Article Text

Abstract
Background: There is a concern that comorbidity or frailty in older people could limit the usefulness of currently available exercise tests for chronic lung disease. This study evaluated the feasibility and reproducibility of the incremental shuttle walking test (SWT) in people aged 70 years or over, compared exercise tolerance with other disability markers, and assessed whether the SWT is responsive to change after bronchodilators.
Methods: Fifty elderly patients with chronic airflow limitation (CAL) and 32 controls without airflow limitation attempted the SWT before and after combined nebulised salbutamol/ipratropium bromide. Subjects also completed the Nottingham Extended Activities of Daily Living index (NEADL) and the London Handicap score (LHS).
Results: Forty four subjects with CAL (88%) and 29 controls (84%) completed the SWT, including many with co-morbidities. Two week repeatability was good and the SWT was strongly associated with EADL (r=0.51, p<0.001) and LHS (r=0.43, p<0.004), but only weakly with forced expiratory volume in 1 second (FEV1) (r=0.31, p=0.05). Subjects with CAL walked a mean distance of 177.7 m compared with 243.3 m in controls (p<0.001); following bronchodilator therapy the distance walked increased in the CAL group by 13.2% (p=0.009).
Conclusion: The SWT is a feasible and reproducible measure of exercise tolerance in elderly people with and without airflow obstruction and correlates with other markers of disability. It is sensitive to change following bronchodilation in subjects with CAL, although the change correlates less well with improvements in FEV1. Overall, these results suggest that the SWT might be an appropriate measure to assess interventions in elderly people.
- exercise tests
- geriatrics
- chronic airflow limitation
- bronchodilator response
Statistics from Altmetric.com
Impaired exercise tolerance is an important feature of airways obstruction1 and its measurement is a useful marker of disability. Exercise training is a key element of pulmonary rehabilitation, and several different methods have been employed to determine its benefit in such programmes. However, the traditional methods of assessing exercise performance, such as cycle ergometry and treadmill testing, may not be relevant to usual exercise patterns2 and may prove difficult for many elderly people. Self-paced walking tests, such as the 6 or 12 minute walk,3,4 have also been criticised because they can be influenced by patient motivation and encouragement.5 These problems prompted the development of the shuttle walking test (SWT)6 which is an incremental and progressive walk around two cones placed 10 metres apart. It was designed to stress the individual to a symptom limited maximum performance. However, its use in an elderly population with chronic lung disease has not been specifically examined, although this group is increasingly being included in pulmonary rehabilitation programmes.7 Furthermore, patient frailty and comorbidity may reduce the value of any test to assess the respiratory limitation of exercise.
Another useful reason to assess exercise tests specifically in elderly subjects is to determine whether they could be used to assess bronchodilator response,8 either in addition to or instead of spirometric tests. An increase in exercise tolerance would provide a rationale for bronchodilator therapy even in the absence of a spirometric response, although this has not been studied in detail previously. The current study was undertaken with three main aims: (1) to assess the reproducibility of the incremental SWT in elderly people; (2) to relate the results to measures of disability and lung function, and (3) to determine whether the SWT is responsive to change induced by bronchodilators.
METHODS
Subjects
Fifty non-institutionalised subjects aged 70 or over with a diagnostic label of “asthma” were recruited from primary care practices. All subjects had a Barthel score of at least 17 out of 20 and a Mini-Mental State Examination score of at least 24 out of 30—that is, they were non-demented subjects. Thirty two control subjects of the same age without known respiratory disease were recruited from the same primary care lists. All subjects completed the MRC Respiratory Symptoms Questionnaire, the Nottingham Extended Activities of Daily Living (NEADL) index9 which measures disability on a scale of 0–22 (22 = no limitation detected), and the London Handicap score (LHS)10 on a scale of 0–100 (100 = no handicap detected).
All participants gave written informed consent and the study was approved by South Birmingham Health Authority research ethics committee.
Lung function tests
Subjects were asked to abstain from smoking, caffeine, or bronchodilators (oral and inhaled) on the day of testing, and attendance was deferred in those who reported an upper respiratory tract infection or exacerbation of wheezing in the previous 6 weeks. Spirometric tests were performed (wedge bellows, Vitalograph, UK) to measure forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and vital capacity (VC) in accordance with protocols from national guidelines,11 and values were related to reference ranges.12 The spirometric tests were repeated 30 minutes after the administration of a combination of nebulised salbutamol (5 mg) and ipratropium bromide (0.5 mg).
Shuttle walking test
The course was established in the corridor of the Lung Investigation Unit and the speed of walking was dictated by a timed signal played on a cassette recorder. Within the first 2 minutes the subjects were advised to increase or decrease their speed if required, but no further encouragement was given. The test ended if the subject was unable to continue (due to breathlessness or any other reason) or was unable to get to the next cone before the timer sounded. The test was repeated 30 minutes after nebulised bronchodilators as detailed above.
Although a practice walk is recommended, it proved to be too exhausting for some subjects to perform three test walks within an hour. The protocol was therefore modified so that, if subjects failed to understand the test appropriately in the first 2 minutes, it was stopped and restarted after a 20 minute rest period. As a learning effect is recognised in similar tests,13 the magnitude of such an effect in older people was assessed by asking 10 subjects with a diagnostic label of asthma to repeat the test on a subsequent visit conducted within 2 weeks of the original test.
Statistical analysis
A significant bronchodilator response was defined as an increase in FEV1 of at least 15% (minimum 200 ml) as recommended.14 Two week test-retest repeatability was calculated according to methods described by Bland and Altman.15 Data were compared within groups using paired Student's t tests and between groups using unpaired Student's t tests. Associations were tested using Pearson's correlation coefficient for parametric data, or Spearman's test where the data were non-parametric. SPSS software (release 6.0) was used to analyse the data and a p value of <0.05 was considered significant.
RESULTS
The characteristics of the subjects are shown in table 1. Subjects with a diagnostic label of asthma were found to have various degrees of airflow obstruction on spirometric testing before administration of the bronchodilator and were felt to be better described as having chronic airflow limitation (CAL). All such subjects complained of respiratory symptoms and were taking at least one respiratory related medication. Although 11 control subjects reported breathlessness when walking along the flat and three reported daily production of sputum, none of them had spirometric evidence of airflow obstruction. The subjects with CAL were more disabled and handicapped than the control subjects, although all subjects were able to walk independently.
Characteristics of study subjects
Lung function
The results of the spirometric tests are summarised in table 2. In the control group 29 subjects (91%) were able to perform the spirometric tests according to national guidelines, while 39 of the patients with CAL (78%) were able to perform reproducible spirometric traces. A significant FEV1 bronchodilator response was observed in 19 subjects with CAL (49% of cases tested), in nine of whom FEV1 increased to at least 80% of predicted values. In the control group FEV1 was more than 80% predicted in 27 subjects, with a minimum value of 76% in the remaining two subjects. Only one control subject had a significant increase in FEV1 from 2.3 l to 2.7 l (19.0%), although the pre-bronchodilator FEV1 was >80% predicted and this subject was asymptomatic.
Pre- and post-bronchodilator lung function and shuttle walk results
Reproducibility of SWT
In the 10 subjects with CAL whose SWT was repeated at 2 weeks (pre-bronchodilator) the mean distance walked increased from 171.0 m to 177.0 m (3.5%) between tests. Using the Bland-Altman method,15 the standard deviations of the results of individual subjects were plotted against their mean values (fig 1) and showed that there was no relation between the two (Kendall's tau=0.05, p=0.8). The mean within-subjects variance was calculated as 153.37, giving a standard deviation of 17.89 m (the measurement error). The coefficient of repeatability was therefore calculated as 35.1 m (1.96 × 17.89).

Shuttle test repeatability in subjects with chronic airflow limitation (CAL) by the Bland-Altman method. The third shuttle walking test was performed within 2 weeks of the baseline test. SD = standard deviation.
SWT in control subjects
The SWT was successfully performed by 27 (84%) of the control subjects in whom the mean (SE) distance walked increased from 243.3 (21.4) m pre-bronchodilator to 256.2 (21.9) m post-bronchodilator, although the change was not statistically significant (p=0.36). All subjects stopped because of limitation in their mobility and not breathlessness. Three control subjects increased their walking distances by more than 35.1 m (the calculated coefficient of repeatability for the CAL group), although these were from much higher baseline levels than in the subjects with CAL.
SWT in CAL subjects
In the subjects with CAL 44 (88%) of the 50 subjects were able to perform the SWT satisfactorily, including nine subjects who were unable to perform satisfactory spirometric tests. The total distance walked was significantly lower in the CAL group than in the control group (p<0.001, independent sample t test). The distance walked increased from 177. 7 (14.6) m pre-bronchodilator to 195.0 (16.8) m post-bronchodilator (p=0.009), representing a 13.2% change on average (range –35.7 to 160.0%). Breathlessness was the limiting factor in 20 subjects, mobility in 21, and other reasons such as “giddiness” in three others. The increase in distance walked was >35.1 m (or more than three “shuttles”) in 10 subjects, eight of whom stopped due to shortness of breath. In the breathlessness group as a whole (n=20) the mean (SE) distance walked changed by 32 m (24.1%) from 205.0 (14.5) m pre-bronchodilator to 237.0 (15.7) m post-bronchodilator (p=0.01). However, in those 19 subjects with a significant post-bronchodilator rise in FEV1, only six subjects increased their walking distance by >35.1 m.
Associations
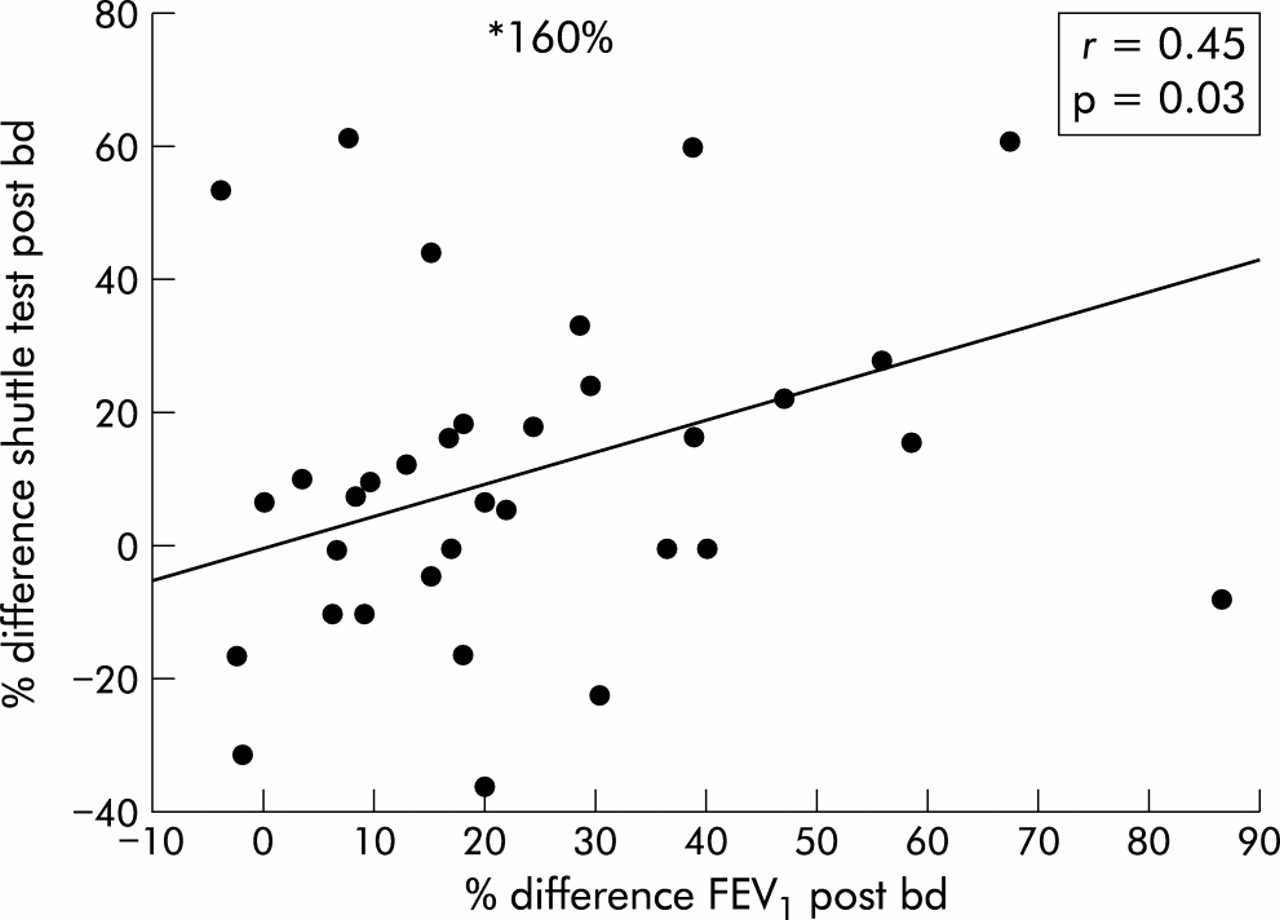
There was no association between SWT and increasing age. FEV1 and SWT were weakly but significantly associated pre-bronchodilator (Pearson's r=0.31, p=0.05), as anticipated from other studies.6,16 VC was more strongly related to SWT (Pearson's r=0.42, p=0.01) although the scatterplot was visually poor. The SWT was, however, significantly associated with the NEADL score (Spearman's r=0.51, p<0.001; fig 2) and also with the LHS (Spearman's r=0.43, p=0.004). Post-bronchodilator FEV1 associations were slightly poorer with NEADL (Spearman's r=0.40, p<0.01), similar for LHS (Spearman's r=0.43, p=0.004), and slightly stronger for SWT (Pearson's r=0.38, p=0.02). There was also a fair association between change in FEV1 and change in SWT distance following bronchodilators (Pearson's r=0.45, p=0.03; fig 3).

Association between SWT and EADL score in subjects with chronic airflow limitation (n=44); bd = bronchodilators.
{kind=link}
{kind=link}
{kind=link}
Association between change in SWT and change in FEV1 following bronchodilators (bd) in subjects with chronic airflow limitation (n=35). Nine subjects who completed the SWT were unable to perform spirometric tests.
DISCUSSION
The feasibility and value of exercise testing in older adults with respiratory disease has received little attention. Exercise tests are acknowledged to be a valuable indicator of disability in rehabilitation programmes and in a range of other related assessments.17 Elderly people are increasingly likely to enrol in such programmes, and outcome measures that are used to assess them must be robust. This study confirms that the SWT is a feasible and reproducible test in elderly people and was completed by 88% of subjects with lung disease, including some with significant comorbidities such as osteoarthritis and previous stroke.
Airways diseases have a significant functional impact on older people,18 and the distance walked by the subjects with CAL was (on average) 74.3 m less than the controls (p<0.001), despite similar comorbidity levels. Although there was an association between the SWT and FEV1, it was weak and the distance walked could not be predicted from lung function test results, as has been described by others.3 Also reported in other studies, VC was more strongly related to exercise tolerance than FEV1.19 Associations with the NEADL index (r=0.51) and the LHS (r=0.43) were appropriate, which suggests that the SWT is a useful marker of disability in this age group. However, it should be noted that subjects were selected on the basis of relative independence in self-care at home (high Barthel scores) and most had reasonable NEADL and LHS scores. Connolly20 has noted that elderly patients with breathlessness tend to score relatively well on such functional scales, often being able to perform tasks such as washing and dressing, despite taking considerable lengths of time to do so. Nevertheless, caution must be applied when considering the appropriateness of the SWT in the most severely disabled patients.
A learning effect is noted in reproducibility studies of exercise tests in younger subjects,13 and a small one was detected in the current study. In the initial validation study of the SWT6 the 95% CI between walks 2 and 3 in 10 subjects was –21.9 to 17.9 m after one practice walk. In the current study the mean 2 week test-retest results between shuttle walks 1 and 3 (pre-bronchodilator) increased by only 6.0 m (with a 35.1 m coefficient of repeatability), although again only 10 subjects were tested. This is similar to a study of exercise in 15 elderly patients of mean age 76 years with chronic obstructive pulmonary disease (COPD)7 which found that overall mean values for the 6 minute walking test did not change when repeated on consecutive days, although a wide 95% CI (±60 m) was reported. Furthermore, the results of Knox et al13 suggest that walk tests repeated after weeks tend to show less “placebo effect” than when repeated after a few days.
It would be of interest to relate the current SWT results with those for the 6 minute walking distance test (6MWD), but published data with direct comparisons are minimal. Troosters et al21 have confirmed that the 6MWD test, although feasible, is a submaximal test in healthy elderly subjects. By contrast, the SWT may provide an assessment of maximal exercise capacity which is helpful in determining protocols for exercise training.6 For the 6MWD, increases in exercise capacity of 30–54 m are variously regarded as clinically important.22,23 We can currently conclude that an increase of 40 m (or four “shuttles”) for the SWT represents a statistically significant improvement in exercise capacity in older subjects, the clinical value of which would require further evaluation.
With regard to the effect of bronchodilators, it is noteworthy that in the CAL group the SWT improved by over 17 m (13.2%) following nebulised treatment compared with a non-significant increase of only 5.3% in the control group from a higher baseline level. Although all tests were supervised by one person (CAED), they were not performed in a blinded fashion and would have benefited from a placebo arm with repetition of the reversibility studies in individual subjects. Nevertheless, the use of a control group has allowed appropriate comparisons. There does appear to be a real increase in walking distance as a result of bronchodilator therapy which is supported by the observation that eight out of the 10 subjects with CAL whose exercise tolerance improved by four shuttles or more stopped because of breathlessness. Such an improvement in the SWT following bronchodilators has not been noted previously, and may reflect the lower walking distances and greater levels of disability in the current population. However, improvements in an individual's exercise tolerance did not significantly match improvement in FEV1. Walking distance increased post-bronchodilator by 40 m or more in only six out of 19 subjects whose FEV1 increased by at least 15%. Overall, the results are consistent with the study by Spence et al2 who examined the effect of oxitropium bromide on corridor walking in subjects with COPD (age unspecified). The authors detected a small but statistically significant increase in the mean distance walked (21 m), although they did not attempt to correlate this with significant changes in spirometry. The slightly stronger association between FEV1 and SWT post-bronchodilator raises the possibility that exercise tolerance would be better assessed formally after bronchodilator treatment. It may therefore also be possible that exercise training would be better performed following bronchodilators, but this would require further testing.
Thus, although a significant improvement in exercise tolerance was seen following bronchodilators for the CAL group as a whole, simple spirometric improvements do not translate into an increase in an individual's exercise tolerance, at least in the short term. However, over a longer period of observation (1 year) Teramoto et al24 found that exercise tolerance increased in patients with COPD treated with oxitropium bromide. In contrast, Grove et al25 failed to detect an improvement in 6MWD in patients with COPD chronically treated with salmeterol. Furthermore, Hay et al26 found that the increase in exercise capacity following oxitropium bromide was not related to the degree of bronchodilation. This may be explained by the fact that other volume related parameters (inspiratory capacity and residual volume) and airway resistance can change markedly even in the absence of flow related improvements.27,28 Exercise limitation in respiratory disease is likely to be due to a number of factors, including abnormal gas exchange, respiratory muscle weakness and deconditioning. It would therefore be unlikely that spirometric improvement following bronchodilators alone would lead to improved exercise capacity.
In conclusion, the incremental SWT appears to be feasible in most independently living elderly subjects, and overall changes in exercise capacity may be demonstrated following bronchodilators. This latter finding requires further confirmation in blinded placebo controlled conditions. Future research should focus on the responsiveness of the SWT to change following pulmonary rehabilitation in older subjects, and to determine the precise threshold for a clinically significant improvement.