Article Text

Abstract
BACKGROUND In patients with mild to moderate chronic obstructive pulmonary disease (COPD) the exercise induced increase in exhaled nitric oxide (eNO) parallels that observed in normal untrained subjects. There is no information on the effects of the level of exercise tolerance on eNO in these patients. The aim of this study was to evaluate the effect of a pulmonary rehabilitation programme including exercise training on eNO in patients with COPD.
METHODS In 14 consecutive male patients with stable COPD of mean (SD) age 64 (9) years and forced expiratory volume in one second (FEV1) 55 (14)% predicted, fractional eNO concentration (Feno), peak work rate (Wpeak) and oxygen uptake (V˙o 2peak) were assessed at baseline (T–1), at the end of a 1 month run in period (T0), and after an 8 week outpatient multidisciplinary pulmonary rehabilitation programme (T1) including cycloergometer training.
RESULTS Fenodid not significantly differ at T–1 and T0 (mean (SE) 4.3 (0.6) and 4.4 (0.6) ppb, respectively), whereas it rose significantly at T1 to 6.4 (0.7) ppb (p<0.02). Compared with T0, both Wpeak andV˙o 2 were significantly (p<0.05) increased at T1 (mean (SE) Wpeak from 89 (5.6) W to 109 (6.9) W);V˙o 2peak from 1.27 (0.1) l/min to 1.48 (0.1) l/min). A significant correlation was found between baseline FEV1 and the change in Feno following the rehabilitation programme (r=–0.71; p<0.05) and between changes in Feno and Wpeak from T0 to T1(r=0.60; p<0.05).
CONCLUSIONS Pulmonary rehabilitation in patients with mild to moderate COPD is associated with an increase in exhaled nitric oxide.
- chronic obstructive pulmonary disease
- exercise training
- exhaled nitric oxide
Statistics from Altmetric.com
Synthesis of nitric oxide (NO) in the respiratory system of animals and humans has been evaluated in vivo by measuring the concentration of NO in the exhaled air (eNO).1 Exhaled nitric oxide is increased in inflammatory lung diseases2 ,3 and reduced in primary pulmonary hypertension.4-7 Exhaled nitric oxide is also reduced6 in patients with severe chronic obstructive pulmonary disease (COPD)8 and it has been suggested as a marker of severity of disease.9 ,10
Impaired exercise tolerance is a common finding in patients with COPD. This feature is not a simple consequence of the loss of pulmonary function. Reduced exercise capacity shows only a weak relation to lung function impairment. Other factors such as peripheral and respiratory muscle weakness and deconditioning are now recognised as important contributors to reduced exercise tolerance.11 It has been shown that, in these patients, pulmonary rehabilitation programmes are likely to improve exercise capacity and health related quality of life (HRQL) if they also include exercise training.12
In healthy subjects eNO has been shown to increase markedly during exercise.13 Furthermore, in trained but not in sedentary healthy subjects it has been reported to be directly correlated with oxygen uptake (V˙o 2) during steady state exercise, suggesting that physical conditioning may induce an increase in eNO output during exercise.14 In patients with mild to moderate COPD an increase in eNO during exercise has been reported to parallel that observed in normal untrained subjects,15 but there is no information on the effects of the level of exercise tolerance on eNO in these patients with COPD. An effect on eNO (if any) might explain the observed benefits of pulmonary rehabilitation programmes including exercise training.16 The aim of this study was therefore to assess the effects on eNO of an 8 week outpatient rehabilitation programme including exercise training in patients with mild to moderate COPD.
Methods
Patients gave their informed consent to participate in the study which was approved by the ethical committee of Salvatore Maugeri Foundation IRCCS and was conducted according to the Declaration of Helsinki.
PATIENTS
Fourteen consecutive sedentary men with stable COPD referred from 1 January to 30 June 1999 for a multidisciplinary outpatient pulmonary rehabilitation programme described elsewhere17 were enrolled in the study. Diagnosis was made according to the American Thoracic Society (ATS) guidelines.8 All the patients were well known in our institution to which they were referred by attending physicians for periodic medical visits, lung function assessment, and eventually a pulmonary rehabilitation programme. All patients were ex-smokers and none had any history of atopy. At the time of the study all of them were clinically and physiologically stable. Patients who had been hospitalised or had suffered from an exacerbation of their disease within the preceding 4 weeks were excluded, as were patients with other organ failure, cancer, an unwillingness to cooperate, or inability to perform an exercise test. All the patients were receiving their regular treatment with inhaled anticholinergic drugs and rescue short term β2 agonists but not systemic or inhaled steroids. None of the patients was receiving long term oxygen. No change in medical treatment was made the week before and during the study period. Fifteen healthy sedentary subjects served as controls for eNO assessment.
STUDY DESIGN
The study was prospective and controlled, the patients serving as their own controls. Lung function was assessed only at baseline (T–1) as there is no evidence that pulmonary rehabilitation programmes affect it.12 Measurements of eNO and cycloergometry were performed at T–1, at the end of a 1 month run in period (T0), and after the completion of an 8 week outpatient pulmonary rehabilitation programme (T1). To further assess the clinical effects of the pulmonary rehabilitation programme, the 6 minute walking distance test (6MWD) and HRQL were measured before (T0) and after it (T1).
MEASUREMENTS
Lung function
Static and dynamic lung volumes were measured by constant volume body plethysmography (Medical Graphic Corp, St Paul, MN, USA) with the patient in the seated position according to the standard procedure. The predicted values according to Quanjer18 were used.
Exercise test
A symptom limited incremental exercise test was performed on an electrically braked cycloergometer (Ergometrics 800S, Sensormedics, Yorba Linda, CA, USA) using the standard 1 minute incremental cycle exercise protocol. Functional and metabolic data were determined at rest and during exercise by means of a computerised system (2900Z, Sensormedics, Yorba Linda, CA, USA). Breathing pattern and minute ventilation (V˙e), V˙o 2, and carbon dioxide production (V˙co 2) were continuously monitored as mean values of 20 second intervals. Electrocardiographic activity was monitored continuously and systemic arterial blood pressure was recorded every minute using a sphygmomanometer. After stabilisation and a 2 minute period of unloaded pedalling at 60 cycles per minute the load was increased by 10 Watts (W) each minute. The patients were strongly encouraged to cycle to the point of intolerable breathlessness, discomfort, or exhaustion until the maximal heart rate was achieved or an abnormal electrocardiogram noted (symptom limited exercise test). Non-invasive estimation of theV˙o 2 lactate threshold (AT) was calculated by the V-slope method.19 At rest and at 10 W intervals, patients were asked their perceived breathlessness and leg fatigue by pointing to a number or phrase on a 10 point modified Borg scale set in large type on a sheet in front of them.20
The 6MWD21 and the HRQL using the St George's Respiratory Questionnaire (SGRQ)22 were also assessed before and after the pulmonary rehabilitation programme (T0 and T1).
Exhaled NO
Patients were asked to abstain from food for at least 4 hours and from alcohol for at least 24 hours before the experiment. Exhaled NO measurement was performed online at rest by means of a chemiluminescence analyser (LR 2000 series, Logan Research, Rochester, UK) as previously described6 ,7 with a constant expiratory flow of more than 200 ml/s (range 250–300 ml/s). The analyser was calibrated daily using a certified NO mixture (108 ppb) in nitrogen (Messer Italia SpA, Collegno, Italy). The NO concentration in the ambient air was measured immediately before the study and, if it was higher than 30 ppb, patient testing was delayed. During the measurement of NO patients exhaled at constant expiratory pressure and flow up to a steady plateau by using a visual display of expiratory flow measured by the pressure and volume sensor in the analyser. The mean value of three reproducible readings (less than 5% intrapatient variability) of eNO plateau (Feno) was taken.23 The modalities of assessment were recorded and maintained constant for each patient for the different periods of evaluation (see study design).
Measurements were performed in the morning on two consecutive days: lung function, eNO and 6MWD in this order on day 1; exercise test and SGRQ on the next morning. The data were collected by physicians and technicians not involved in the study who were blind to eNO measurements.
Pulmonary rehabilitation programme
The pulmonary rehabilitation programme was a multidisciplinary programme17 consisting of three 3 hour sessions per week for 8–10 weeks including (1) supervised incremental exercise until patients achieved 30 minutes of continuous cycling at 50–70% of the maximal load achieved on an incremental cycloergometer exercise test carried out at admission24; (2) abdominal, upper and lower limb muscle activities lifting progressively increasing light weights (300–500 g), shoulder and full arm circling25; (3) patient and family specific education—for example, whether patients were focused on abstaining from smoking, environmental control, and on the management plans.
STATISTICAL ANALYSIS
All data are shown as mean (SD) or (SE) as specified. The time course of the results in patients was analysed using a one way ANOVA for repeated measures. A post hoc test with Bonferroni correction was then used when requested. Within subject reproducibility of NO measurements was analysed by ANOVA for repeated measures with Huynh-Feldt correction. The Wilcoxon matched paired test was used to test differences in non-parametric measures. Spearman analysis was then used to evaluate the linear correlation coefficient between Feno and functional parameters. A p value of <0.05 was considered to be statistically significant.
Results
Of 27 patients with COPD admitted to the pulmonary rehabilitation programme, 13 were excluded due to smoking (n=2), use of inhaled steroids (n=5), or severe associated diseases (n=6). Fourteen patients fulfilled the inclusion criteria and entered the study. Their demographic, anthropometric, and functional characteristics are shown in table 1. According to the ATS standards8 10 of the patients were in COPD stage I and four in stage II.
Mean (SD) demographic, anthropometric, and lung function data
Exercise tolerance
The time course of exercise performance as assessed by cycloergometry and 6MWD is shown in table 2. As expected, no differences were found in peak work rate, cardiopulmonary parameters, and sensations of dyspnoea and leg fatigue at the end of the run in period (T0). At the end of the pulmonary rehabilitation programme (T1) a significant improvement in exercise tolerance as assessed by peak cycloergometry work rate and 6MWD was observed. Sensations of dyspnoea and leg fatigue at the same work load were also significantly reduced.
Mean (SE) effects of rehabilitation on exercise response
Quality of life
The time course of HRQL as assessed by SGRQ (total and component scores) is shown in table 3. The total SGRQ score improved after the pulmonary rehabilitation programme, mainly due to an improvement in the Symptoms score.
Effects of rehabilitation on quality of life (SGRQ)
Exhaled NO
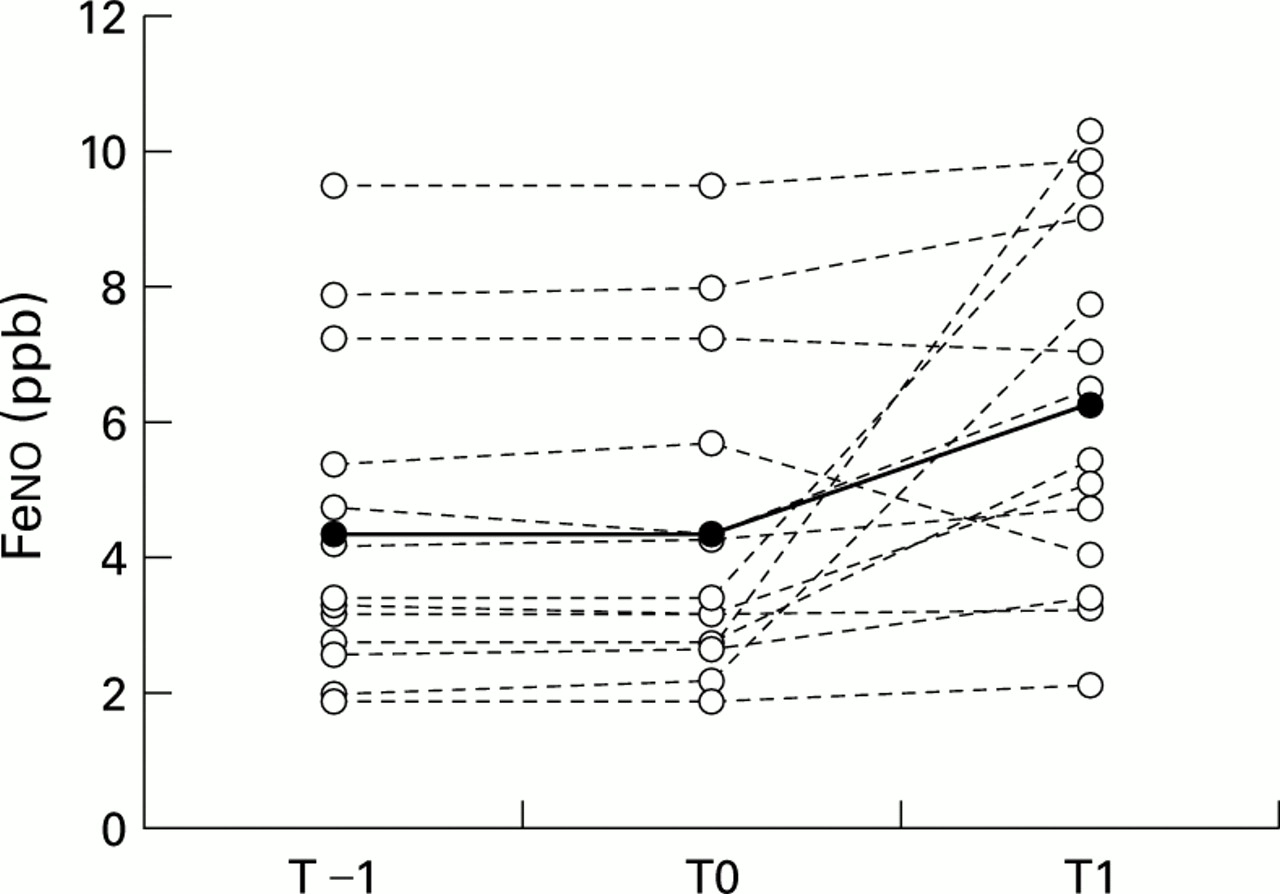
Individual and mean values of Feno measured over time are shown in fig 1. Despite the wide interpatient variability, mean and individual values of resting Feno assessed at T–1 and T0 were very similar (mean (SE) 4.3 (0.6) ppb and 4.4 (0.6) ppb, respectively; mean (SD) absolute change 0.05 (0.15) ppb (95% CI –0.03 to 0.14)) and did not differ significantly from those obtained in healthy controls (4.3 (0.4) ppb). In contrast, all but two showed individual increases in Feno following the pulmonary rehabilitation programme (T1). As a result, a significant mean increase in Feno was seen following the pulmonary rehabilitation programme to 6.4 (0.7) ppb (mean (SD) absolute change 1.97 (2.69) ppb (95% CI 0.41 to 3.53)).

Individual (dotted line) and mean values (continuous line) of Feno measured 1 month (T–1), immediately before (T0) and after (T1) the pulmonary rehabilitation programme. Post hoc for p<0.01 T1 v T0 and T–1.
Figure 2 shows the relationship between changes in exercise tolerance and in Feno before and after the pulmonary rehabilitation programme. A significant correlation (r=0.60) was found.
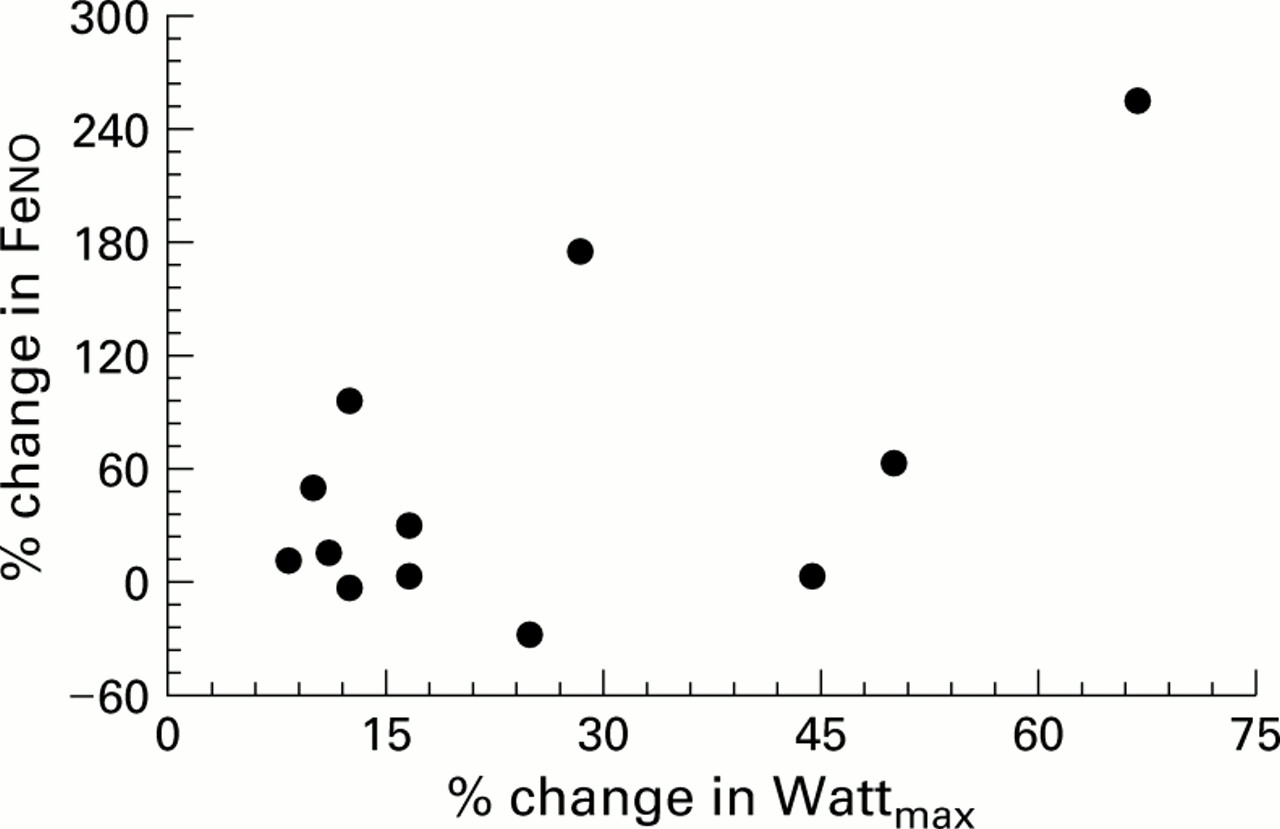
Correlation between changes in Feno and in maximal work load following pulmonary rehabilitation programme; r=0.60; p<0.05.
There was an inverse relationship (r=–0.71) between the increase in Feno at T1 and baseline FEV1 (fig 3). No significant relationship was observed between changes in Feno and changes in 6MWD or SGRQ.

{kind=link}
{kind=link}
{kind=link}
Correlation between change in Fenoelicited by the pulmonary rehabilitation programme and severity of airflow obstruction at admission; r=–0.71; p<0.005.
Discussion
This study is the first to show that, in patients with mild to moderate COPD, improvement in exercise tolerance following a multidisciplinary pulmonary rehabilitation programme including lower limb training may be associated with an increase in resting eNO.
The baseline mean values of Feno (T–1 and T0) were lower than those obtained in previous studies in our laboratory in patients with COPD of similar severity.6 ,7 The discrepancy can be explained by the fact that in this study we used the single breath manoeuvre with a constant expiratory flow of more than 200 ml/s (range 250–300), whereas in the previous studies a lower expiratory flow was used. Indeed, an inverse relationship between expiratory flow and eNO concentration has been described.26 The measurements at T–1 and T0 showed good reproducibility and, as in a previous study,6 the mean Feno values observed in our patients with mild to moderate COPD both at T–1 and T0 did not differ from those recorded in healthy controls.
This study is the first to show an effect of a pulmonary rehabilitation programme on eNO in patients with COPD. Improvement in exercise tolerance was associated with an increase in resting eNO. In a previous study15 we observed that eNO increased in patients with mild to moderate COPD during maximal exercise, although to a lower extent than in normal age related sedentary controls. In the previous study most of the increase in eNO was related to the increase inV˙e. In the present study V˙e at rest did not change over time, therefore we cannot ascribe the changes in eNO following the pulmonary rehabilitation programme to changes inV˙e.
Compared with untrained normal subjects, studies in athletes reported a greater increase in eNO output during strenuous exercise.14 In contrast, other authors have reported that, in normal subjects during exercise, eNO was mainly related to the magnitude of aerobic metabolism and was independent of the level of physical training.27 In addition, it has also been shown that resting levels of plasma nitrate (a stable soluble end product of NO) are significantly higher in athletes than in sedentary controls and correlate with the peak work rate.28 This may suggest an association between physical fitness and formation of NO with resulting beneficial effects of training on cardiovascular health.28
The exercise related increase in eNO in normal subjects has been postulated as deriving mainly from the airway,29 perhaps through an upregulation of NO synthase by increased vascular shear stress. Although a vascular origin of eNO has been suggested in acute exercise,30 Sartori et al 31 have recently demonstrated in healthy humans that pulmonary eNO is mostly of epithelial rather than endothelial origin, and does not provide a marker for vascular or endothelial function.
This study has shown a significant correlation between changes in eNO and in peak work load following a pulmonary rehabilitation programme in patients with stable COPD. An increase in eNO was recorded after the pulmonary rehabilitation programme in almost all the patients studied (12 out of 14). The two patients whose NO value decreased or remained unchanged were unable to reach the optimal plateau according to the exercise training protocol adopted (see Methods), starting below 50% of the initial work load because of severe dyspnoea. Interestingly, the change in eNO in our COPD patients after the pulmonary rehabilitation programme was inversely related to the degree of baseline airway obstruction (fig 3). Only the most severe COPD patients (ATS disease stage III) and those with an associated cor pulmonale are known to produce lower levels of eNO,6 ,7 probably due to reduced expression and activity of constitutive NO synthase. Since the patients in the study were in ATS disease stages I or II, we did expect similar production of NO from the airway both at rest and during effort. Nevertheless, suggested positive effects on vasodilation,32 bronchodilation,33 ,34 and ventilation-perfusion distribution35 resulting from enhanced NO activity might have favoured the most obstructed patients in the study.
In contrast with the incremental cycloergometer exercise test, no significant relationship was observed between changes in Feno and in 6MWD after the pulmonary rehabilitation programme. This may reflect differences between modalities of the exercise test, the 6MWD reflecting endurance capacity more than the incremental test.36 The lack of a relationship between changes in eNO and in HRQL is not surprising and probably reflects the comprehensive nature of the pulmonary rehabilitation programme and the fact that HRQL depends on more than just exercise ability.17
The most important limitation of this study is the lack of a randomised protocol with a control group. However, due to the prospective design and the lack of change in eNO during the run in period, we are confident that the pulmonary rehabilitation programme was the major determinant for the observed changes in eNO. Indeed, both eNO and exercise tolerance increased after the pulmonary rehabilitation programme, but not during the run in period, with at least 36% of the change in eNO being accounted for by the increase in exercise tolerance (fig 2).
In conclusion, with the limitation of the lack of a randomised control population, our study suggests that an increase in exercise tolerance related to a pulmonary rehabilitation programme may be associated with an increase in eNO in patients with mild to moderate COPD. eNO might, at least theoretically, be a useful marker for assessing the pathophysiological adaptation to training in patients with COPD. Further prospective randomised controlled studies are needed to better define this role.