Article Text

Abstract
The study of patients being weaned from mechanical ventilation has offered new insights into the physiology of respiratory failure. Assessment of the balance between respiratory muscle strength, work and central drive is essential if difficulty in weaning occurs, and optimisation of these elements may improve the success of weaning. Psychological support of patients and the creation of units specialising in weaning have also resulted in a higher success rate.
- critical care
- weaning
- ventilation
Statistics from Altmetric.com
Difficulty in weaning from mechanical ventilation is associated with intrinsic lung disease and/or a prolonged critical illness. After critical illness the incidence of weaning failure varies with 20% of all admissions failing initial weaning.1,2 The incidence of weaning failure increases in patients who have been ventilated for many weeks but is low (<5%) in patients who undergo elective surgery such as after cardiopulmonary bypass.3 In a recent audit in our intensive care unit (ICU) of patients who had received mechanical ventilation for more than 72 hours, weaning was the dominant clinical problem during recovery and accounted for over half of the total time spent on the ICU. The mean number of weaning episodes was 5 per patient.
When assessing patients clinically, it is useful to determine whether the patient has yet to start weaning, is in the middle of a weaning attempt, is not yet ready to wean, or will never be able to wean. A simple assessment screen consisting of the concentration of inspired oxygen relative to the arterial oxygen tension, the level of positive end expiratory pressure (PEEP), the amount of sedation, and the inotropic requirements can be performed every day in patients receiving mechanical ventilation. The screen identifies patients who may be successfully weaned and reduces the number of patients receiving mechanical ventilation for more than 21 days.4 Furthermore, passing the screening test is associated with reduced in-hospital mortality.4 This review concentrates on patients who are difficult to wean from mechanical ventilation, many of whom will have made repeated attempts at weaning.
PREDICTING THE LIKELY SUCCESS OF WEANING
Although much has been written about the assessment of weaning, many studies do not set a numerical threshold for a score which is then tested prospectively. This important element of study design has resulted in many papers using retrospective analysis and may in part explain the variability of study results. For example, tachypnoea is an indicator of weaning failure in some studies5 but not in others.2
Apart from study design, other influences are important when interpreting the ability of a test to predict weaning success. Tests should be standardised and reproducible.6 Although many tests are standardised in the laboratory or in normal subjects, few studies have been performed on standardisation of weaning parameters in the critically ill.7 Similarly, their reproducibility in the ICU environment is crucial. A further problem is that many studies have been performed on a heterogeneous group of patients.
SIMPLE BEDSIDE TESTS
Spirometric tests of lung function have been used frequently and are often quoted as predictors of weaning. Although early reports suggested that minute ventilation, maximal pressure generation, and the ability to increase minute ventilation (maximal voluntary ventilation) were useful, further studies have not reproduced these findings. Indeed, although some of the commonly used tests have high sensitivity, their specificity is often surprisingly low (table 1).
Commonly quoted predictive variables of weaning8
Rapid shallow breathing
A common finding in patients who fail to wean is the early development of rapid shallow breathing when the ventilator is disconnected.5 This represents the coordinated response of the patient to the ventilatory load applied. The attractive features of this assessment are that it tests the whole ventilatory system and requires that the patient be disconnected from the ventilator, thus indicating whether or not the patient can breathe in a controlled environment. Rapid shallow breathing (frequency divided by tidal volume, f/Vt) is best assessed with the patient breathing with continuous positive airway pressure (CPAP) at the level of PEEP used during mechanical ventilation. Rapid shallow breathing has a sensitivity of 0.97 with a specificity of 0.64.8 Weaning parameters with a low specificity result in some patients, who are able to breathe independently, being prevented from weaning. By encouraging all patients to be disconnected from the ventilator this may in part be avoided.
Combined tests
Combining measurements may improve one’s ability to predict weaning outcome. Sassoon and Mahutte9 repeated the analysis of rapid shallow breathing but combined it with the occlusion pressure in the first 100 ms (P0.1), an index of central drive. At this early phase of respiration, where little length has changed, the pressure generated is related to the degree of stimulation to the respiratory muscles. Although the combination of f/Vt and P0.1 provided the most sensitive and specific predictor, receiver operator curve (ROC) analysis showed only a modest gain with the addition of P0.1.
Yang and Tobin8 devised the CROP index ((Cdyn × Pimax × [Pao2/Pao2])/rate) which consisted of dynamic compliance (Cdyn), maximum mouth pressure (Pimax), oxygenation (Pao2/Pao2), and respiratory rate. This was no better than f/Vt alone when assessed prospectively. Measurements integrating ventilatory endurance and the efficiency of gas exchange yield the most successful results but are complex and difficult to use.10
COMPONENTS OF WEANING FAILURE
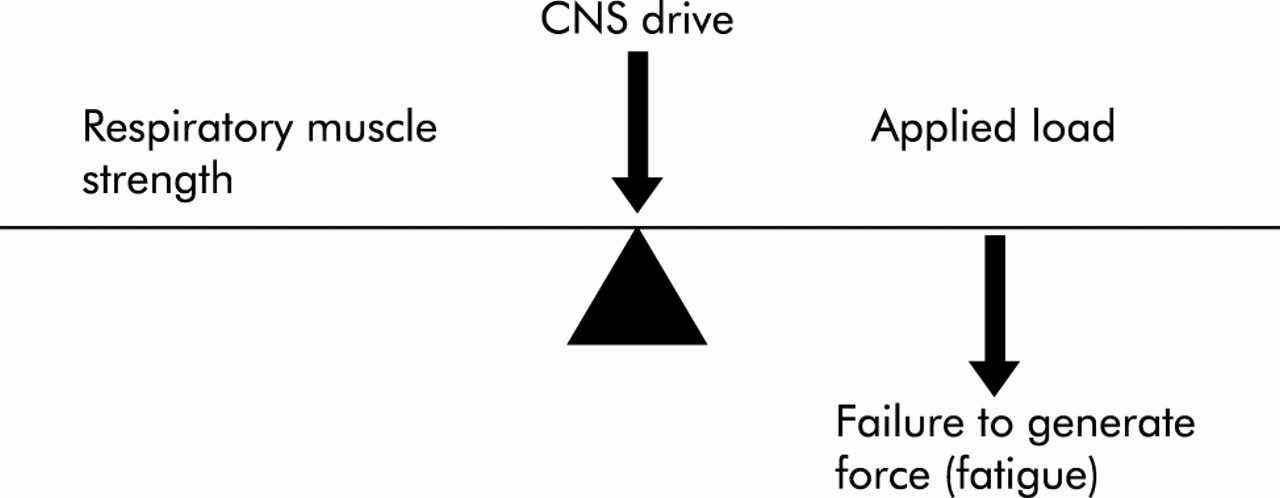
Weaning from mechanical ventilation depends on the strength of the respiratory muscles, the load applied to the muscles, and the central drive (table 2). Respiratory failure may result from disorders in one of these three areas—for example, a myopathy reducing strength, acute bronchospasm suddenly increasing load, or opiates acting on the central nervous system. However, it is also possible that disorders of strength and load occur together.
The three determinants of ventilation and common pathophysiological conditions associated with failure to wean
The relationship between these three key components of spontaneous breathing may be visualised as a balance (fig 1). If the muscles are heavily loaded, spontaneous contraction cannot be maintained and the muscles may fail acutely. Such acute reversible failure of force generation is termed fatigue. This has been shown in studies of both electromyography (EMG)11,12 and changes in the relaxation rate of respiratory muscles during weaning.13 The pathophysiology of weaning failure has been studied in small groups of patients.13–15 It seems likely that the dominant feature is high levels of load relative to the strength of the respiratory muscles. As weaning progresses, load increases compared with those who succeed a weaning trial. In most cases the drive to breathe is high.15
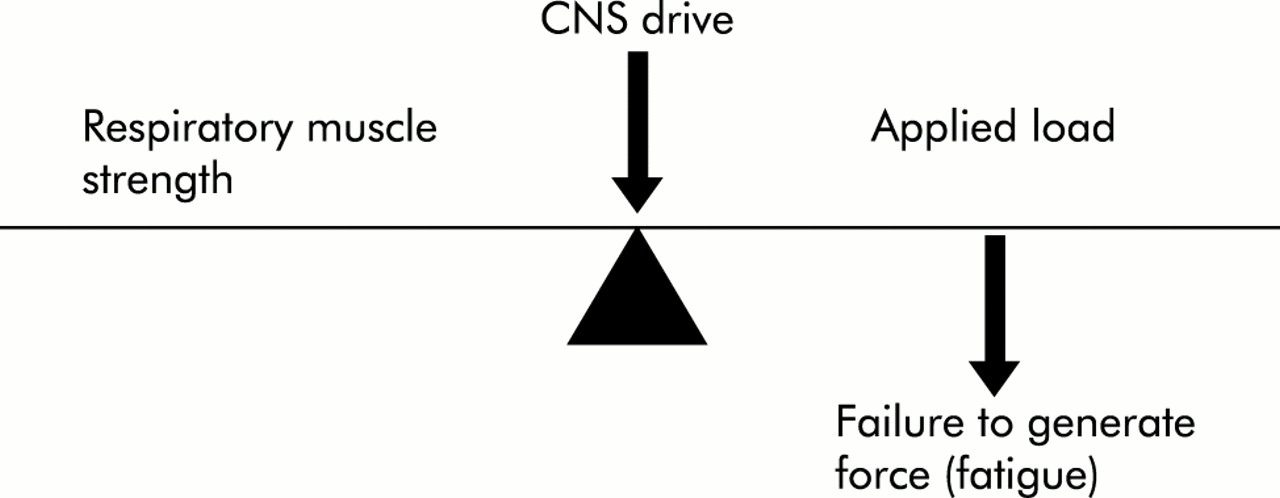
Key components of spontaneous breathing. Drive from the central nervous system acts on the peripheral respiratory muscles. The balance between the components can be disordered, leading to fatigue of the respiratory muscles, failure to generate force, and a decrease in alveolar ventilation.
Respiratory muscle strength
Originally the tension of the respiratory muscles was tested in normal subjects by taking maximum pressure measurements at the mouth (Pimax),16,17 while oesophageal and gastric balloon catheters allow the study of diaphragmatic strength. Contractions of the diaphragm can be obtained by electric or magnetic stimulation of the phrenic nerves.18,19
In the intubated patient maximal pressure generation can be assessed during occluded maximal manoeuvres and this can be simply performed as the endotracheal tube is easily accessible. Pimax was originally measured in intubated patients being weaned from mechanical ventilation by Sahn and Lakshminarayan.1 Patients with severe weakness (Pimax <20 cm H2O) were unable to wean. However, as a sole indicator of the ability to breathe spontaneously, muscle strength alone may not predict success or failure. Severely weak muscles can only sustain spontaneous breathing if all other factors are entirely normal.
The measurement of respiratory muscle strength on the ICU presents more challenges.20 Firstly, generating maximal pressure with an artificial airway leads to movement of the endotracheal tube which inhibits maximal pressure generation. Secondly, many patients cannot sustain the one second plateau pressure demanded by the original Pimax protocol.16 Lastly, few patients can coordinate respiration to ensure that they reach residual volume before maximum inspiratory effort.
In order to improve the ability of patients and normal subjects to perform a maximal inspiratory manoeuvre, brief inspiratory efforts were investigated during gasping against a closed airway with pressure measured in the endotracheal tube.13,21 Inspiration against an occluded airway is well tolerated by patients provided the technique is well explained and that the gasping does not continue for longer than 20 seconds. An advantage of the gasp is that maximal efforts build up over the 3–8 inspiratory efforts. This technique has been used to measure strength in patients who are not fully conscious, enabling a voluntary estimate to be made in a group of patients who were previously unable to comply with a volitional protocol.21
When the reproducibility of the measurement of inspiratory strength was assessed in intubated patients, the between observer, within day, and between day variability of inspiratory efforts were very variable.22 The observation of a low (weak) inspiratory pressure has to be treated with caution. However, a strong effort is reassuring and unlikely to be an artifact. Finally, non-volitional magnetic stimulation of the diaphragm has been applied to the critically ill. This technique may enable studies to be performed that will address the time course and extent of respiratory and skeletal muscle weakness in critically ill patients.23
Aetiology of respiratory muscle weakness in the critically ill
Although most patients are weak, the precise cause of weakness is not always known. Causes of acute weakness include electrolyte disturbances such as hypophosphataemia and hypomagnesaemia. Although electrolyte abnormalities are relatively common on the ICU, their significance in this context is unknown. Long term weakness may be due to critical illness itself. Disuse of skeletal muscles leads to atrophy, where the reduced cross section of the muscle decreases maximum tension. This process is rapid and 7–10 days of disuse may decrease maximum pressure generation by the diaphragm by 50%.24 Critical illnesses are commonly associated with a polyneuropathy,25 with or without a myopathy.26 Such patients may present with extreme weakness, mainly in the legs, and tetraplegia is possible.27
If the muscles are weak, can we improve strength with exercise or training? Skeletal muscle responds to training regimens by increasing mass and cross sectional area. For a training regimen to be effective it must be controlled, such that the task is repetitive and supramaximal with periods of rest between training exercises.28 In addition, strength training differs conceptually and in practice from endurance training.29 For the respiratory muscles, training is ill defined and although it is felt that the respiratory muscles should behave in a similar manner to other muscle groups, definitive studies have yet to show how they may be trained. It is likely that the response to training will in part be genetically determined. The general observation that some individuals are responsive to and have ability at certain types of exercise has led to studies showing genetic differences in the response to training according to genotype.30 A genetic polymorphism of the angiotensin converting enzyme (ACE) gene has been described with a 256 base pair deletion or insertion, termed DD or II.31 In de-trained subjects there is an 11-fold difference between homozygous subgroups in response to performing a repetitive biceps exercise.30 Recently, respiratory muscle strength and endurance was studied in de-trained subjects who underwent general non-specific training. Respiratory muscle endurance was increased fivefold in the II subgroup.32
Central nervous system drive
Although central respiratory drive is not often measured on the ICU, it is possible to measure P0.1, an index of drive.33 P0.1 is raised when respiratory drive is artificially increased during a hypercapnic challenge and is also high in patients suffering ventilatory failure.34 In intubated patients it is often the case that little or no gas flows in the early part of inspiration, if valves are required to open and the speed of response is slow. In such circumstances, patients may be making occluding breathing efforts and P0.1 may be measured within the airway automatically by the ventilator.35
Can P0.1 be used to assess weaning from mechanical ventilation? It is easy to apply the technique to ventilated patients and, when respiratory drive is raised, the measured pressure exceeds 5.5 cm H2O. A raised P0.1 is associated with failure to wean.36 Interestingly, patients who are able to breathe during weaning trials not only have a low P0.1 but are also able to increase drive and minute ventilation during a hypercapnic challenge.37 Patients who are able to breathe spontaneously do so with a lower central drive and also have some ventilatory reserve, contrasting with the fixed capacity of patients who fail to wean.
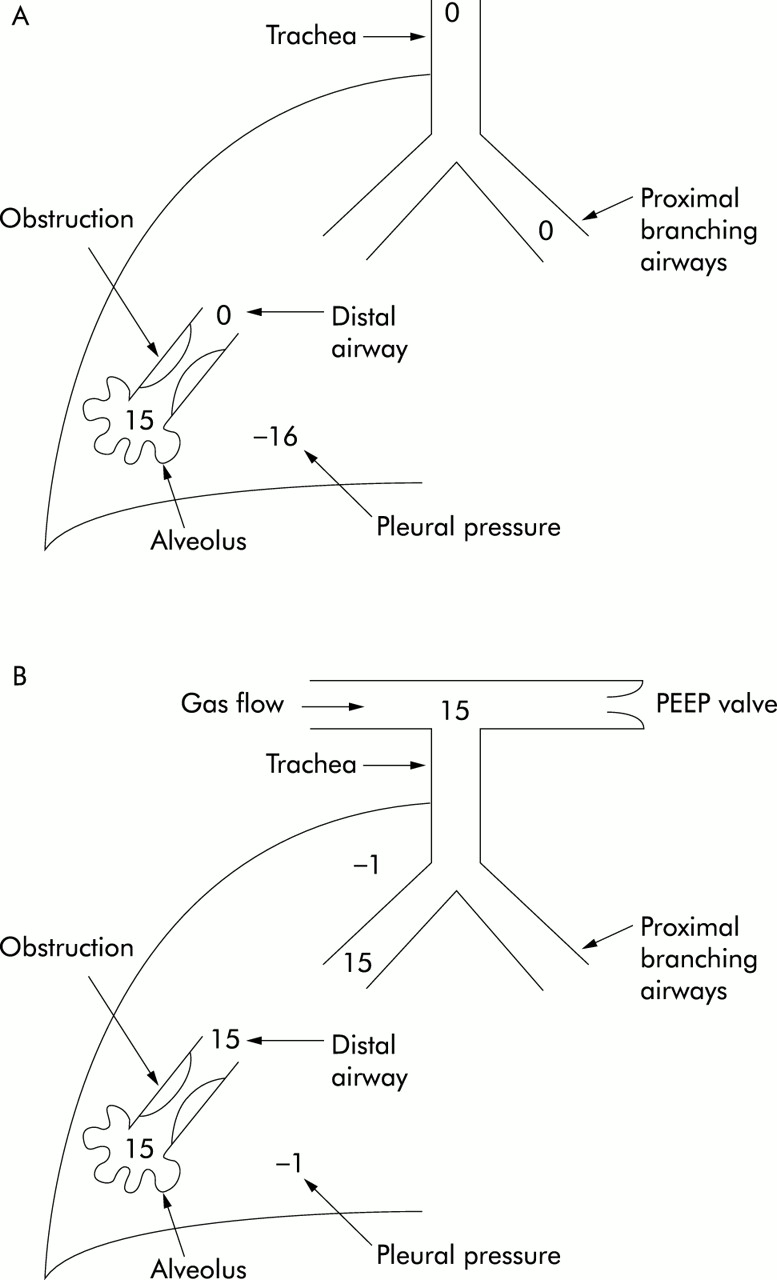
Respiratory drive has been measured in patients receiving pressure support ventilation where the level of pressure support was decreased in stages.38 It would follow that, as the amount of support decreases, there will be a moment when drive to the muscles increases. In patients who were able to breathe spontaneously, the level of drive remained low. Conversely, in patients who fail to wean, drive increased, often above the level seen previously. It is possible that the level of ventilatory support could be titrated in this manner, keeping the level of drive within the “normal” range for patients on the ICU. A similar approach was used to adjust the level of external PEEP applied to patients with varying degrees of intrinsic PEEP.39 As the level of external PEEP increased, the ability of the patients to achieve gas flow reduced until the optimum balance of internal and external PEEP was reached (fig 2). Respiratory drive increased if external PEEP achieved hyperinflation, enabling the adjustment of external PEEP to the correct level without requiring the difficult measurement of internal PEEP in the spontaneously breathing patient.
{kind=link}
{kind=link}
The threshold load effect of intrinsic or auto-positive end expiratory pressure (PEEP). When auto-PEEP is high, no gas flow will occur at the mouth until the pressure generated within the chest exceeds the level of intrinsic PEEP. (A) The pressure within the alveolus cannot fall to zero because of the obstruction to expiratory flow. The pressure to begin gas flow must be less than the level of intrinsic PEEP, in this case –16 cm H2O. (B) External PEEP is applied, balancing the intrinsic PEEP. This has the effect of reducing the pressure required to begin inspiratory flow, in this case from –16 to –1 cm H2O.
Load applied to the muscles
Work is performed when a force moves through a distance and is termed “external” as it may be easily measured. Internal work is performed when there is no movement, when the muscle contracts and produces tension and heat. To calculate external work in the respiratory system, the tidal volume must be integrated with respect to the transpleural pressure generated during the breath. This requires some measure of pleural pressure, usually obtained from oesophageal balloon catheters, and simultaneous measurement of volume at the mouth. Internal work can be imagined if there is no gas flow, as occurs in complete obstruction. In this circumstance, energy is dissipated against distortions of the chest wall and no ventilation occurs.
Work is often increased in weaning failure40,41 and successful weaning occurs when work is reduced. It is possible to monitor work continuously and, in those who fail to wean, pressure generation is significantly higher at the end of the weaning trial, inspiration as a fraction of the respiratory cycle lengthens, and patients are tachypnoeic.
CLINICAL IMPLICATIONS
Exhaustive breathing may damage skeletal muscle fibres and cause a reduction in the ability to generate pressure. Indeed, in healthy volunteers the strength of the diaphragm as judged by magnetic twitch transdiaphragmatic pressure is substantially reduced up to 24 hours after breathing to exhaustion through an inspiratory resistance of 60% of maximal.42
Failure to wean from mechanical ventilation does not exclusively affect respiratory muscle performance. The oxygen consumption of muscles can rise considerably and changes in gut mucosal pH indicate that an oxygen debt occurs during failed weaning attempts.43,44 More organ specific disorders occur when the level of respiratory work is high. In patients at risk of coronary artery disease, weaning precipitates ischaemia45 which may not be detected at the bedside, particularly if three lead ECG monitoring is used. Weaning is less likely to succeed if myocardial ischaemia occurs.46 Furthermore, mechanical ventilation supports left ventricular function in patients with incipient heart failure.47 Hence, invasive haemodynamic measurements and radionuclide imaging in patients showed decreased left ventricular performance and oesophageal pressure, and a 2–3-fold increase in pulmonary artery occlusion pressure when weaning failed. Re-ventilation reversed this effect and subsequent treatment to support the myocardium led to successful weaning. Heart failure in patients who fail to disconnect from mechanical ventilation is an important differential diagnosis.
Triggering mechanical ventilation is an important aspect of setting the ventilator when patients are breathing spontaneously. Triggering from the inspiratory flow reduces work involved in triggering compared with pressure triggering.48 If the trigger sensitivity is set inappropriately, it is difficult to breathe through the ventilator and, in weak patients, it is possible that no breath is delivered and de-synchrony occurs. Improvements in trigger methodology have decreased inspiratory work, with flow triggering becoming the standard. In health, ventilators can now be set such that almost no work is performed to initiate a breath. Mechanical ventilation in severe lung disease is a greater challenge, especially in obstructive lung diseases where the transmission of the inspiratory effort to the upper airway may be delayed. When the time delay is prolonged, the ventilator senses inspiration at a point when the inspiratory muscles are contracting. Thus, persistent respiratory muscle contraction leads to occult internal work being performed. Instead of conventional triggering at the ventilator end of the airway, sensing inspiration at the distal tip of the endotracheal tube would avoid some of the time delay in patients with chronic obstructive pulmonary disease (COPD). Experimentally, it is possible to compare conventional triggering with triggering at the ventilator, and substantial reductions in the work can be achieved. It is possible to move the inspiratory trigger even closer to the respiratory muscles, offsetting the delay in triggering if pressure is sensed within the chest. Oesophageal triggering has recently been found to reduce total inspiratory work in normal volunteers.49
RECENT ADVANCES IN MECHANICAL VENTILATION
Proportional assist ventilation (PAV)
A conventional ventilator has one variable that is determined by the user. For example, in the pressure control mode the airway pressure can be manipulated. During the breath the volume delivered to the patient depends on the mechanics of the lung and chest wall. With PAV the ventilator measures the compliance and resistance of the system during each breath. The ventilator can then be set to deliver the pressure required for a given tidal volume, or a proportion of it, depending on the gain of the system set by the operator. PAV can unload the respiratory muscles to a greater extent than other modes of ventilation. It can compensate for dynamic changes in resistance and compliance and allow the patient to vary tidal breathing, maintaining the amount of intrinsic muscle effort set by the operator.50,51 Similar technology can be applied to the work required to breathe through an endotracheal tube. By measuring the resistance and compliance of a standard endotracheal tube, automatic tube compensation (the amount of assistance relative to the inspiratory flow rate) can be provided.52
Hyperinflation
Expiratory flow limitation causes hyperinflation and increased resting end expiratory pressure. This is termed auto or intrinsic PEEP,53 and it acts as a load during inspiration as the patient must generate a negative pressure equal to the level of auto-PEEP in order to generate gas flow at the mouth that triggers inspiration. Asynchrony with the ventilator may be caused by excessive auto-PEEP and may be resolved by matching the external applied PEEP to balance the system.54 In normal subjects, such a load would be easily borne. For example, an average level of intrinsic PEEP of 11 cm H2O is a small fraction of the total pressure generating ability. However, many intubated patients generate a maximum of –30 cm H2O. In this context, overcoming the threshold load effect of intrinsic PEEP uses 33% of available pressure generation and may contribute to fatigue.
Techniques of weaning
Important studies in the 1990s established that the mode of ventilation has a major influence on the success of weaning. Brochard et al55 compared weaning by pressure support (PS), T-piece trials, and synchronised intermittent mandatory ventilation (SIMV) in a group of patients who had failed to wean and in whom it was predicted that weaning would be problematic. Over a period of 28 days SIMV was clearly inferior to the other techniques, with an advantage in favour of the PS group. This study also emphasised the importance of a weaning protocol. The Spanish Lung Failure Collaborative Group reported contrasting findings.56 While SIMV was clearly less favourable, T-piece weaning was advantageous overall. Although both studies showed that SIMV was disadvantageous, the explanation for the differing findings between PS and T-piece weaning may relate to differences in study design. For example, the duration of mechanical ventilation was different between the two studies, with fewer longer term patients in the Spanish study.
Non-invasive ventilation (NIV)
NIV has several advantageous features for weaning patients, including the absence of sedative drugs, early removal of the endotracheal tube, a decrease in ventilator associated pneumonia, and better compliance with chest physiotherapy.57 These advantages have seldom been studied in a controlled manner and to date the majority of studies have been performed in patients with chronic respiratory failure in an effort to avoid endotracheal intubation.
In 22 patients referred to a specialist chronic ventilation unit for weaning from mechanical ventilation, NIV was rapidly tolerated in 20 and many were extubated quickly.58 Ten patients required nasal ventilation at night when discharged home. Although this study was not controlled, it certainly shows that patients who are difficult to wean can be extubated and may be managed in a high dependency area using NIV support.
Psychological support
Psychological disturbance occurs during weaning trials and feelings of hopelessness affect performance.59 Clinically, there appears to be a gap between the physiological testing performed at the bedside and the actual performance of the patient, some of which may be attributable to other factors including personality, fear, agitation, depression, and empowerment.60 Weaning is associated with depression and treatment may be helpful.61 An important element of the care of patients during weaning is to devise methods of psychological support.62 One example is to ask the patient to imagine a particularly strong memory and through rehearsal this fantasy is strengthened. The memory is then used during weaning to allay anxiety and increase tolerance of reductions in ventilatory support.
Specialist weaning units
The demand for ICU beds has led to the development of facilities specialising in weaning.63,64 Weaning units tend to admit patients with single organ failure who do not require complex organ support. Such units are more cost effective, with dramatic reductions in both the fixed overheads and the consumable cost associated with weaning. Moreover, by concentrating effort in a specialist area and through the development of protocols to guide the weaning effort, it is possible to decrease the time spent on mechanical ventilation.63,65,66