 to characterise the mechanical properties of the nasal passages.
The low frequency implementation of the forced oscillation technique (LFOT) allows the measurement of the respiratory system impedance (Zrs) at frequencies including the spontaneous breathing rate (<2 Hz) and the simultaneous determination of airway and respiratory tissue mechanics. Sly and co-workers11 have described the use of the LFOT in infants. More recently, the influences of lung volume,12 chest wall,13 and inhaled bronchodilators14 and constrictors15 on Zrs have been reported. The contribution of the nasal pathway to the airway resistance and inertance (R and I, respectively) derived from the low frequency Zrs has yet to be described. The aims of the present study were to characterise the resistive and inertive properties of the nasal impedance and to determine the relative contributions of the nose to low frequency respiratory system mechanics.
METHODS
Subjects
Eleven infants aged 8–25 months recruited from the general population were studied. The infants were between 67 and 90 cm in body length and their body weight ranged from 8.7 to 14.9 kg. They were sedated with an oral dose of chloral hydrate (70–100 mg/kg) and placed in a supine position with the head supported in the midline and the neck slightly extended. Respiratory history was determined from a parental questionnaire. Eight infants had no parentally reported history of respiratory disease, while three had a history of recurrent wheeze and/or cough. All infants were asymptomatic at the time of the study and they had been free of respiratory infections for a period of at least 4 weeks. The human ethics committee of Princess Margaret Hospital for Children approved the experimental protocol. Parents gave written consent and were generally present during the study.
Measurement apparatus
Zrs was measured at a transrespiratory pressure (Prs) of 20 cm H2O as described previously.11 Briefly, the infant's lungs were raised to a Prs of 20 cm H2O three times; following the third inflation the airway opening was held occluded at the raised Prs, indecing the Hering-Breuer reflex. During the resulting pause in breathing a multifrequency forcing signal, between 0.5 and 20 Hz, was applied to the airway opening by a loud speaker via a soft rimmed face mask. Identical transducers (model 33NA002D, ICSensors, Milpitas, CA, USA) were used to detect Prs and the pressure drop across the screen pneumotachograph measuring the central airflow. Nasal pressure (Pn) was determined using a solid state catheter tip pressure transducer (MTC 5F; Drager, Best, the Netherlands). The transducer was passed through the larger nostril and placed 4–5 cm into the nasal cavity, slightly above the nasopharynx, and used to determine the respiratory system impedance distal to the nasal pathway (Zlrs). Both Zrs and Zlrs were corrected for the shunt effect of the dead space and compliance of the face mask, as described previously.11
A four parameter model of the respiratory system was fitted to the individual Zrs and Zlrs data.16 The model contained a frequency independent resistance (R) and inertance (I) and a tissue compartment characterised by the coefficients of tissue damping (G) and elastance (H): where j is the imaginary unit, ω is the angular frequency, and α is expressed as α=(2/π) arctan (H/G). Zlrs was calculated from Pn and its parameters are denoted by Rlrs, Ilrs, etc. Nasal impedance (Zn) was assumed to be an in-series component of Zrs and, accordingly, calculated as Zn = Zrs – Zlrs. Since the Zn data were found to be consistent with the impedance of a resistance (Rn) – inertance (In) pathway, Rn and In were obtained from the corresponding parameters of Zrs and Zlrs as Rn = R – Rlrs and In = I – Ilrs.
where j is the imaginary unit, ω is the angular frequency, and α is expressed as α=(2/π) arctan (H/G). Zlrs was calculated from Pn and its parameters are denoted by Rlrs, Ilrs, etc. Nasal impedance (Zn) was assumed to be an in-series component of Zrs and, accordingly, calculated as Zn = Zrs – Zlrs. Since the Zn data were found to be consistent with the impedance of a resistance (Rn) – inertance (In) pathway, Rn and In were obtained from the corresponding parameters of Zrs and Zlrs as Rn = R – Rlrs and In = I – Ilrs.
Study protocol and analysis
Four to six impedance spectra were collected in each infant with 2–3 minute intervals of spontaneous breathing interposed. The model of the respiratory system was fitted to the individual impedance data and the nasal mechanical parameters were calculated as described above. The parameter values for each infant are expressed as mean (SD) of the individual estimates. Group parameter data (R, I, G and H) are expressed as group means (SE). The effect of introducing the nasal pressure catheter was assessed in a subgroup of patients (n=4) by measuring Zrs prior to and following catheter insertion. The frequency dependence (Fd) of the nasal resistance (Rn) and reactance (Xn) was assessed by determining the slope of the regression line across the frequency range of 0.5–15 Hz for each child. Pearson product moment correlation was used to establish the relative contribution of the nasal impedance to Zrs and to examine whether the magnitude of this contribution altered with body length. Significance was accepted at p<0.05.
RESULTS
Figure 1 illustrates an averaged impedance measurement for an individual infant and its corresponding model fit for Zrs and Zlrs. Zn is also shown (Zn = Zrs – Zlrs). The negative frequency dependence of Zrs and Zlrs within both the resistive (Rrs) and reactive (Xrs) components represents the frequency dependence of the respiratory tissues. The plateau in Rrs observed at higher frequencies is associated with the frequency independent properties of the airway and nasal pathways. The resistive properties of Zn were predominantly independent of frequency, with a group mean Fd of –0.03 (0.03) (range –0.22 to 0.14). The reactive component of Zn exhibited strong linear frequency dependence across the whole spectrum, reflecting the inertive properties of the nasal cavity, with a group mean Fd of 0.91 (0.17) (range 0.44–2.46).

Representative spectra from an individual infant showing mean (SD) Zrs (•), Zlrs (▴) and Zn (▪) spectra and their corresponding model fits (solid line). Open symbols represent data points corrupted by cardiac noise and are excluded from the model fit.
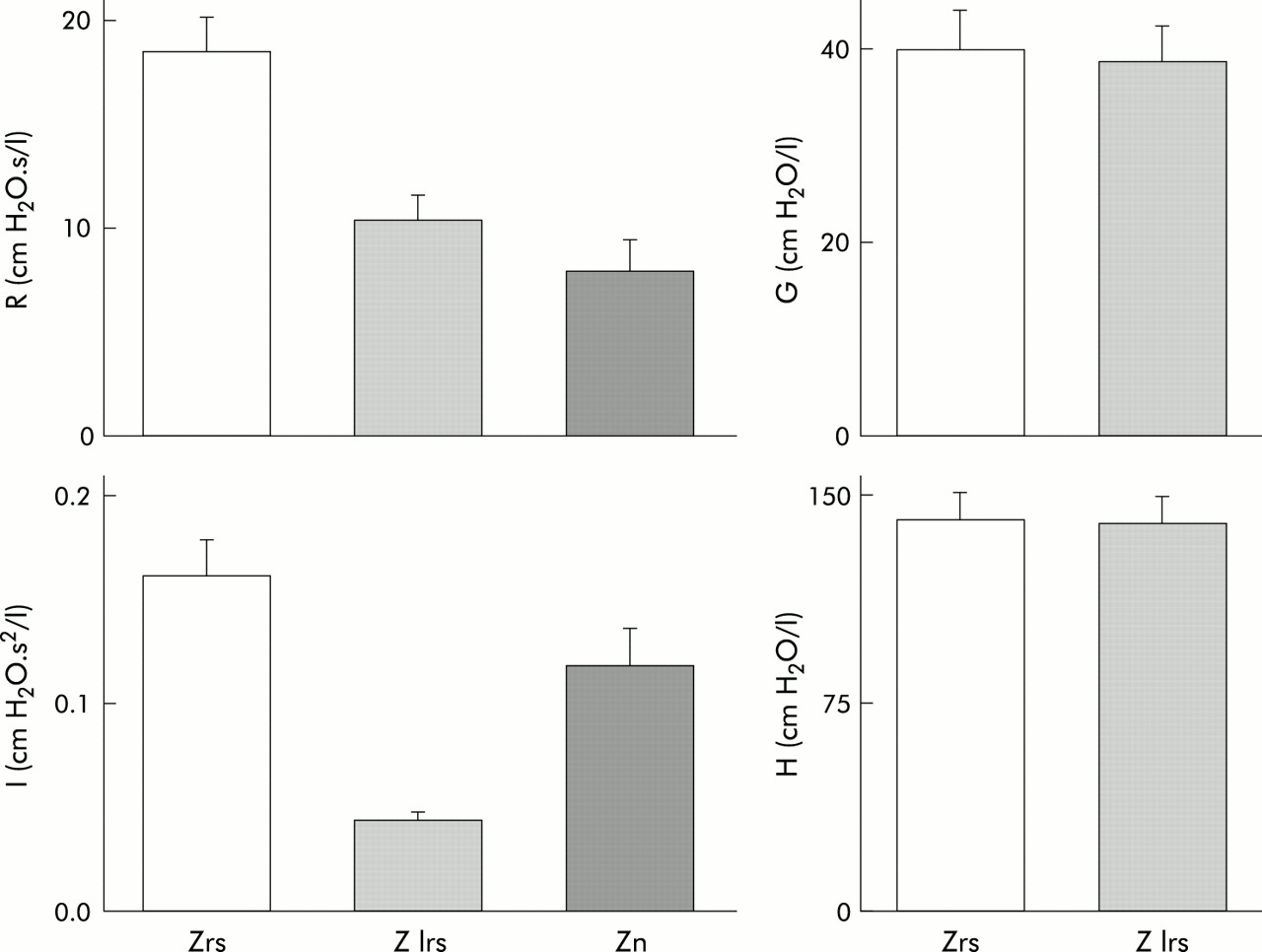
Figure 2 shows the group mean mechanical parameters for the respiratory, lower respiratory, and nasal components. Nasal impedance was found to contribute significantly to the airway properties of the respiratory system. The contributions of lower respiratory and nasal compartments to R were approximately equal (55.4 (4.9)% and 44.6 (4.9)%, respectively), while the nasal pathway dominated the inertive properties of the respiratory system (71.7 (3.5)%). The values of tissue parameters estimated from Zlrs were slightly and statistically not significantly lower than those from Zrs (38.3 (3.7) v 39.7 (3.9) cm H2O/l for G and 142.9 (10.3) v 142.8 (10.2) cm H2O/l for H). The relative contribution of the nasal pathways to the overall respiratory system mechanics was found to have no systematic variation with body length.
{kind=link}
{kind=link}
Partitioning of respiratory system mechanics (open bar) into lower respiratory (light shaded bar) and nasal (darker shaded bar) mechanics. The lower respiratory and nasal pathways contributed approximately equally to R (55.4 (4.9)% and 44.6 (4.9)%, respectively), while the nasal cavity dominated the inertive properties of the respiratory system (71.7 (3.5)%). Group mean (SE) data are shown.
In a subgroup of infants the acute effect of nasal catheter placement on Zrs was assessed. Although the group mean resistance and inertance slightly increased following catheter placement (from 15.2 (2.4) to 17.2 (2.7) cm H2O.s/l and from 0.11 (0.02) to 0.13 (0.02) cm H2O.s2/l, respectively), together with small and inconclusive decreases in G and H (from 34.5 (9.2) to 32.4 (6.1) cmH2O/l and from 132.7 (12.7) to 128.8 (11.3) cm H2O/l, respectively), none of these changes was statistically significant.
DISCUSSION
This study was designed to determine the contribution of the nose to the mechanical properties of the total respiratory system. Low frequency respiratory and lower respiratory impedance spectra were determined in 11 sedated infants during the Hering-Breuer reflex apnoea at a transrespiratory pressure of 20 cm H2O. A model containing a simple airway and a constant phase tissue compartment17 was fitted to these impedance spectra allowing simultaneous assessment of the airway and tissue mechanics of the respiratory system. The contribution of the nose to the mechanical properties of the respiratory system was also quantified.
Partitioning of Zrs into Zn and Zlrs
The results showed that the LFOT could be adapted to obtain reliable estimates of nasal impedance. Measurements of Rn using rhinometry are well established in adults and older children.5,18–20 The forced oscillation technique has also been applied in adults using measurements at the mouth and nares,21 utilising the Valsalva manoeuvre22 or by measuring impedance at the mouth with the nose open and closed.4 These techniques have proved difficult to translate into an infant population who are unable to perform voluntary manoeuvres. Stocks and Godfrey described an adaptation of the posterior rhinometry technique for use in infants,1 while Desager et al3 applied the forced oscillation technique to determine the Fd of Zn above 8 Hz. The present study is the first to quantify the resistive and inertive properties of the nasal impedance and to partition the low frequency Zrs in infants into its lower respiratory and nasal components.
Our impedance data are consistent with the assumption that, once the effect of the face mask compliance is removed,11 there remain no appreciable shunt elements distal to the airway opening that may lead to differences between the airflow measured and that entering Zlrs: the observed minor and statistically insignificant differences between G and Glrs and H and Hlrs can readily be attributed to calibration inaccuracies and/or negligible inconsistencies in model fitting. Therefore, in the low frequency range studied, Zn can be regarded as an in series component of Zrs and its frequency dependence is consistent with that of a relatively rigid walled, resistive-inertive pathway.
Contribution of Rn to Rrs
Nasal resistance was found to contribute 44.6 (4.9)% to the Newtonian resistance of the respiratory system in the present study, which compares well with the reported values of 49% from posterior rhinometry1 or 2–49% with the forced oscillation technique above 8 Hz.3 We note here that, since the amplitude of the oscillatory flow was kept low (0.06–0.08 l/s) in order to avoid involvement of non-linear effects in the nasal passages, the contribution of Rn to Rrs must have been smaller than that in the case of spontaneous breathing. Desager et al3 measured Rrs between 4 and 52 Hz and reported values at two discrete frequencies (24 and 48 Hz). The mean slope between these frequencies was then calculated to determine Fd. The authors reported minimal frequency dependence in both normal and asthmatic children, and slightly negative Fd values in children with a higher Rn. In the present study there was no significant frequency dependence of Rn, confirming that the frequency dependence of Rrs results from the mechanical behaviour of the pulmonary tissues.11,16
Contribution of Xn to Xrs
The nasal cavity provided the dominant contribution to the inertive properties of the respiratory system (71.7 (3.5)%) and this was manifested in a marked decrease in the resonant frequency when Zn was included in the measurement, with the resonant frequencies of Zlrs and Zrs being 13.6 (2.3) Hz and 6.7 (1.0) Hz, respectively. Previous studies have not attempted to determine the influence of Xn on Xrs. Desager et al3 reported a positive frequency dependence of Xn between 24 and 48 Hz in 19 asthmatic infants. They observed mean Xn values of –0.9 (3.7) cm H2O.s/l and –0.1 (1.9) cm H2O.s/l at 24 and 48 Hz, respectively; these negative values are at variance with our Zn data and may express the increasing influence of upper airway wall properties at higher frequencies.
Acute influence of nasal catheter placement
We observed no significant changes in the respiratory parameters following nasal catheter placement. In contrast, Stocks et al7 reported an increase in Rn in a group of preterm infants when a nasogastric feeding tube was passed through the larger nostril, with the changes becoming more pronounced when the tube was passed through the smaller nostril. While both studies used an identically sized catheter (FG5), the noted differences may be attributed to the relative sizes of the infants at the time of testing. In the previous study7 the preterm infants were studied in the first 4 weeks of postnatal life, whereas the current study was performed in term infants ranging from 8 months to 2 years postnatal age. Hence the cross section area of the nose in the present study would be considerably larger and the effects of the catheter accordingly reduced. In the current study the nasal catheter was passed through the larger nostril; it is possible that, had the smaller nostril been used, we may have found some differences in our estimations of respiratory mechanics. We conclude that the presence of the catheter did not lead to any appreciable overestimation of Zn and its contribution to Zrs in the present study.
Changes in Zn with body length
In a cross sectional study, Stocks and Godfrey1 found that the absolute values of Rn decreased monotonically from birth to the end of the first year of postnatal life when plotted against thoracic gas volume (TGV). However, the percentage contribution of Rn to airway resistance remained relatively constant against TGV and this finding is consistent with that of the present study. The contribution of the nasal pathway to the airway properties of the respiratory system in the present population was relatively constant in infants of different length. This suggests that, as an infant grows, the rates of change of the mechanical properties of the respiratory system below the nasopharynx and the nose with body length are approximately equal.
In conclusion, the present study has shown that the nasal resistance significantly contributes to the respiratory system resistance, while the inertive properties of the nose dominated the overall inertance of the respiratory system. Since therapeutic interventions and/or challenge tests may impact differently on the mechanical properties of the upper and lower tracts of the respiratory system, the ability to partition the respiratory system into nasal and lower respiratory system compartments will provide a greater degree of sensitivity to diagnostic tests that wish to assess changes in respiratory system mechanics.
Acknowledgments
This study was funded by grants from the National Health and Medical Research Council of Australia (#941252) and the Ministry of Health of Hungary (ETT 591/1996 06).