Article Text

Abstract
BACKGROUND Clearance of inhaled technetium 99m-labelled diethylenetriamine penta-acetic acid (99mTc-DTPA) from the lungs is a potential indicator of disease progression in patients with idiopathic pulmonary fibrosis (IPF).
METHODS We prospectively analysed the usefulness of this technique for predicting survival in 106 non-smoking patients with usual interstitial pneumonia (UIP) pattern IPF diagnosed by high resolution CT (HRCT) scanning or histological examination (M/F 65/41, mean (SD) age 61 (11) years). DTPA clearance was analysed according to both mono-exponential and bi-exponential models. Half times for the fast (t 0.5 F) and slow (t 0.5 S) components of clearance, the percentage contribution of the fast component (f F ), and half time for mono-exponential approximation to the early part of the clearance curve (t 0.5) were calculated.
RESULTS The patients had substantially faster t 0.5(mean 23.9 (9.6) minutes) than normal values (>45 minutes). Thirty seven patients (35%) died during follow up (median 15 months). Univariate Cox regression analysis identified significant predictors of survival as age, forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), total lung capacity (TLC), % predicted TLC, carbon monoxide transfer factor (Tlco), % predicted Tlco, arterial oxygen tension (Pao 2), oxygen saturation,t 0.5 F, and HRCT fibrosis score. Multiple stepwise Cox regression analysis identifiedt 0.5 F(p=0.03, hazard ratio 0.747, 95% CI 0.578 to 0.964), % predicted TLC (p=0.02, hazard ratio 0.976, 95% CI 0.956 to 0.995), % predicted Tlco (p=0.003, hazard ratio 0.960, 95% CI 0.935 to 0.986), and age (p=0.003, hazard ratio 1.062, 95% CI 1.021 to 1.104) as independent predictors of survival.
CONCLUSION These data suggest that 99mTc-DTPA clearancet 0.5 Fmeasurement may predict survival in patients with UIP pattern IPF.
- idiopathic pulmonary fibrosis
- cryptogenic fibrosing alveolitis
- 99mTc-DTPA clearance
- survival
Statistics from Altmetric.com
Idiopathic pulmonary fibrosis (IPF), cryptogenic fibrosing alveolitis, is a progressive, fatal, and increasingly common disease.1 ,2 Recent revision of the histological classification of IPF has emphasised the clinical importance of the different histological patterns of usual interstitial pneumonia (UIP), desquamative interstitial pneumonia (DIP), and non-specific interstitial pneumonia/fibrosis (NSIP).3 The critical differences between these histological subcategories lie in the potential responsiveness to steroids and in survival.4UIP pattern IPF has a poor prognosis with a median survival of 2.8 years, and 65% of patients with IPF fall in this group.4
Predicting survival in IPF is difficult. To date, pulmonary function, high resolution CT (HRCT) scans, and response to treatment have been used as surrogates for estimating survival.5-8
Clearance of inhaled technetium 99m-labelled diethylenetriamine penta-acetic acid (99mTc-DTPA) is an index of lung epithelial permeability.9 Increased DTPA clearance may be a sensitive marker of inflammation10 and normal clearance certifies absence of inflammation.11 It has been used in the repertoire of investigations in a number of diffuse parenchymal lung diseases12-16 and could potentially be used as a predictor for disease progression in UIP. A previous study of DTPA in a heterogeneous group of patients with IPF showed that normal DTPA clearance selects patients with a favourable prognosis.15
The objective of this study was to evaluate the potential of99mTc-DTPA scanning to predict survival in patients with UIP pattern IPF. Our study differs from earlier studies in that we have resolved the clearance of 99mTc-DTPA into its fast and slow components and have analysed the prognostic significance of each component of clearance independently. In addition, we wished to determine whether DTPA clearance correlated with pulmonary function, HRCT scores, and the cellular characteristics of bronchoalveolar lavage (BAL) fluid.
Methods
PATIENT SELECTION CRITERIA
Patients with either histological evidence of UIP pattern IPF or an HRCT scan highly suggestive of UIP pattern IPF were included in the study. Patients were excluded if any of the following were present: (1) collagen vascular disease, allergic alveolitis or exposure to organic dusts, (2) co-existing heart failure, active pulmonary infection, or pneumothorax causing the functional abnormalities at presentation, (3) current smoking (during the 6 months prior to the measurement of DTPA clearance). Patients were secondarily excluded on the following criteria: (1) a subsequent pulmonary tissue diagnosis other than UIP pattern IPF, (2) an objective response to corticosteroids alone, and (3) those who subsequently underwent lung transplantation.
SURGICAL LUNG BIOPSIES
Surgical lung biopsy specimens were obtained either through a thoracotomy incision or by video assisted thoracoscopic surgery. The site of the biopsy was directed by HRCT scanning.
Definition of UIP pattern IPF by histological criteria
A diagnosis of UIP was made if the following histopathological features were present3:
- (a)
- a variegate picture of interstitial fibrosis, inflammation and normal tissue;
- (b)
- a tendency for fibrosis to occur in a subpleural and peripheral distribution;
- (c)
- exclusion of features indicating another aetiology (e.g. asbestos bodies, granulomas).
HRCT SCANNING
All included patients underwent HRCT scanning of the chest using a Picker PQ scanner (Picker International). The HRCT scans consisted of 1.5 mm thick slices acquired at 10 mm increments through the thorax reconstructed with a high spatial frequency algorithm. Scans were performed at the end of inspiration with the patients in the supine position and no intravenous contrast was given. The HRCT scans were reviewed independently by two pulmonary radiologists (MSG and AWH) who were unaware of the clinical and functional findings.
Definition of UIP pattern IPF by HRCT criteria
A diagnosis of UIP was made if the following HRCT features were present17 ,18:
- (a)
- reticular pattern of intralobular interstitial thickening demonstrating a peripheral, subpleural, and basal predominance with irregular pleuroparenchymal interfaces;
- (b)
- may show areas of honeycombing and traction bronchiectasis;
- (c)
- ground glass opacification may be present but the reticular pattern predominates.
The same radiologists scored each lobe of the lung for the extent of ground glass opacity (HRCT ground glass score) and reticular opacities and honeycombing (HRCT fibrosis score) on a scale of 0–5 based on the method described by Kazerooni et al.19 The mean value for all lobes was incorporated into a ground glass and fibrotic score for each patient and scores were then averaged for the two readers.
PULMONARY PHYSIOLOGY
Pulmonary function tests were performed at the start of the study at the same visit as the radiological examination. Spirometric tests (Sensormedics Vmax 22, California, USA), plethysmographic lung volumes (Sensormedics 6200 Plethysmograph) and carbon monoxide lung transfer factor (Tlco) (PK Morgan, Rainham, UK) were measured in all patients. Alveolar volume (Va) was measured by a single breath helium dilution method and transfer coefficient (Kco) was calculated from Tlco/Va. Tlco values were corrected for the haemoglobin concentration of the patient. Values were expressed as percentages of the predicted values calculated according to sex, weight, and age.20 All but four patients had blood gas analyses at rest while breathing room air using the end capillary (earlobe) technique (ABL330 Acid-Base Laboratory, Copenhagen, Denmark).
99mTC-DTPA SCANNING
An aerosol of 99mTc-DTPA was produced using pressurised air. The jet nebuliser produces an aerosol with a median aerodynamic diameter of less than 1 μm. Patients were seated in front of a gamma camera and inhaled the aerosol during normal tidal breathing through a mouthpiece with a one way valve and noseclip in place. Administration continued for up to 5 minutes or until a suitable count rate was detected over the lungs. Patients were then imaged from the posterior side using a gamma camera with general purpose collimator. Images were acquired for 60 minutes at an image resolution of 64 × 64 using a frame duration of 20 seconds for at least the first 15 minutes. Regions of interest were then drawn around both lungs and a region was defined either between the kidneys or in the shoulders to enable suitable subtraction of background activity. Solute clearance was calculated from the rates of radionuclide disappearance from the lungs. Clearance rates obtained from each individual refer to both mono-exponential and bi-exponential clearance analyses. Curve stripping was used to separate the two components of the bi-exponential disappearance curves. Briefly, the slow component can be identified from the later section of the 60 minute curve, usually taking the last 30 minutes. The contribution of the slow component to the early part of the curve can then be calculated and subtracted out, isolating the fast component.
Four DTPA variables were analysed. These were half times for (1) the fast (t 0.5 F) and (2) the slow (t 0.5 S) components of the bi-exponential curve, (3) the fraction of the tracer cleared by the fast (f F ) component, and (4) the half time from a mono-exponential approximation to the early part of the curve (t 0.5).
The clearance half timest 0.5 Fandt 0.5 Swere defined as the time to achieve a 50% decrease in the fast and slow components of the curve, respectively.f F andfS were defined as the respective fractions of tracer cleared into the “fast” or “slow” components (fig 1). The half time from a mono-exponential approximation to the first 15 minutes of the curve was also calculated. The normal half time value for this parameter is more than 45 minutes.21

Schematic representation of the two component system. (A) DTPA is deposited onto normal and abnormal tissues and cleared by slow and fast processes. (B) Fractional depositions and speeds of the processes can be calculated from time variation of lung activity.
BRONCHOALVEOLAR LAVAGE
Bronchoalveolar lavage was performed by a standard method. In brief, patients were premedicated with atropine and midazolam and the upper airway was anaesthetised with 4% lidocaine (lignocaine). Two aliquots of 50 ml warm sterile saline were instilled into the middle lobe and then recovered by gentle suction. The lavage was filtered through two layers of sterile gauze to remove mucus. Preparations of the cell suspensions were made in a cytocentrifuge (Cytospin 3; Shandon Scientific Ltd, Astmoor, UK) and cytospin slides of BAL cells were stained by the Papanicolaou method for cell differentiation. At least 200 cells were counted.
FOLLOW UP
The date of the DTPA study was established as the baseline from which survival was measured. Follow up concluded with the patient's death or last presentation. Survival was confirmed from the hospital notes and by contacting the patient's primary care physician.
STATISTICAL ANALYSIS
The statistical analyses were performed using the SPSS/PC (version 9.0, SPSS Inc, USA) software package. Values are expressed as means (SD) and a statistical significance level of 0.05 was used. Cox proportional hazards regression analysis was used throughout.
The characteristics of the patients who underwent open lung biopsy were compared with those who had not, using the Mann-Whitney U test. Kaplan-Meier survival curves were derived for patients in the two groups and comparison was made using the log rank test statistic.
Univariate Cox regression analysis was completed to identify significant variables predicting survival status. Variables which were significant by univariate Cox regression analysis were taken as potential predictors of survival and were used as covariates in the stepwise multivariate Cox regression analysis to identify independent predictors of survival. Those variables found to be independent predictors of survival by the multivariate analysis were used to perform stratified Cox regression survival function analysis. Each variable was further stratified into quartiles and the survival of the patients estimated. The quartile stratification was performed for age, % predicted Tlco, % predicted TLC, andt 0.5 F. The age quartiles included those patients aged <50 years, 50–59 years, 60–69 years, and >70 years; the % predicted Tlcoquartiles were >55%, 45–54%, 35–44%, and <35%; the %predicted TLC quartiles were >90%, 75–89%, 60–75%, and <60%; and thet 0.5 Fquartiles were >6.5 minutes, 5.5–6.4 minutes, 4.5–5.4 minutes, and <4.5 minutes. The results were summarised as hazard ratios which represent the relative risk of dying as a result of a specific characteristic during the entire period of observation.
The four measures of DTPA clearance were correlated against individual physiological, radiological, and BAL parameters by Pearson's correlation coefficient (two tailed).
Results
PATIENT SELECTION
One hundred and thirty one patients were potential candidates for participation in the study (fig 2). Patients were secondarily excluded from the study if they had a subsequent tissue diagnosis other than UIP and/or responded to steroids (n=14) or underwent lung transplantation (n=11). A total of 106 patients therefore formed the study group (65 men, mean (SD) age 61 (11) years). The diagnosis of UIP pattern IPF was established by surgical (open or thoracoscopic) lung biopsy in 32 patients (30%). Seven patients (7%) had a diagnosis based on a transbronchial biopsy and HRCT scan. For six patients (6%) the diagnosis based on HRCT scanning was verified at necropsy. In 61 patients (57%) the diagnosis of UIP was based on the HRCT scan alone.
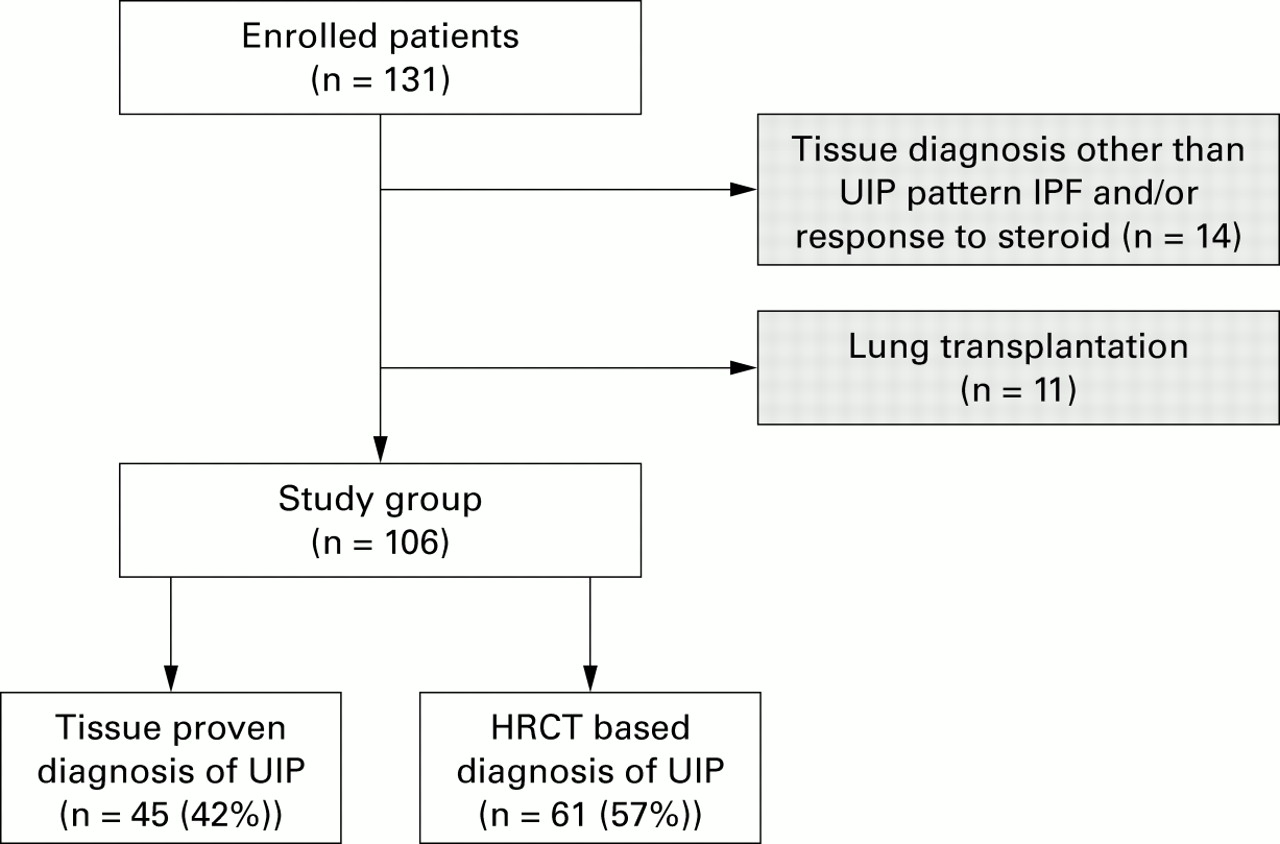
Patient flow through the enrolment process to make up the study group.
Thirty seven of the patients had never smoked while the remaining 69 had ceased smoking at least 6 months before entry into the study. No patient was lost to follow up. The median duration of follow up was 15 months. Thirty seven patients (35%) died of progressive lung disease during the follow up period (32 from respiratory failure, three from infection, and two from lung cancer). The median survival was 47 months.
Table 1 shows the characteristics of the patients including pulmonary function, BAL cell differential counts, and HRCT scores. Although HRCT scanning was performed for diagnostic purposes in all patients, the scan was available and suitable for fibrosis and ground glass scoring in 71 patients. DTPA scanning variables are shown in table 2.
Patient characteristics (n=106)
99mTc-DTPA clearance rates of study subjects
OPEN LUNG BIOPSIES
Patients who had an open lung biopsy were significantly younger than the other patients (mean 55.6 v 63.3 years, p<0.001) with better Tlco (4.47v 3.76 mmol/kPa/min, p=0.044), Kco (1.23 v 1.09 mmol/kPa/min/l, p=0.039), and Pao 2 (9.44v 8.47 kPa, p=0.006); the difference in the Kaplan-Meier survival did not reach statistical significance (log rank p=0.24).
FACTORS ASSOCIATED WITH SURVIVAL BY UNIVARIATE COX REGRESSION ANALYSIS
Age, FEV1, FVC, TLC, Tlco, Pao 2, oxygen saturation, HRCT fibrosis score,t 0.5 F, % predicted TLC, and % predicted Tlco were statistically significant predictors of survival (table 3).
Variables significantly and not significantly associated with survival by univariate Cox regression analysis
BIVARIATE CORRELATIONS BETWEEN DTPA VARIABLES AND OTHER PARAMETERS
Although several correlations between the four DTPA variables and various measures of pulmonary function, blood gas analysis, HRCT scores, and BAL fluid differential cell counts reached statistical significance (p<0.05), the degree of correlation assessed by ther value was nowhere more than weak. Those correlations which reached significant p values are shown in table4.
Correlations between DPTA variables and other parameters
STEPWISE MULTIVARIATE COX REGRESSION ANALYSIS
By multivariate stepwise regression analysis, age (p=0.003), % predicted TLC (p=0.02), % predicted Tlco (p=0.003), andt 0.5 F(p=0.03) were found to be independent predictors of survival (table 5). The inclusion of other DTPA scanning parameters, pulmonary function, HRCT scores, and BAL fluid differential cell counts did not improve the Cox regression model.
Effect of independent predictors on survival determined by multiple stepwise regression analysis
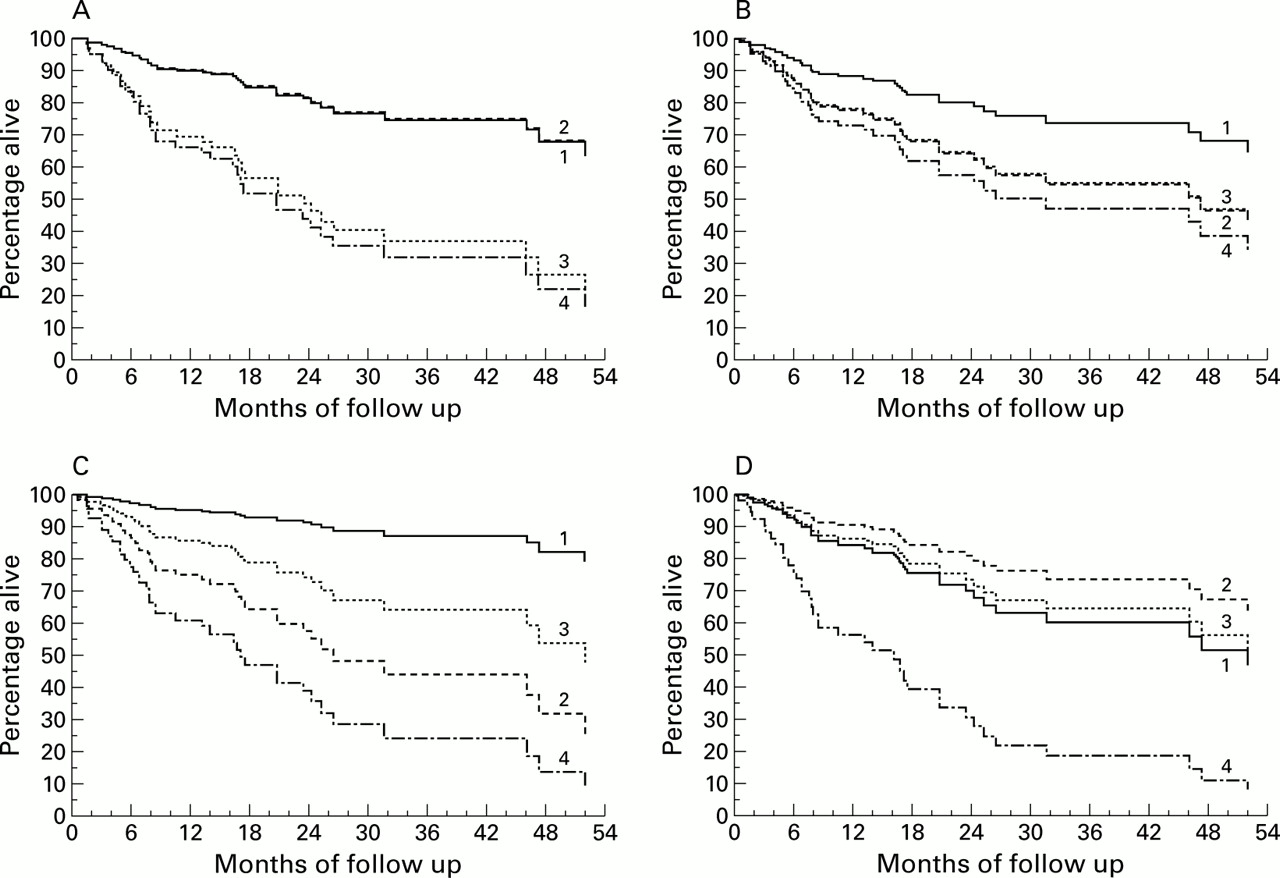
Multivariate Cox regression analysis yielded the hazard ratios shown in table 5. The hazard of death increases by 6% (95% CI 2 to 10) for every year of patient age, by 2% (95% CI 1 to 4) for every 1% decrease in % predicted TLC, by 4% (95% CI 1 to 6) for every 1% decrease in % predicted Tlco, and by 25% (95% CI 4 to 42) for every 1 minute decrease int 0.5 F(table 5). The effect of these variables on survival is plotted by quartiles in fig 3.
{kind=link}
{kind=link}
{kind=link}
Survival analysis grouped by (A) Tlcopercentage predicted quartiles, (B) t0.5F quartiles, (C) age quartiles, and (D) TLC percentage predicted quartiles. (A) 1 = patients with Tlco >55% predicted (n=30), 2 = Tlco 45–54.9% predicted (n=23), 3 = Tlco 35–44.9% predicted (n=29), 4 = Tlco <35% predicted (n=22). (B) 1 = patients with t0.5F >6.5 minutes (n=26), 2 = t0.5F 5.5–6.4 minutes (n=22), 3 = t0.5F 4.5–5.4 minutes (n=30), 4 = t0.5F <4.5 minutes (n=25). (C) 1 = patients <50 years (n=15), 2 = age 50–59 years (n=34), 3 = age 60–69 years (n=36), 4 = age >70 years (n=21). (D) 1 = patients with TLC >90% predicted (n=26), 2 = TLC 75–89.9% predicted (n=23), 3 = TLC 60–74.9% predicted (n=24), 4 = TLC <60% predicted (n=32).
Discussion
This study was conducted to assess the ability of DTPA scanning to predict survival in patients with UIP pattern IPF. The data presented demonstrate that thet 0.5 Fcomponent of DTPA clearance is a significant independent predictor for survival in the stepwise multiple regression analysis, augmenting the prognostic information given by age, % predicted TLC, and % predicted Tlco. The p values in table 5 indicate that age and % predicted Tlco are the most important predictors of survival, followed by % predicted TLC andt 0.5 F. Improved prediction of survival may be particularly important in the context of referral for lung transplantation.
In this study only patients with a secure diagnosis of UIP were included. This demanded either an open lung biopsy or an HRCT scan in all cases, and 30% of patients were subject to histological confirmation of the diagnosis of UIP by open lung biopsy. This is higher than the standard practice in the UK where open lung biopsy rates of 8% are usual.22 Inclusion only of patients with histological confirmation of disease may be ideal. However, such a strategy would result in a selection bias towards patients who are sufficiently well to undergo biopsy. Inclusion of those patients in whom the diagnosis has been secured by HRCT scanning should result in a more representative spectrum of cases. Several studies have shown that HRCT findings can predict histological patterns.17 ,19 ,23 ,24 Furthermore, our mean fibrosis score of 2.0 closely mirrors that of Kazerooni et al 19 who found a strong correlation between the CT fibrosis score and the pathology fibrosis score.
In our study the median survival was 47 months. Published median survival figures vary from 2.9 years for a population based cohort study to 5 years in the selected subgroups which reach tertiary referral centres.2 Our population falls into the latter category.
In UIP pattern IPF non-invasive tests of high sensitivity and specificity are required by clinicians to distinguish cases which will show progressive disease from those which will behave in an indolent manner. Wells et al 15 were the first to report the potential role of DTPA scanning for predicting the clinical course of fibrosing alveolitis, although their study included a majority of patients with systemic sclerosis. Their study showed that normal clearance predicted stable lung function; survival was not analysed. In contrast, this study is restricted to UIP pattern IPF. In the present study the increased mono-exponential rate of99mTc-DTPA lung clearance—that is, reducedt 0.5—in the entire patient group is in keeping with previous reports for IPF.10 ,15However, our study differs from previous studies in that it focuses on the resolution of the DTPA clearance into fast and slow components, allowing the demonstration that the fast component is a prognostic indicator in UIP pattern IPF (table 3).
It has been shown that, with a median aerodynamic diameter of 0.8 μm or less, deposition occurs primarily beyond the ciliated epithelium—that is, on the respiratory bronchioles and alveoli.26 In healthy non-smokers pulmonary clearance of99mTc-DTPA follows a mono-exponential course with a half time of 60–70 minutes. In healthy smokers the clearance may be resolved mathematically into two exponential components.25This bi-exponential course has been demonstrated in several groups including patients with ARDS, HIV infection, hyaline membrane disease, and patients without oedema after exposure to coal dust and crack cocaine.11 Bi-exponential clearance is always abnormal.26 The published half times of the bi-exponential components are typically of the order of 13 and 83 minutes, respectively. The physical basis of the bi-exponential clearance is uncertain, but it has been suggested that the fast clearance occurs in areas of damaged lung while the slow (normal) clearance occurs in areas of normal lung (fig 1).10 We speculate that the rapid clearance may occur across the bare basement membrane, denuded of epithelium, which has been demonstrated in ultrastructural studies of IPF.27 If this is the case, then the proportion of the clearance that occurs by the fast component (f F ) may be a measure of the proportion of the lung parenchyma which is diseased, and the rapidity of clearance by the fast component may be a measure of the severity of damage to the abnormal areas of the lung.
In previous 99mTc-DTPA scanning studies in patients with IPF the pulmonary clearance of aerosol has usually been analysed as a mono-exponential approximation to the clearance curve, as applied by Wells et al.15 ,28 ,29 These studies have typically been based on the rate of clearance in the first 7–15 minutes and thus the half times were strongly influenced by the fast component of the clearance. These studies have been performed in relatively small groups of patients compared with our patient population.
Some central airway deposition of the aerosol was observed in a significant minority of patients despite the small size of the aerosol particles used. This effect is frequently seen in patients with poor lung function due to airflow obstruction or emphysema, bronchial asthma, chronic bronchitis, and other conditions, as well as technical difficulties and variations between nebulisers. Additional analysis of the images from eight patients with marked central deposition was carried out using information from both whole lung and peripheral lung areas, but a paired t test showed no significant difference between thet 0.5 Fvalues calculated for the two areas. Similarly, in a further group of eight patients without central deposition there was no significant difference betweent 0.5 Fvalues for the whole lung and peripheral lung areas.
Hence, whole lung information was used in all the analysis presented to minimise the effects of statistical noise in the curve processing. Mucociliary clearance from the central airways does not appear to play a significant role in the measurement oft 0.5 Fin this study group.
We found no correlation between aerosol clearance and pulmonary function parameters (table 4), in agreement with the findings of previous studies.28 ,30 Similarly, only a weak correlation between DTPA clearance and % predicted Tlco was found in patients with sarcoidosis and scleroderma.31 ,32 The consistent absence of a correlation may be because the impairment of pulmonary function parameters is a result of the maldistribution of ventilation and perfusion or loss of surface area, while the increased rate of DTPA clearance is caused by increased junctional permeability in the alveolar capillary membranes.
Theoretically, the major barrier to clearance of DTPA across the alveolar-capillary barrier is at the alveolar epithelium. In lung fibrosis it is likely that the greatest contribution to clearance within the first minutes will be from fragmented interepithelial junctions, as suggested in previous studies.10 The lower values oft 0.5 Fobserved in patients who die may therefore be attributable to changes in epithelial morphology and severe damage of the lung tissue accompanying more inflammatory cell accumulation as well as fibrosis and destruction.
In conclusion, in UIP pattern IPF a biphasic pattern of clearance of DTPA from the lungs is seen. A reduced half time for the rapid component of clearance is an independent predictor of reduced survival. This technique complements other prognostic indicators such as age, % predicted TLC and Tlco and gives additional information as to expected survival. Our preliminary conclusion is that this simple and readily available technique could usefully be incorporated into clinical practice.
Acknowledgments
The authors acknowledge the Greater Manchester Lung Fibrosis Consortium for contributing patients, and Mrs Julie Morris and Mr Stephen Francis for advice on the statistical analysis of the data.
Members of the Greater Manchester Pulmonary Fibrosis Consortium: Dr G Archer, Stepping Hill Hospital, Stockport; Dr T Baker, Maelor Hospital, Wrexham; Dr PV Barber, Wythenshawe Hospital, Manchester; Dr B Bradley, Bolton General Hospital, Bolton; Dr Burton, Royal Preston Hospital, Preston; Dr KB Carroll, Wythenshawe Hospital, Manchester; Dr M Chopra, Tameside Hospital, Manchester; Dr J Earis, Fazakerley Hospital, Liverpool; Dr M Finnegan, Bury General Hospital, Bury; Dr J Finnerty, Countess of Chester Hospital, Chester; Dr D Graham, Whiston Hospital, Merseyside; Dr S Hanley, North Manchester General Hospital, Manchester; Dr C Hardy, Manchester Royal Infirmary, Manchester; Dr AM Hilton, Wythenshawe Hospital, Manchester; Dr K Jones, Bolton General Hospital, Bolton; Dr I Keeping, County of Chester Hospital, Chester; Dr S Madi, Chorley Hospital, Chorley; Dr J Miles, North Manchester General Hospital, Manchester; Dr R O'Driscoll, Hope Hospital, Manchester; Dr C Payne, Tameside Hospital, Manchester; Professor CAC Pickering, Wythenshawe Hospital, Manchester; Dr AK Webb, Wythenshawe Hospital, Manchester; Dr J Williams, Halton General Hospital, Runcorn; Dr R Wolstenholme, Royal Albert and Edward Infirmary, Wigan; Professor AA Woodcock, Wythenshawe Hospital, Manchester.