Article Text

Abstract
Background: Protease activated receptor-2 (PAR-2) is a transmembrane G protein coupled receptor preferentially activated by trypsin and tryptase. The protease activated receptors play an important role in most components of injury responses including cell proliferation, migration, matrix remodelling, and inflammation. Cigarette smoking causes an inflammatory process in the central airways, peripheral airways, lung parenchyma, and adventitia of pulmonary arteries.
Methods: To quantify the expression of PAR-2 in the central airways of smokers and non-smokers, surgical specimens obtained from 30 subjects undergoing lung resection for localised pulmonary lesions (24 with a history of cigarette smoking and six non-smoking control subjects) were examined. Central airways were immunostained with an antiserum specific for PAR-2 and PAR-2 expression was quantified using light microscopy and image analysis.
Results: PAR-2 expression was found in bronchial smooth muscle, epithelium, glands, and in the endothelium and smooth muscle of bronchial vessels. PAR-2 expression was similar in the central airways of smokers and non-smokers. When smokers were divided according to the presence of symptoms of chronic bronchitis and chronic airflow limitation, PAR-2 expression was increased in smooth muscle (median 3.8 (interquartile range 2.9–5.8) and 1.4 (1.07–3.4) respectively); glands (33.3 (18.2–43.8) and 16.2 (11.5–22.2), respectively); and bronchial vessels (54.2 (48.7–56.8) and 40.0 (36–40.4), respectively) of smokers with symptoms of chronic bronchitis with normal lung function compared with smokers with chronic airflow limitation (COPD), but the increase was statistically significant (p<0.005) only for bronchial vessels.
Conclusions: PAR-2 is present in bronchial smooth muscle, glands, and bronchial vessels of both smokers and non-smokers. An increased expression of PAR-2 was found in bronchial vessels of patients with bronchitis compared with those with COPD.
- smoking
- chronic obstructive lung disease
- bronchitis
- G protein coupled receptors
Statistics from Altmetric.com
Receptors that are activated by proteolysis (protease activated receptors, PARs) belong to an emerging family of seven transmembrane domains, the G protein coupled receptor superfamily.1,2 PAR-3 and PAR-4 are activated by thrombin, whereas PAR-2 and PAR-4 are activated by trypsin and tryptase. Northern blot analysis has revealed the presence of PAR-2 in a variety of human tissues with a high abundance of mRNA in kidney, pancreas and intestinal tissue and less mRNA in the heart and lungs.3,4 In intact tissues, junctional receptors for PAR-2 were first demonstrated in rat vascular and gastric smooth muscle5 and, recently, immunohistochemical localisation of PAR-2 has been reported in human bronchial smooth muscle, epithelium,6 and in mast cells from various normal human tissues.7 Evidence has accumulated for both a protective and a proinflammatory effect of PAR-2 in the airways. In different animal species and in humans, activation of PAR-2 may initiate protective mechanisms in response to both airway inflammation and increased airway tone,8–,10 or it may cause bronchoconstriction.11
PAR-2 may be a critical element in airway inflammation,12 repair, and tissue remodelling.13 The recent observation that tryptase, possibly by acting on PAR-2, is an important stimulus for the proliferation of human airway smooth muscle cells in asthmatic airways14 and that it induces lung fibroblast proliferation via activation of PAR-215 is of considerable interest.
It is well established that cigarette smoking causes an inflammatory process in both central and peripheral airways and in lung parenchyma.16 Increased numbers of both macrophages and T lymphocytes have been described in the central airways of smokers, whereas in smokers who develop chronic obstructive pulmonary disease (COPD) there is an increased number of CD8+ T lymphocytes in central, peripheral airways and in the adventitia of pulmonary arteries.17 As the severity of airflow limitation increases, there is a parallel increase in the number of neutrophils in the airways.16 In addition, mast cell infiltration and degranulation has been described in the bronchial glands of smokers with symptoms of chronic bronchitis.18 However, none of these studies has completely clarified the mechanisms involved in the inflammatory process present in the airways of smokers. To the best of our knowledge, precise immunohistochemical characterisation of the distribution of PAR-2 expression in the central airways of smokers and non-smokers has never been attempted.
The aim of this study was to characterise PAR-2 expression in the central airways of smokers and non-smokers.
METHODS
Subjects
Thirty patients undergoing lung resection for a solitary peripheral carcinoma were examined, of whom 24 had a history of cigarette smoking (14 current smokers, 10 ex-smokers for more than 2 years). Seven had symptoms of chronic bronchitis and normal forced expiratory volume in 1 second (FEV1) (bronchitic patients), eight had symptoms of chronic bronchitis and fixed airway obstruction (COPD patients), and nine were asymptomatic with normal lung function. We also examined six asymptomatic non-smokers with normal FEV1. Chronic bronchitis was defined as cough and sputum production occurring on most days of the month for at least 3 months of the year during the 2 years prior to the study.19 Fixed airway obstruction was defined as FEV1 <80% predicted with a reversibility of <15% after inhalation of 200 μg salbutamol. Subjects with chronic bronchitis had had no exacerbations, defined as increased dyspnoea associated with a change in the quality and quantity of sputum, that had led them to seek medical attention during the month preceding the study. All subjects had been free of acute upper respiratory tract infections and none had received glucocorticoids or antibiotics within the month preceding surgery, or bronchodilators within the previous 48 hours. They were non-atopic (negative skin tests for common allergen extracts) and had no past history of asthma or allergic rhinitis.
The study conformed to the Declaration of Helsinki and informed written consent was obtained for each subject. Each subject underwent an interview, chest radiography, electrocardiography (ECG), routine blood tests, skin tests with common allergen extracts, and pulmonary function tests in the week before surgery.
Pulmonary function tests
Pulmonary function tests included measurements of FEV1 and forced vital capacity (FVC) (Biomedin Spirometer, Padova, Italy). The predicted normal values used were those from the European Coal and Steel Community (ECSC).20 In order to assess the reversibility of airway obstruction in subjects with a baseline FEV1 of <80% predicted, the FEV1 measurement was repeated 15 minutes after inhalation of 200 μg salbutamol.
Histology
Bronchial rings were taken from the lobar or segmental bronchus of the lobe obtained at surgery, away from the tumour site. They were fixed immediately in freshly prepared 1% paraformaldehyde in phosphate buffered saline (PBS, pH 7.4) for 6 hours, washed twice (1 hour) with PBS containing 15% sucrose, embedded in OCT compound, snap frozen in isopentane precooled in liquid nitrogen, and stored at –70°C for later use.
Serial cryostatic sections 10 μm thick were immunostained with a rabbit anti-rat polyclonal antibody. PAR-2 antiserum B5 was raised in rabbits to a synthetic peptide fragment of rat PAR-2 (30GPNSKGR ↓ SLIGRLDT46P-YGGC ↓), coupled to keyhole lympet haemocyanin (YGGC added for conjugation = trypsin cleavage site).21,22 PAR-2 was detected by the streptavidin-biotin complex peroxidase method and the peroxidase activity was revealed using the nickel enhancement method, as previously described.23 Briefly, endogenous peroxidase activity was blocked by immersing slides in 0.3% hydrogen peroxide in methanol for 30 minutes. After washing in PBS, non-specific binding was blocked by incubating in 3% normal swine serum in PBS containing 0.05% bovine serum albumin (BSA) and 0.1% sodium azide for 30 minutes. The sections were then incubated overnight at 4°C with the primary antibody (1:1000 dilution). Negative controls were performed by preabsorbing the antibody with the non-conjugated immunogenic peptide diluted at 10–3 or 10–5 M in the antibody (1:1000 dilution) and incubating overnight before application to the tissue. Further negative controls were performed by the omission of the primary antibody. After washing in PBS the sections were incubated for 30 minutes with biotinylated swine anti-rabbit IgG antibody (E431, Dako, High Wycombe, UK). The sections were washed and incubated for 60 minutes with streptavidin-biotin complex reagent (StreptABComplex/HRP, K0377, Dako), and immunoreactivity was visualised with 3`-3` diaminobenzidine. They were then dehydrated and mounted in Eukitt.
Light microscopic analysis of the vessels and bronchial glands of the bronchial submucosa in the coded slides was performed with a Zeiss microscope (Zeiss, Germany). An eyepiece graticule with a graded scale was superimposed on the microscopic field and vessels were counted at a magnification of ×312 in the area 500 μm beneath the epithelial basement membrane in non-overlapping fields until all the available area was covered. The number of total vessels/high power field (HPF) did not differ between the four groups of subjects examined. Results were expressed as a percentage of the number of PAR-2 positive vessels/number of total vessels examined. Acini of bronchial glands were counted at a magnification of ×500 in alternate non-overlapping fields until all the gland area was covered. The number of total acini/HPF did not differ between the groups of subjects examined. The results were expressed as the percentage of the number of PAR-2 positive acini/number of total acini examined. The percentage of both PAR-2 positive vessels and acini was evaluated on slides counterstained with haematoxylin.
The area of bronchial smooth muscle positive for PAR-2 was evaluated with an image analysis system (Windows Image version 3.4, Casti Imaging, Venice, Italy). Images of microscopic fields at a magnification of ×100 were captured via a video camera attached to a microscope (Leyca, Germany). The area was measured in the image by interactive delineation. Using the computer mouse, the boundaries of the bronchial wall (considered as the area between the basement membrane and the bronchial cartilage) and the boundaries of PAR-2 positive bronchial smooth muscle were delineated. The number of pixels included within the boundaries was converted to the tissue area using a factor determined by calibrating the image analyser with a graded scale viewed using the same microscope and objective used for the study. The area of bronchial wall was the same in the four groups of subjects examined. The results were expressed as the percentage of PAR-2 positive bronchial smooth muscle area/bronchial wall area.
The number of PAR-2 positive epithelial cells was counted using a microscope (Leyca, Germany) at magnification ×630. The length of the basement membrane was evaluated by image analysis. Results were expressed as the number of PAR-2 positive epithelial cells/mm basement membrane. To increase the accuracy, the percentage of PAR-2 positive smooth muscle area and the number of PAR-2 positive epithelial cells were evaluated on slides not counterstained with haematoxylin because of the difficulty of distinguishing the positive signal from the counterstaining on the computer screen of the image analyser.
Statistical analysis
Group data were expressed as mean (SE) values or as medians and interquartile ranges (IQR) where appropriate. Differences between groups were analysed using the non-parametric Kruskal-Wallis analysis of variance (ANOVA) followed by the Mann-Whitney U test for non-normally distributed data. The unpaired Student's t test was used for normally distributed data. Probability values of p<0.05 were accepted as significant. At least three replicate measurements were performed by the same observer in 10 randomly selected slides, and the intra-observer reproducibility was assessed with the intraclass correlation coefficient for repeated measurements.
RESULTS
Clinical findings
The characteristics of the subjects examined are reported in table 1⇓. Smokers and non-smokers were similar with regard to age. The number of packs/year was similar in the three groups of smokers, but the number of years of smoking was significantly different between asymptomatic smokers and bronchitic patients (32 (3.5) v 49 (2.8), p<0.05) and between asymptomatic smokers and patients with COPD (32 (3.5) v 50.8 (2.2), p<0.01). As expected from the selection criteria, COPD patients had a significant lower FEV1 (% predicted) and FEV1/FVC ratio than did asymptomatic smokers and patients with bronchitis. COPD patients (FEV1 <80% predicted) showed no significant response to bronchodilators (range 3.8–5.4%).
Characteristics of subjects
Immunohistochemical findings
Quantification of PAR-2 was satisfactory in bronchial smooth muscle, bronchial glands, and in bronchial vessels in all subjects. By contrast, because the epithelium was not well preserved in all samples, quantification of PAR-2 in bronchial epithelium was satisfactory in five asymptomatic smokers, four patients with bronchitis, five with COPD, and five non-smokers.
The intraclass correlation coefficients for at least three repeated measurements were 0.8 for vessels, 0.6 for glands, 0.7 for smooth muscle, and 0.6 for epithelium.
Positive immunostaining for PAR-2 was found in the bronchial smooth muscle layer (fig 1⇓), the bronchial glands (fig 2⇓), the endothelium and smooth muscle of bronchial vessels (fig 3⇓), and the bronchial epithelium (fig 4⇓). Preabsorption of PAR-2 antibody with the non-conjugated immunogenic peptide completely abolished the staining.
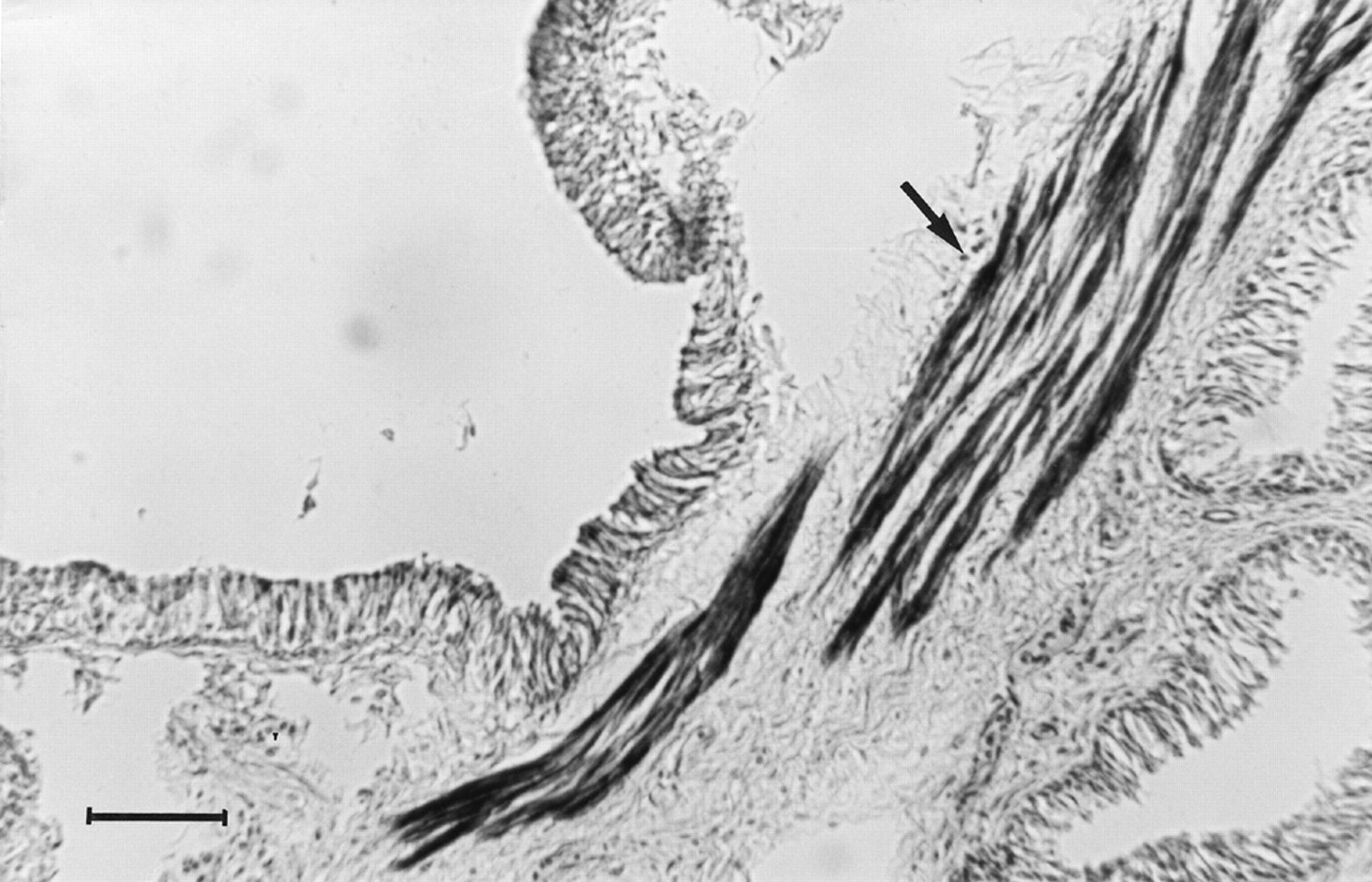
Photomicrograph showing PAR-2 immunostaining (arrow) in bronchial smooth muscle. Bar = 85 μm.

Photomicrograph showing PAR-2 immunostaining (arrow) in bronchial glands. Bar = 34 μm.
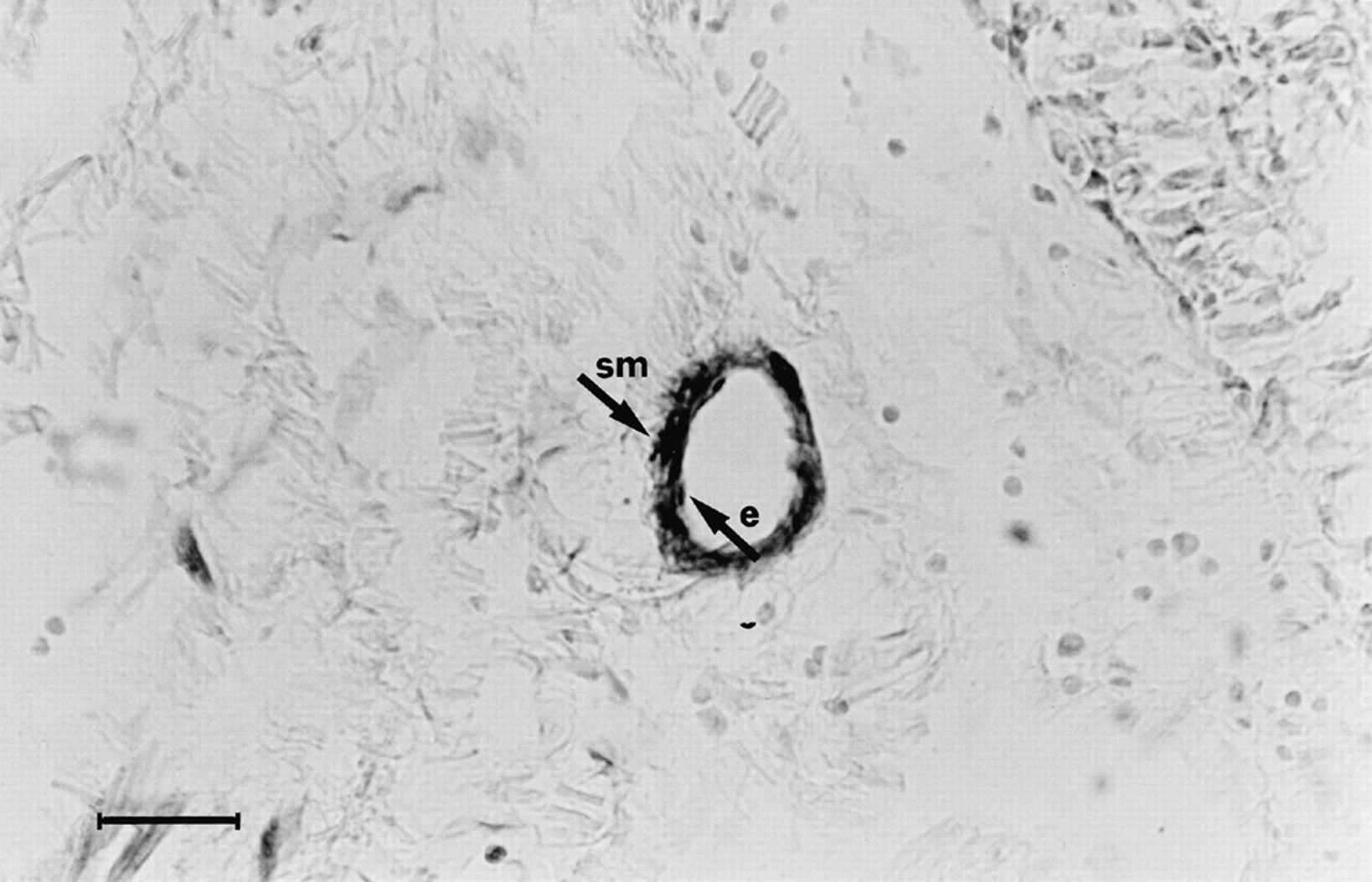
Photomicrograph showing PAR-2 immunostaining (arrows) in endothelium and smooth muscle of bronchial vessels (e = endothelium; sm = smooth muscle). Bar = 34 μm.

Photomicrograph showing PAR-2 immunostaining (arrow) in bronchial epithelium. Bar = 34 μm.
No significant differences were observed in the PAR-2 expression of the central airways between smokers and non-smokers (table 2⇓). When smokers were divided into current smokers and ex-smokers, ex-smokers showed a trend towards increased PAR-2 in bronchial smooth muscle (median 4.9 (IQR 2.1–6.1)); vessels (48.1 (40.0–54.9)), and epithelium (25 (20.0–50.0)).
PAR-2 expression in different structures of central airways of non-smokers and smokers*
When the population of smokers was divided according to the presence of symptoms of chronic bronchitis and of chronic airflow limitation, no significant differences in PAR-2 expression in bronchial smooth muscle between asymptomatic smokers, symptomatic smokers with normal lung function (patients with bronchitis), and patients with COPD were found (fig 5A⇓). In the bronchial glands there was a trend towards increased PAR-2 expression in patients with bronchitis (median 33.3 (IQR 18.2–43.8)) compared with COPD patients (median 16.2 (IQR 11.5–22.2); Mann-Whitney U test, p<0.05; Kruskal Wallis analysis of variance, p>0.05; fig 5B⇓). In bronchial vessels PAR-2 expression was significantly increased in smokers with symptoms of chronic bronchitis and with normal lung function (median 54.2 (IQR 48.7–56.8)) compared with patients with COPD (median 40.0 (IQR 36–40.4); Mann-Whitney U test, p<0.005; Kruskal Wallis analysis of variance, p<0.05; fig 5C⇓). The median (IQR) number of total bronchial vessels/HPF was similar in all groups. In particular, the number of bronchial vessels was 0.8 (0.8–0.9) and 0.8 (0.6–1.2) in patients with bronchitis and COPD, respectively.

Individual values of percentage of (A) area of smooth muscle positive for PAR-2 normalised by bronchial wall area, (B) PAR-2 positive acini normalised by number of total acini examined, and (C) PAR-2 positive bronchial vessels normalised by number of total vessels examined. Horizontal bars represent median values. AS = asymptomatic smokers with normal lung function; B = smokers with symptoms of chronic bronchitis and normal lung function (bronchitic subjects); COPD = smokers with symptoms of chronic bronchitis and chronic airflow limitation.
No significant differences in PAR-2 expression in the epithelium were seen between the groups.
When symptomatic smokers with and without chronic airflow limitation were considered together, PAR-2 expression in bronchial glands and in bronchial vessels was positively correlated with % predicted FEV1 (p<0.05, ρ = +0.59 and p<0.002, ρ = +0.74, respectively; fig 6⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between (A) percentage of PAR-2 positive acini/total acini and FEV1 (% predicted) and (B) percentage of PAR-2 positive vessels/total vessels and FEV1 (% predicted) Open circles = COPD patients; closed circles = bronchitis patients. Rho and p values correspond to Spearman's rank correlation coefficient.
DISCUSSION
We have shown that PAR-2 expression is present in bronchial smooth muscle, bronchial glands, bronchial vessels, and the epithelium of both smokers and non-smokers. Our experiments indicate that PAR-2 expression is similar in the central airways of smokers and non-smokers, but increased PAR-2 expression is seen in the bronchial vessels of patients with bronchitis compared with those with COPD. In patients with bronchitis there was also a trend toward increased PAR-2 expression in bronchial smooth muscle (threefold increase) and in bronchial glands (twofold increase). To our knowledge, this is the first study to attempt to quantify the expression of PAR-2 in human central airways.
Cigarette smoking is associated with an inflammatory process, but the characteristics of the airway inflammatory process of smokers who develop COPD compared with those who do not are still under investigation. Cigarette smoking is a major risk for the development of COPD, but it is unknown why some smokers develop symptoms of chronic bronchitis and others develop chronic airflow limitation. Chronic mucus hypersecretion and chronic airflow limitation may coexist in the same subject, but chronic bronchitis and chronic airflow limitation might be considered as separate entities.
We hypothesised that PAR-2 expression would be increased in the airways of smokers since proinflammatory agents upregulate PAR-2 on endothelial cells, and because PAR-2 agonists, including tryptase, induce neurogenic inflammation, stimulate vasodilation, plasma extravasation, neutrophil infiltration, and cause secretion of proinflammatory cytokines.24–,28 The findings of similar PAR-2 expression in the airways of smokers and non-smokers and of decreased PAR-2 expression in the airway structures of COPD patients compared with bronchitic patients with normal lung function were unexpected. Possible explanations for the first finding could be that PAR-2 has no role in the airway inflammatory process of smokers or that its role is evident only in peripheral airways. Other explanations include the possibility that the study was perhaps underpowered for the trends seen to be significant. The discrepancy between the second finding and our hypothesis may reflect a downregulation of the receptor which may occur under pathological circumstances. We cannot exclude the possibility that an increased stimulus of tryptase released from mast cells of patients with COPD18 might have caused a downregulation of receptor expression. Other explanations include a different cytokine environment in chronic bronchitis and in COPD that could affect PAR-2 expression.
The functional consequence of the increased PAR-2 expression in bronchial vessels and probably in bronchial glands and bronchial smooth muscle of subjects with symptoms of chronic bronchitis—that is, with chronic mucus hypersecretion—but without chronic airflow limitation is, at the moment, uncertain. A possible role for PAR-2 in mucus secretion comes from studies showing that trypsin interacts with PAR-2 to increase [Ca2+]i and activates ion channels in dog pancreatic duct epithelial cells29 and that, in the rat, sublingual PAR-2 triggers mucin secretion, at least in part, via activation of tyrosine kinase.30 The trend towards increased PAR-2 expression in the bronchial smooth muscle of smokers with symptoms of chronic bronchitis and with normal lung function compared with COPD patients is more difficult to explain as conflicting results in the literature suggest or rule out a bronchoprotective role for PAR-2. Cocks and coworkers have shown that activation of PAR-2 causes relaxation of airway preparations from mouse, rat, guinea pig, and humans by release of a cyclooxygenase product from the epithelium.8,10 We observed that symptomatic smokers with normal lung function had a trend towards increased PAR-2 expression in all the central airway structures, suggesting a possible protective role at least towards the development of chronic airflow limitation. The positive correlation observed in our study between lung function (% predicted FEV1) and PAR-2 expression in acini and vessels supports this hypothesis.
The increased PAR-2 expression in bronchial vessels of subjects with symptoms of chronic bronchitis but without chronic airflow limitation underlines the importance of vascularisation in patients with chronic bronchitis and COPD. It is established that smokers who develop COPD exhibit endothelial dysfunction in pulmonary arteries, inflammatory cells with a prevalence of CD8+ T lymphocytes in the adventitia of the same arteries, and increased expression of E-selectin on vessels and of ICAM-1 on basal epithelial cells.16 However, in spite of extensive investigations on the effects of cigarette smoke on the pulmonary vasculature, studies have focused more on muscular pulmonary arteries than on bronchial vessels and the precise functional significance of vascular changes is unknown. It is noteworthy that this study showed a similar number of total bronchial vessels in smokers and non-smokers, and in symptomatic smokers with and without chronic airflow limitation, indicating that cigarette smoke does not cause increased vascularity, at least in central airways, and that the increased PAR-2 expression is not the result of an increase in the number of vessels.
How could PAR-2 have an effect on the interactions between cigarette smoke, inflammatory cells, bronchial vessels, smooth muscle, glands, epithelium, chronic mucus hypersecretion, and chronic airflow limitation? This question cannot be answered exhaustively until the endogenous protease responsible for activating this receptor in vivo has been identified. This study has shown that the signal for PAR-2 is more relevant in bronchial vessels where immunostaining is present in both endothelium and smooth muscle. It is known that endothelial cells express PAR-2,31 that PAR-2 activation stimulates an endothelium dependent nitric oxide mediated relaxation of isolated vascular tissue,32 that trypsin expression is present in vascular endothelial cells,33 and that upregulation of both protein and mRNA for PAR-2 follows vascular injury and is greatest in areas containing actively proliferating cells,34 suggesting a role for PAR-2 in the remodelling of vessels. Endothelial cells are potentially exposed to a variety of extracellular proteases, particularly during vascular injury or inflammation.35 It should be noted that endothelial cells in most anatomical locations are unlikely to encounter trypsin, and therefore it cannot be ruled out that PAR-2 activation is caused by other proteases.35
Finally, because of recent reports that the proinflammatory cytokines tumour necrosis factor (TNF)-α and interleukin (IL)-1α can cause a marked increase in PAR-2 expression in human endothelial cells,24 and that a surprising number of IL-4 and IL-5 mRNA positive cells are present deep in the bronchial wall of smokers with chronic bronchitis but not of those with COPD,36 it is possible that changes in PAR-2 expression may be a result of a different cytokine environment.
The population of smokers with symptoms of chronic bronchitis and with normal lung function seems to be a “distinct” group. The subjects included in this study were all in a stable condition with no recent clinical exacerbations and none had taken glucocorticosteroids in the month prior to the study. These inclusion criteria exclude the possibility of an effect of both severity of disease and of anti-inflammatory treatment on changes in the expression of PAR-2. A confusing element in any study performed on specimens surgically resected from patients with lung cancer is that cancer itself may influence the results. However, compared with bronchial biopsies, specimens obtained at surgery allow analysis of the entire bronchial wall. Moreover, as a result of our having examined only tissue away from the tumour site, we feel confident that our findings of an upregulation of PAR-2 in bronchial vessels of symptomatic smokers with normal lung function are valid.
In conclusion, by using immunohistochemical techniques we have mapped the expression of PAR-2 in the central airways of smokers and non-smokers. Positive immunostaining was found in the bronchial smooth muscle layer, bronchial glands, smooth muscle and endothelium of bronchial vessels, and in the epithelium. PAR-2 expression was similar in the central airways of smokers and non-smokers. However, a significant increase in PAR-2 expression was seen in the bronchial vessels of smokers with symptoms of chronic bronchitis and with normal lung function compared with patients with COPD.
Acknowledgments
The authors thank Drs G Cavallesco and G Azzena for their expert collaboration, and G Fulgeri for typing the manuscript.
REFERENCES
Footnotes
This study was supported by MURST (60%, 40%), ARCA, Ferrararicerche, Azienda Ospedaliera di Ferrara and NIH DK 43207.