Article Text

Abstract
A case of relapsing polychondritis presenting as tracheomalacia is reported in which an unusual low pitched sound was heard at the mouth and over the chest wall during expiration. The sound was associated with expiratory airflow limitation and oscillation on the flow trace of approximately 50 Hz. Spectral analysis of the sound showed it to have the characteristics of sounds produced by flutter in flow limited flexible tubes. These observations suggest that the sound was produced by airflow induced flutter in the trachea and main airways and is further evidence in support of the dynamic flutter theory of wheeze production.
- relapsing polychondritis
- tracheomalacia
- wheeze
- spectral analysis
Statistics from Altmetric.com
Relapsing polychondritis is an uncommon condition in which recurrent episodes of inflammation lead to destruction of cartilage, most commonly in the ear, nose, joints and the respiratory tract.1 When the respiratory tract is affected the loss of cartilaginous support in the trachea and main bronchi (tracheomalacia) results in airflow obstruction, failure to expectorate sputum, and recurrent infections. We report such a case which was associated with the production of an unusual expiratory sound. The spectral analysis of this sound and its relationship to airflow is presented. Possible mechanisms of sound production are discussed and related to the current theories of dynamic flutter and wheeze in floppy tubes.
Case report
A 55 year old woman who was a life long non-smoker with no history of previous chest disease was admitted to hospital with a two month history of dyspnoea and wheeze. On examination she was obese, tachypnoeic, and a low pitched expiratory “wheezing” sound was heard at the mouth. On auscultation the sound occurred on deep and forced breathing but not with tidal breathing. It was present in all areas but was loudest over the upper anterior chest wall. Investigations revealed airflow obstruction (FEV1 0.9 l, FVC 2.0 l, FEV1 35% of predicted normal), a normal chest radiograph, and a mild eosinophilia. A diagnosis of late onset asthma was made and treatment with inhaled β agonists, inhaled corticosteroids, and oral aminophylline was started. She did not respond to this medication and further investigations were undertaken.
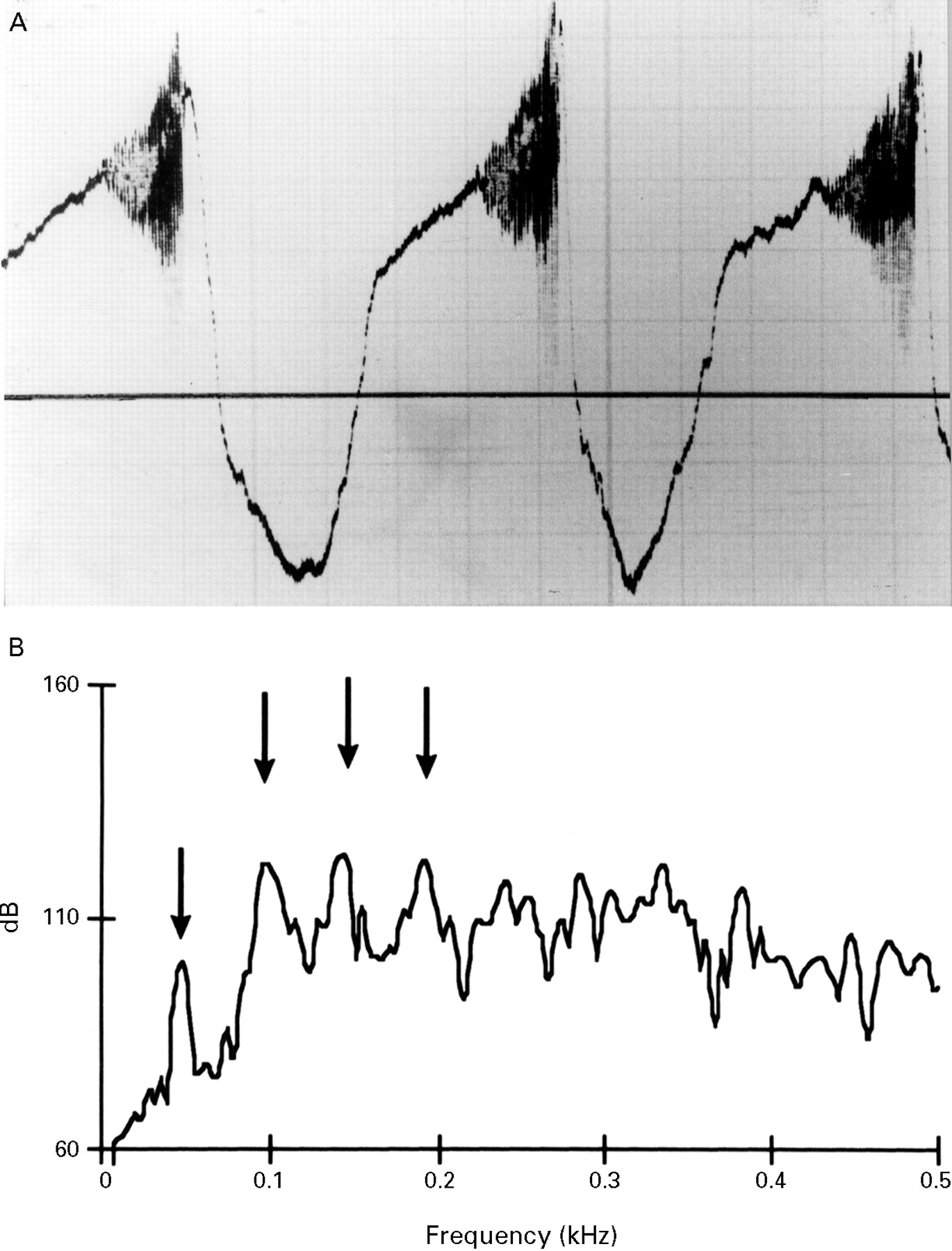
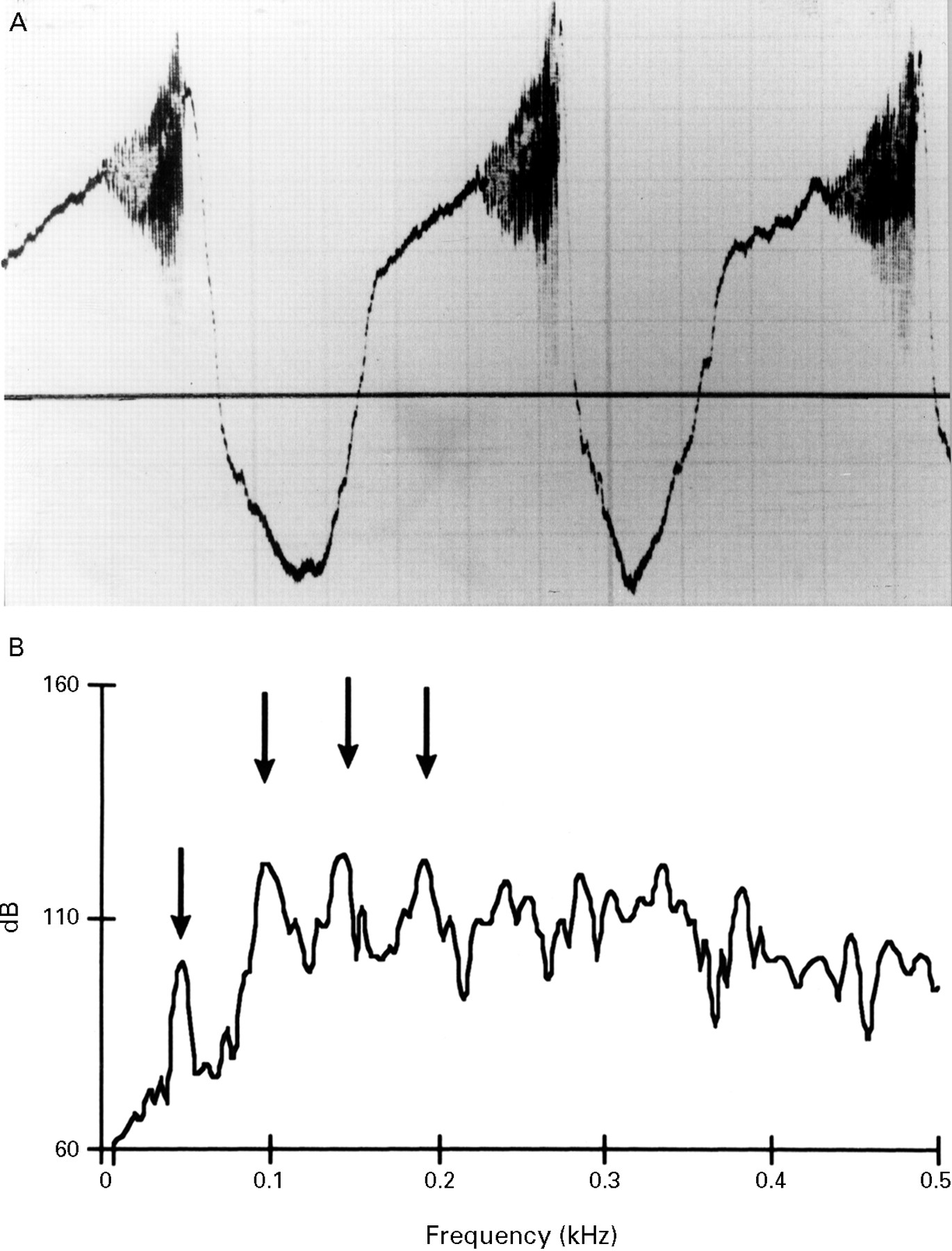
A flow-volume loop showed attenuation most marked in the expiratory limb (PEFR 0.8 l/s, PIFR 1.86 l/s). The overall pattern of the flow-volume envelope was characteristic of major airway intrathoracic obstruction.2 When superimposed, the tidal and maximal expiratory envelopes coincided suggesting that global airflow limitation had occurred during tidal breathing. An obvious saw tooth oscillation with a frequency of approximately 50 Hz, occurring at the same time as the low pitched expiratory sound, was also present on the expiratory limb of the flow trace (fig 1A).
{kind=link}
(A) Flow tracing (zero flow marked by the horizontal line; inspiration is in an upward direction and expiration is in a downward direction). Note the onset of oscillations on the expiratory limb which coincided with the low pitched sound. (B) Power spectrum of the expiratory sound, frequency in kHz on the horizontal axis and power in dB on the vertical axis. The arrows point to the peaks of energy (harmonics). The first arrow on the left points to the fundamental frequency of the sound at 48 Hz and the subsequent three arrows to the harmonics. Note that each harmonic is spaced 48 Hz apart.
Fibreoptic bronchoscopy under local anaesthetic revealed tracheobronchomalacia, the trachea, lobar and segmental bronchi collapsing on expiration with the anterior and posterior walls touching on forced manoeuvres. There were no abnormalities of the ear lobes, nose or joints to suggest that the cause of the tracheomalacia was due to relapsing polychondritis.
A recording of the sound was made using an air coupled electret condenser microphone (Monacor, ECM-2002, Radioshack; free field frequency response in air 50–16 000 Hz) placed on the upper right anterior chest wall. The sound was recorded onto magnetic tape using a frequency modulated (FM) tape recorder (Store 7D, Racal Electronics, Southampton, UK). Simultaneously, flow measured by a Fleisch no. 3 pneumotachograph was recorded onto a second channel. The recorded sounds were low pass filtered by a fourth order active Butterworth-type analogue filter with cut off frequency of 1.6 kHz and digitised at a sampling rate of 4 kHz with a 12 bit analogue to digital converter. Overlapping 128 point (32 ms) segments were spectrally analysed using a Fast Fourier Transforms (FFT) algorithm with a Hanning window (Ultra Digital Systems, C3M, interfaced to an IBM PC compatible computer).
Ten randomly chosen expiratory sounds were analysed and displayed as a three dimensional colour spectrogram and a power spectral plot. The spectrogram showed that the sound started abruptly with five or six high energy harmonic components spaced 48 Hz apart. The harmonic components fell by approximately 10 Hz during expiration. Figure 1B shows the corresponding power spectral plot (power in decibels against frequency in kHz). The distinct harmonic peaks (which are marked by arrows) are clearly seen, the first at 48 Hz (0.048 kHz) is the fundamental frequency and the subsequent peaks all spaced 48 Hz apart are harmonics (the fundamental frequency is always equal to the frequency difference between the harmonic peaks).
The patient subsequently had multiple admissions to hospital with increased dyspnoea and sputum production, usually precipitated by infection. Ten years after her first presentation she died in acute respiratory failure precipitated by bronchopneumonia.
Post-mortem examination revealed narrowing of the trachea (circumference 2.8 cm) and both main bronchi (internal diameter of the left main bronchus was 2 mm). The right lower lobe bronchi showed mucus plugging and bronchiectasis. Much of the cartilage had been destroyed and replaced with fibrous tissue; histological examination of the surviving cartilage showed a low grade lymphocytic and plasma cell infiltration, diagnostic of relapsing polychondritis.
Discussion
This patient’s initial clinical presentation with severe airflow obstruction was thought to be due to asthma. However, poor reversibility to bronchodilators and the presence of an unusual low pitched expiratory sound raised doubts about the diagnosis and bronchoscopic examination revealed the presence of severe tracheobronchomalacia of unknown aetiology. At the time there was no evidence of generalised cartilaginous disease, the diagnosis of relapsing polychondritis being made after death. Respiratory tract involvement with polychondritis has been reported to occur in 56% of cases but in only 14% is it the initial presenting symptom.3 In this case even after 10 years the disease remained limited to the chest.
Relatively little is known about the production of wheezing sounds. Gavriely and co-workers, using mathematical models4 and observing flow in flexible tubes,5 6 have demonstrated that wheeze is due to a complex interrelationship between the fluid and elastic forces inducing airway wall flutter at a flow-limiting segment. The thicker and wider the tube the lower the pitch of the wheezing sound. In methacholine induced wheezing in asthmatic subjects the association of expiratory wheezing with tidal airflow limitation has recently been confirmed7 and, as predicted by Gavriely’s model, the pitch of the wheeze fell during expiration as the geometry of the airway changed.
In this case the sound corresponded to oscillations in the flow tracing and suggests that airflow was clearly linked to the sound production. The multiple harmonic components seen in the spectrograph and power spectrum of the sound (fig 1B) were similar to the analysis of flutter in flow limited floppy tubes.5 Although airflow limitation does not usually occur in the trachea, in this case the lack of tracheal support was obvious at bronchoscopy and in these unusual circumstances airflow limitation at the level of the trachea is possible. The fundamental frequency of this expiratory sound was 48 Hz so it was not a wheeze (defined as having power peaks above 200 Hz8). However, the frequency of any “wheezing sound” is inversely related to the calibre of the airway producing the sound,4 suggesting that the sound was produced in a large airway such as the trachea. Furthermore, the dynamic nature of the sound, falling in pitch during expiration as the geometry of the trachea changes, is similar to the finding described during expiration in asthmatic wheezing.7
In this patient relapsing polychondritis resulted in a floppy trachea and produced a unique set of circumstances which allowed insights into the mechanism of dynamic flutter and wheeze production. This is the first time that a low pitched fluttering sound has been reported in association with tracheomalacia. It was the sound that suggested an alternative diagnosis and this may prove to be a useful physical sign in the diagnosis of tracheomalacia.